Download as pdf or txt
You might also like
- Architectural Thesis Synopsis-Health Resort Pt.Document2 pagesArchitectural Thesis Synopsis-Health Resort Pt.Priyanka75% (4)
- Detailed Lesson Plan in HOPE 3 Module 2 L. ObjectivesDocument8 pagesDetailed Lesson Plan in HOPE 3 Module 2 L. ObjectivesJarnel CabalsaNo ratings yet
- Coma, Hyperthermia and Bleeding Associated With Massive LSD OverdoseDocument6 pagesComa, Hyperthermia and Bleeding Associated With Massive LSD Overdose0j1u9nmkv534vw9vNo ratings yet
- Holze 2022 Ok - Excluir Repetido Holze 2023Document8 pagesHolze 2022 Ok - Excluir Repetido Holze 2023Ramiro Manzano NúñezNo ratings yet
- Assessment of Early Morning Serum Cortisol Levels in - 2022 - Medical Journal ADocument7 pagesAssessment of Early Morning Serum Cortisol Levels in - 2022 - Medical Journal AAnisha RanaNo ratings yet
- Longevity Effect of Liuwei Dihuang in Both: Caenorhabditis Elegans and Aged MiceDocument14 pagesLongevity Effect of Liuwei Dihuang in Both: Caenorhabditis Elegans and Aged Micemeltwithsnow163.comNo ratings yet
- Risperidona e Dano RenalDocument10 pagesRisperidona e Dano RenalRegina Souza AiresNo ratings yet
- Jurnal JiwaDocument11 pagesJurnal JiwaBasudewo AgungNo ratings yet
- Westermann 2004 2 PDFDocument14 pagesWestermann 2004 2 PDFfissionmailedNo ratings yet
- Eli GardDocument7 pagesEli GardthanaNo ratings yet
- Journal of Schizophrenia ResearchDocument8 pagesJournal of Schizophrenia ResearchAustin Publishing GroupNo ratings yet
- Influence of Salidroside, A Neuroactive Compound of in Rats: Rhodiola Rosea L., On Alcohol Tolerance DevelopmentDocument14 pagesInfluence of Salidroside, A Neuroactive Compound of in Rats: Rhodiola Rosea L., On Alcohol Tolerance DevelopmentGolanNo ratings yet
- Blood Pressure, Heart Rate, and Urinary Catecholamines inDocument9 pagesBlood Pressure, Heart Rate, and Urinary Catecholamines inJoão Marcel CamargoNo ratings yet
- Holze 2023Document10 pagesHolze 2023Ramiro Manzano NúñezNo ratings yet
- 2024 03 11 24304098v1 FullDocument17 pages2024 03 11 24304098v1 FullpyjirbfmpektdpprtmNo ratings yet
- Clinical Pharmacology of Methadone in DogsDocument9 pagesClinical Pharmacology of Methadone in Dogscarolinemsilva1No ratings yet
- Biomolecules 10 00279 v2Document8 pagesBiomolecules 10 00279 v2Róbson BatistaNo ratings yet
- Research Article: Laleh Farokhmehr, Hesameddin Modir, Bijan Yazdi, Alireza Kamali, Amir Almasi-HashianiDocument7 pagesResearch Article: Laleh Farokhmehr, Hesameddin Modir, Bijan Yazdi, Alireza Kamali, Amir Almasi-HashianiAndhika DNo ratings yet
- Description of Reference Ranges for Organic Acids in Urine مهمDocument11 pagesDescription of Reference Ranges for Organic Acids in Urine مهمfarkad rawiNo ratings yet
- The Effect of Storage Conditions On Sample Stability in The Routine Clinical LaboratoryDocument5 pagesThe Effect of Storage Conditions On Sample Stability in The Routine Clinical LaboratorysidomoyoNo ratings yet
- Research ArticleDocument8 pagesResearch ArticleelinNo ratings yet
- Jfda 27 01 323Document9 pagesJfda 27 01 323Mohamed Medhat AliNo ratings yet
- Jurnal Amlodipin UdtDocument7 pagesJurnal Amlodipin UdtdidiisafitriNo ratings yet
- High Plasma Oxytocin Levels in Men With Hypersexual DisorderDocument7 pagesHigh Plasma Oxytocin Levels in Men With Hypersexual DisorderboxeritoNo ratings yet
- Preclinical Acute Toxicity Studies and Rodent-Based Dosimetry Estimates of The Novel Sigma-1 Receptor Radiotracer (F) FPSDocument13 pagesPreclinical Acute Toxicity Studies and Rodent-Based Dosimetry Estimates of The Novel Sigma-1 Receptor Radiotracer (F) FPSirfanjadoonNo ratings yet
- 5 PharmacologyDocument4 pages5 Pharmacologyshiv_prhNo ratings yet
- Models of HypertensionDocument15 pagesModels of HypertensionAnant KhotNo ratings yet
- A Case of Severe Hypertriglyceridaemia and HypercholesterolaemiaDocument1 pageA Case of Severe Hypertriglyceridaemia and Hypercholesterolaemiathys2000No ratings yet
- S Venner Holm 1964Document17 pagesS Venner Holm 1964vsvsuresh2099No ratings yet
- Olanzapine-Induced Renal Damages and Metabolic Side Effects: The Protective Effects of ThymoquinoneDocument6 pagesOlanzapine-Induced Renal Damages and Metabolic Side Effects: The Protective Effects of ThymoquinonezainNo ratings yet
- The Effect of Aloin in Blood Glucose and Antioxidants in Male Albino Rats With Streptozotocin-Induced DiabeticDocument18 pagesThe Effect of Aloin in Blood Glucose and Antioxidants in Male Albino Rats With Streptozotocin-Induced DiabeticJunaid MinhasNo ratings yet
- Metabolic StressDocument3 pagesMetabolic StressRoberto MartineNo ratings yet
- Assessment of Antidiabetic Effect of 4-HIL in Type 2 Diabetic and Healthy Sprague Dawley RatsDocument11 pagesAssessment of Antidiabetic Effect of 4-HIL in Type 2 Diabetic and Healthy Sprague Dawley RatsMaxin BangsalNo ratings yet
- Yagyopathy: Applications of Yajna For Healing Amidst The Fascinating AchievementsDocument21 pagesYagyopathy: Applications of Yajna For Healing Amidst The Fascinating AchievementsNamrata75100% (1)
- Antinuclear Antibodies by Indirect Immunofluorescence: Optimum Screening Dilution For Diagnosis of Systemic Lupus ErythematosusDocument5 pagesAntinuclear Antibodies by Indirect Immunofluorescence: Optimum Screening Dilution For Diagnosis of Systemic Lupus ErythematosusMargriet MayasinNo ratings yet
- Art - 253A10.1007 - 252Fs40262 017 0513 9Document12 pagesArt - 253A10.1007 - 252Fs40262 017 0513 9galaxy.victorNo ratings yet
- Pier Vincenzo Piazza Et Al - Glucocorticoids Have State-Dependent Stimulant Effects On The Mesencephalic Dopaminergic TransmissionDocument5 pagesPier Vincenzo Piazza Et Al - Glucocorticoids Have State-Dependent Stimulant Effects On The Mesencephalic Dopaminergic TransmissionSour60No ratings yet
- Oxygenation Response in Experimental Diabetic Retinopathy: - Lipoic Acid Corrects Late-Phase Supernormal RetinalDocument6 pagesOxygenation Response in Experimental Diabetic Retinopathy: - Lipoic Acid Corrects Late-Phase Supernormal RetinalmagreaNo ratings yet
- 1 s2.0 S0014299916304800 MainDocument10 pages1 s2.0 S0014299916304800 MainlypemenosdiogenesNo ratings yet
- The Effect of Hetastarch (670/0.75) in Vivo On Platelet Closure Time in The DogDocument6 pagesThe Effect of Hetastarch (670/0.75) in Vivo On Platelet Closure Time in The DogsoledadDC329No ratings yet
- Full Mud Bath - Autonomic Variables - Healthy Volunteers - Dr. GnanadeepDocument7 pagesFull Mud Bath - Autonomic Variables - Healthy Volunteers - Dr. Gnanadeepsangu malar selvanNo ratings yet
- Population Pharmacokinetics of Intravenous Valproic Acid in Korean PatientsDocument7 pagesPopulation Pharmacokinetics of Intravenous Valproic Acid in Korean PatientsNoval ZulfikarNo ratings yet
- Kroboth 2003Document4 pagesKroboth 2003egrdfgNo ratings yet
- Article (1) - 2001 - Ponizovsky Et Al., 'Phospholipid Patterns in Schizophrenia... ' Schizophr ResDocument6 pagesArticle (1) - 2001 - Ponizovsky Et Al., 'Phospholipid Patterns in Schizophrenia... ' Schizophr Resshimonl3892No ratings yet
- 1 s2.0 S1018364717301052 MainDocument5 pages1 s2.0 S1018364717301052 Mainreza.scienceloverNo ratings yet
- Selenium and Leptin Levels in Febrile Seizure: A Case-Control Study in ChildrenDocument6 pagesSelenium and Leptin Levels in Febrile Seizure: A Case-Control Study in ChildrenDyah Gaby KesumaNo ratings yet
- Concentration-Response Relationships: Salicylate-Induced Ototoxicity VolunteersDocument8 pagesConcentration-Response Relationships: Salicylate-Induced Ototoxicity VolunteersAfnan AlkaffNo ratings yet
- Jurnal LisinoprilDocument7 pagesJurnal LisinoprildidiisafitriNo ratings yet
- Comparative in Vitro Dissolution and in Vivo Bioequivalence of Two Diclofenac Enteric Coated FormulationsDocument5 pagesComparative in Vitro Dissolution and in Vivo Bioequivalence of Two Diclofenac Enteric Coated FormulationsgeoaislaNo ratings yet
- Estudio Sobre DiabetesDocument5 pagesEstudio Sobre DiabetesGloria María De León MancillasNo ratings yet
- Drug Interaction HT and DMDocument6 pagesDrug Interaction HT and DMAfief Izuddin MhsNo ratings yet
- A Randomized Trial of Two Different Doses of A SHR-5 of Capacity For Mental WorkDocument11 pagesA Randomized Trial of Two Different Doses of A SHR-5 of Capacity For Mental WorkMARIBELNo ratings yet
- Studies On The Effects of Polydextrose Intake On Physiologic Functions in Chinese PeopleDocument7 pagesStudies On The Effects of Polydextrose Intake On Physiologic Functions in Chinese PeopleNhung Nguyễn Thị HồngNo ratings yet
- Journal of Neurochemistry - 2016 - Jalewa - Novel Incretin Analogues Improve Autophagy and Protect From MitochondrialDocument13 pagesJournal of Neurochemistry - 2016 - Jalewa - Novel Incretin Analogues Improve Autophagy and Protect From Mitochondrialjalewa.jaishreeNo ratings yet
- 1519 FullDocument6 pages1519 Fullpharmas1114No ratings yet
- Berner T 2007Document8 pagesBerner T 2007lorena091186No ratings yet
- Effect of Cs-4 (Cordyceps Sinensis) On Exercise Performance in Healthy Older Subjects: A Double-Blind, Placebo-Controlled TrialDocument6 pagesEffect of Cs-4 (Cordyceps Sinensis) On Exercise Performance in Healthy Older Subjects: A Double-Blind, Placebo-Controlled TrialRodas 108No ratings yet
- Rummel Kluge2010Document9 pagesRummel Kluge2010Ai Hwa LimNo ratings yet
- Aya Psychopharmacology 2011Document15 pagesAya Psychopharmacology 2011theendofthelineNo ratings yet
- 1026 FullDocument5 pages1026 FullMuhammad Yufimar Rizza FadilahNo ratings yet
- Bioequivalence Study of Two Formulations of Bisoprolol Fumarate Tablets in Healthy SubjectsDocument7 pagesBioequivalence Study of Two Formulations of Bisoprolol Fumarate Tablets in Healthy SubjectsSan-Clin-Eq LaboratoryNo ratings yet
- Milk PH As A Function of CO2 Concentration, Temperature, and Pressure in A Heat ExchangerDocument9 pagesMilk PH As A Function of CO2 Concentration, Temperature, and Pressure in A Heat ExchangerasdadasdasNo ratings yet
- The Impact of Intelligence On Memory and Executive Functions of Children With Temporal Lobe Epilepsy-Methodological Concerns With Clinical RelevanceDocument27 pagesThe Impact of Intelligence On Memory and Executive Functions of Children With Temporal Lobe Epilepsy-Methodological Concerns With Clinical RelevanceasdadasdasNo ratings yet
- WMS-III Performance in Patients With Temporal Lobe Epilepsy-Group Differences and Individual ClassificationDocument11 pagesWMS-III Performance in Patients With Temporal Lobe Epilepsy-Group Differences and Individual ClassificationasdadasdasNo ratings yet
- Identification of New NBOH Drugs in Seized Blotter Papers - 25B-NBOH, 25C-NBOH, and 25E-NBOHDocument13 pagesIdentification of New NBOH Drugs in Seized Blotter Papers - 25B-NBOH, 25C-NBOH, and 25E-NBOHasdadasdasNo ratings yet
- Brochure XGENIA ENGDocument2 pagesBrochure XGENIA ENGTaherNo ratings yet
- 8 September Morning Surgery and Allied 2017Document25 pages8 September Morning Surgery and Allied 2017Asma SaleemNo ratings yet
- Chrome Galvanize - AerosolDocument1 pageChrome Galvanize - AerosolJodyNo ratings yet
- Crestone Updated Draft Operator AgreementDocument21 pagesCrestone Updated Draft Operator AgreementJulie BaxterNo ratings yet
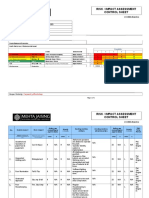
- Risk / Impact Assessment Control Sheet: CC/EHS/RA/014 ContractDocument4 pagesRisk / Impact Assessment Control Sheet: CC/EHS/RA/014 Contractsaurabh juwatkarNo ratings yet
- Gudisan Activity 1Document3 pagesGudisan Activity 1Filbs GudisanNo ratings yet
- First Aid BookletDocument37 pagesFirst Aid BookletLeNo ratings yet
- The Political Economy of Growth-Democracy and Human CapitalDocument15 pagesThe Political Economy of Growth-Democracy and Human CapitalArchietasari NindyamurtiNo ratings yet
- Nursing Care PlanDocument12 pagesNursing Care Plantzichi80% (5)
- Fasting For Fat LossDocument43 pagesFasting For Fat LossGordonReader8100% (2)
- Garces PsychDocument2 pagesGarces PsychSherlyn Miranda GarcesNo ratings yet
- Let It Snow (November 2022)Document16 pagesLet It Snow (November 2022)Watertown Daily TimesNo ratings yet
- 【加CE】出口 - 生化试剂 - N-乙酰-β-D-氨基葡萄糖苷酶试剂盒 NAG - 说明书 - 英文 - 1030316 - 2018.11.23Document3 pages【加CE】出口 - 生化试剂 - N-乙酰-β-D-氨基葡萄糖苷酶试剂盒 NAG - 说明书 - 英文 - 1030316 - 2018.11.23Abdul HameedNo ratings yet
- Report On Square LTDDocument12 pagesReport On Square LTDNazmulHasanNo ratings yet
- Injury Statistics SheetDocument4 pagesInjury Statistics SheetEslam IsmaeelNo ratings yet
- Food Safety BrazilDocument10 pagesFood Safety BrazilAdil KaukabNo ratings yet
- Updated Paternity and Maternity Leave W - ExerciseDocument20 pagesUpdated Paternity and Maternity Leave W - ExerciseNielle BautistaNo ratings yet
- Eng8 Q4 Mod1Document25 pagesEng8 Q4 Mod1Janine Loresco-FernandezNo ratings yet
- Face Process of Interacting That Focuses On Advancing The Physical and Emotional Well-Being of A PatientDocument8 pagesFace Process of Interacting That Focuses On Advancing The Physical and Emotional Well-Being of A PatientJanray CalunsodNo ratings yet
- Iota AdnexDocument10 pagesIota Adnexlinh hoàngNo ratings yet
- AIIMS Jodhpur Juniour Residents NoticeDocument4 pagesAIIMS Jodhpur Juniour Residents NoticeVijaya sharmaNo ratings yet
- Ch. 7 Control of Microbial GrowthDocument10 pagesCh. 7 Control of Microbial GrowthYousef DosouqiNo ratings yet
- BurnsDocument31 pagesBurnsLouis Carlos RoderosNo ratings yet
- Mock Test 176Document4 pagesMock Test 176Ngan Nguyen PhuongNo ratings yet
- Laparoscopic Splenectomy For Pediatric Wandering Spleen - A Case ReportDocument11 pagesLaparoscopic Splenectomy For Pediatric Wandering Spleen - A Case ReportAdlyn Bea Albesa-BernaldezNo ratings yet
- ThyroidectomyDocument3 pagesThyroidectomyhahahahaaaaaaaNo ratings yet
- Diabetes Final Research EssayDocument13 pagesDiabetes Final Research Essayapi-549030089No ratings yet
- CSL Recruitment 2024Document11 pagesCSL Recruitment 2024Chitikala RajeshNo ratings yet