Download as pdf or txt
You might also like
- Ward Round ProformaDocument2 pagesWard Round ProformaAnonymous no7EOvHlNo ratings yet
- Nursing Care Plan-AscitesDocument10 pagesNursing Care Plan-AscitesKayki Louise75% (4)
- Aboriginal Hypertension Brochure Resource PDFDocument2 pagesAboriginal Hypertension Brochure Resource PDFRickNo ratings yet
- Vivaldi Oboe Concerto in A Minor (RV463)Document14 pagesVivaldi Oboe Concerto in A Minor (RV463)Amín CarrilloNo ratings yet
- Massive Pulmonary EmbolismDocument3 pagesMassive Pulmonary Embolismnananana123No ratings yet
- RT-PCR ReportDocument1 pageRT-PCR ReportAnuj SharmaNo ratings yet
- Vaccine MemosDocument13 pagesVaccine MemosThe Daily OrangeNo ratings yet
- New Idaho Vaccine Exemption FormDocument2 pagesNew Idaho Vaccine Exemption FormDonnaNo ratings yet
- Discromatie Test 38Document13 pagesDiscromatie Test 38nelutza_popNo ratings yet
- Immunity Worksheet PDFDocument3 pagesImmunity Worksheet PDFCrayolaConsumer Sumer100% (1)
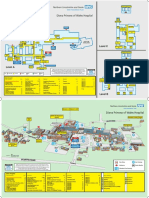
- Diana Princess of Wales Hospital: Level CDocument2 pagesDiana Princess of Wales Hospital: Level CTeamkamal FillahNo ratings yet
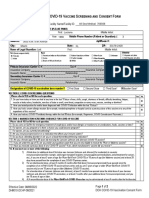
- Covid-19 Vaccine Screening and Consent Form Pfizer-Biontech Covid-19 VaccineDocument2 pagesCovid-19 Vaccine Screening and Consent Form Pfizer-Biontech Covid-19 Vaccinesiriamma wiliamsNo ratings yet
- BivalentConsent MichaelBelen HAG322426Document2 pagesBivalentConsent MichaelBelen HAG322426michaeljohnbelen14No ratings yet
- BivalentConsent LucianaPedrosopessoa 559154Document2 pagesBivalentConsent LucianaPedrosopessoa 559154Tatah SouzaNo ratings yet
- COVID-19 Vax Consent FormDocument3 pagesCOVID-19 Vax Consent FormCj CCNo ratings yet
- Informed Consent UniversalDocument1 pageInformed Consent Universalahasgahsg031No ratings yet
- Vaccine Administration Record (VAR) - Informed Consent For VaccinationDocument2 pagesVaccine Administration Record (VAR) - Informed Consent For VaccinationHilda LunaNo ratings yet
- Walgreens VAR FormDocument2 pagesWalgreens VAR FormZubaer RahmanNo ratings yet
- COVID-19 Vaccination Consent Form: Basic Info: First Tell Us Who You AreDocument2 pagesCOVID-19 Vaccination Consent Form: Basic Info: First Tell Us Who You AreVAS skytelNo ratings yet
- Covid-19 Vaccine Consent Form: Information About Person To Receive Vaccine (Please Print)Document2 pagesCovid-19 Vaccine Consent Form: Information About Person To Receive Vaccine (Please Print)Karylle PetilNo ratings yet
- Medical QuestionnaireDocument2 pagesMedical QuestionnaireKunal GuptaNo ratings yet
- Walgreens Community VAR ENGDocument2 pagesWalgreens Community VAR ENGRhea BayabanNo ratings yet
- Covid 19 Vaccination Consent Form For Covid 19 Vaccination Covid 19 Vaccination Consent Form - 1Document6 pagesCovid 19 Vaccination Consent Form For Covid 19 Vaccination Covid 19 Vaccination Consent Form - 1Stephanie BewleyNo ratings yet
- Consent Form - Pfizer-Biontech Covid-19 VaccineDocument2 pagesConsent Form - Pfizer-Biontech Covid-19 VaccineRommel Bucasas GarciaNo ratings yet
- FINAL COVID-19 Vaccine Consent Form Inc. FDA Eua and ACIP 12.13.2020Document2 pagesFINAL COVID-19 Vaccine Consent Form Inc. FDA Eua and ACIP 12.13.2020Natasa PrelevicNo ratings yet
- Consentimiento CovidDocument2 pagesConsentimiento CovidAlexis G. MamaniNo ratings yet
- Covid 19 Vaccination Consent Form For Covid 19 Vaccination Covid 19 Vaccination Consent Form - 1Document4 pagesCovid 19 Vaccination Consent Form For Covid 19 Vaccination Covid 19 Vaccination Consent Form - 1bersabeh abayNo ratings yet
- Covid 19 Vaccination Consent Form For Covid 19 Vaccination Covid 19 Vaccination Consent Form 2Document7 pagesCovid 19 Vaccination Consent Form For Covid 19 Vaccination Covid 19 Vaccination Consent Form 2Erich PirnkeNo ratings yet
- Screening QuestionnaireDocument2 pagesScreening QuestionnaireKarina RojasNo ratings yet
- COVID 19 Consent FormDocument2 pagesCOVID 19 Consent FormfvdssfdNo ratings yet
- Pfizer Screen Consent Form PrintDocument2 pagesPfizer Screen Consent Form Printp. wsmNo ratings yet
- Basics FsDocument2 pagesBasics FsRomeo TevesNo ratings yet
- Pfizer Consent Form - FillableDocument8 pagesPfizer Consent Form - FillableAbraham Baeza - Viajes PegüisNo ratings yet
- CONSENT FORM - COVID-19 VaccineDocument5 pagesCONSENT FORM - COVID-19 Vaccinebersabeh abayNo ratings yet
- DOH - Covid Vaccine Screening Consent FormDocument2 pagesDOH - Covid Vaccine Screening Consent FormCasey Feindt100% (1)
- COVID Safe PlanDocument9 pagesCOVID Safe PlanskubalaspamNo ratings yet
- COVD 19 Vaction Form 2020 Pfizerv2Document1 pageCOVD 19 Vaction Form 2020 Pfizerv2Neel YoyoNo ratings yet
- Condado de Los Ángeles: Vacunas Contra El Covid-19-Preguntas Frecuentes (Faq)Document16 pagesCondado de Los Ángeles: Vacunas Contra El Covid-19-Preguntas Frecuentes (Faq)Shakira MonqueNo ratings yet
- Eapps Health StartDocument6 pagesEapps Health StartRegine CaspilloNo ratings yet
- Useless Documents Because I Wanted To Download A File and They Asked Me To Upload 5 Documents.Document2 pagesUseless Documents Because I Wanted To Download A File and They Asked Me To Upload 5 Documents.Harsh MehtaNo ratings yet
- QC Protektodo Forms Sinopharm 1st Dose AranetaDocument3 pagesQC Protektodo Forms Sinopharm 1st Dose AranetaRalph Clinton PalomenoNo ratings yet
- Patient Registration Packet For COVID Vaccine 1.19.2021Document3 pagesPatient Registration Packet For COVID Vaccine 1.19.2021Revengie CunalibanNo ratings yet
- Preparing For COVID-19 Vaccination: Make Sure Your Details Are CorrectDocument3 pagesPreparing For COVID-19 Vaccination: Make Sure Your Details Are CorrectPhan Huu Anh TuanNo ratings yet
- New Hire Medical Checklist 4.27.12Document6 pagesNew Hire Medical Checklist 4.27.12Mark Aaron WilsonNo ratings yet
- Vaccine Cluster - Health Screening FormDocument3 pagesVaccine Cluster - Health Screening FormArlene AngelesNo ratings yet
- Formular Za Pristanak Na Cijepljenje Na FloridiDocument2 pagesFormular Za Pristanak Na Cijepljenje Na FloridiIndex.hrNo ratings yet
- YL Camping Consent and Health FormDocument4 pagesYL Camping Consent and Health Formmcronin1970No ratings yet
- COVID-19 Vaccine Consent FormDocument5 pagesCOVID-19 Vaccine Consent FormSiamakNo ratings yet
- Hi 58723057234Document2 pagesHi 58723057234NofoNo ratings yet
- Golden Eagle Final Expense Application FBLICDocument7 pagesGolden Eagle Final Expense Application FBLICDen NisNo ratings yet
- Covid Questionnaire FormDocument2 pagesCovid Questionnaire FormtaguikenzoNo ratings yet
- Pfizer Informed Consent Form Eng - April 15 2021Document1 pagePfizer Informed Consent Form Eng - April 15 2021Christie ConalesNo ratings yet
- Public FAQDocument15 pagesPublic FAQIan WeberNo ratings yet
- Pacifc MMI Application Form PDFDocument6 pagesPacifc MMI Application Form PDFKaitaMahnNo ratings yet
- Declaration of Good Heath: Ddmmy YYYDocument2 pagesDeclaration of Good Heath: Ddmmy YYYindu chauhanNo ratings yet
- CDC Vaccine FactsDocument6 pagesCDC Vaccine Facts13WMAZNo ratings yet
- Frequently Asked Questions About COVID-19 Vaccines For Families and EducatorsDocument2 pagesFrequently Asked Questions About COVID-19 Vaccines For Families and EducatorsLizzie Hernández-CarrizalesNo ratings yet
- Covid19vaccineconsentform UpdatedDocument2 pagesCovid19vaccineconsentform UpdatedGlenn ReinhardtNo ratings yet
- Moderna (Health Declaration Screening Form) Eng - June 18 2021Document1 pageModerna (Health Declaration Screening Form) Eng - June 18 2021Paulo Justin Tabangcora OropillaNo ratings yet
- Pfizer Health Declaration Screening Form Eng June 9 2021Document1 pagePfizer Health Declaration Screening Form Eng June 9 2021Kim GomezNo ratings yet
- Nonmedical Exemption FormDocument1 pageNonmedical Exemption FormSupreme Understanding DassNo ratings yet
- Vaccine ExemptionVacLib GeorgiaDocument2 pagesVaccine ExemptionVacLib GeorgiaDonnaNo ratings yet
- COVID-19 Vaccines: Third Dose For People Who Are ImmunocompromisedDocument2 pagesCOVID-19 Vaccines: Third Dose For People Who Are ImmunocompromisedBaltazar BonillaNo ratings yet
- Fieldtrip Dietary Medical Questionnaire NHMDocument2 pagesFieldtrip Dietary Medical Questionnaire NHMAna LarrabeitiNo ratings yet
- Youth Ministries Medical and Liability Release Kayaking Trip August 10Document4 pagesYouth Ministries Medical and Liability Release Kayaking Trip August 10DiaanNo ratings yet
- Fighting Covid-19: The Unequal Opportunity Killer: You Are Not Helpless in the Face of the Covid-19 EpidemicFrom EverandFighting Covid-19: The Unequal Opportunity Killer: You Are Not Helpless in the Face of the Covid-19 EpidemicNo ratings yet
- Analysis Prokofiev Flute Sonata PDFDocument2 pagesAnalysis Prokofiev Flute Sonata PDFAmín CarrilloNo ratings yet
- Early in The MorningDocument2 pagesEarly in The MorningAmín CarrilloNo ratings yet
- Chamber Music Literature and Repertoire 2 FinalDocument7 pagesChamber Music Literature and Repertoire 2 FinalAmín CarrilloNo ratings yet
- Die MainachtDocument4 pagesDie MainachtAmín CarrilloNo ratings yet
- Finzi, Gerald - The SighDocument4 pagesFinzi, Gerald - The SighAmín CarrilloNo ratings yet
- Trade WindsDocument5 pagesTrade WindsAmín CarrilloNo ratings yet
- Hansel and Gretel With Cuts (2) - CompressedDocument115 pagesHansel and Gretel With Cuts (2) - CompressedAmín CarrilloNo ratings yet
- IMSLP481782 PMLP780817 Kuhlausonatinasforthepianovol - Iop.20no.1Document5 pagesIMSLP481782 PMLP780817 Kuhlausonatinasforthepianovol - Iop.20no.1Amín CarrilloNo ratings yet
- TTBPP 4-7Document4 pagesTTBPP 4-7Amín CarrilloNo ratings yet
- REDONE F Dimitri Shostakovich (1906-1975)Document6 pagesREDONE F Dimitri Shostakovich (1906-1975)Amín CarrilloNo ratings yet
- Wingell Herzog Chapter 1 Pg. 1-22Document12 pagesWingell Herzog Chapter 1 Pg. 1-22Amín CarrilloNo ratings yet
- Grades S22Document1 pageGrades S22Amín CarrilloNo ratings yet
- FileDocument83 pagesFileAmín CarrilloNo ratings yet
- Beethoven, Pianist. String PlayerDocument6 pagesBeethoven, Pianist. String PlayerAmín CarrilloNo ratings yet
- BookingconfirmationDocument2 pagesBookingconfirmationAmín CarrilloNo ratings yet
- Nikolay Rimsky-Korsakov (1844-1908)Document4 pagesNikolay Rimsky-Korsakov (1844-1908)Amín CarrilloNo ratings yet
- Joseph de Bologne Chevalier de Saint-Georges (1745-1799)Document8 pagesJoseph de Bologne Chevalier de Saint-Georges (1745-1799)Amín Carrillo100% (1)
- 2022 PMAHCC Foundation Rob Vega ScholarshipDocument6 pages2022 PMAHCC Foundation Rob Vega ScholarshipAmín CarrilloNo ratings yet
- 9620 - CLDocument9 pages9620 - CLAmín CarrilloNo ratings yet
- June 2022 Invoice: Amount Due by 15 JUL 2022Document3 pagesJune 2022 Invoice: Amount Due by 15 JUL 2022Amín CarrilloNo ratings yet
- Roots and BranchesDocument4 pagesRoots and BranchesAmín CarrilloNo ratings yet
- Family Planning Methods: Presented byDocument56 pagesFamily Planning Methods: Presented byNise Mon KuriakoseNo ratings yet
- Pharmacology Viva QuestionsDocument1 pagePharmacology Viva Questionsmaheen_ju100% (2)
- LEH 3-4A Chapter 22 1213Document33 pagesLEH 3-4A Chapter 22 1213ikaNo ratings yet
- ABSTRACT BOOK - FinalDocument79 pagesABSTRACT BOOK - FinalAlejandro XandirNo ratings yet
- A Special Interview With Dr. Daniel AmenDocument19 pagesA Special Interview With Dr. Daniel Amenzapperindia100% (1)
- Body Disease and Emotional Issues Two Pager 1Document2 pagesBody Disease and Emotional Issues Two Pager 1Color CrystalNo ratings yet
- 10 On 2020 HSCT WBDocument94 pages10 On 2020 HSCT WBabdullahNo ratings yet
- Daftar Pustaka 3Document8 pagesDaftar Pustaka 3Marsela Renasari PrestyNo ratings yet
- Shin LuluDocument2 pagesShin LuluEka HimawanNo ratings yet
- Endometriosis GuidelineDocument44 pagesEndometriosis GuidelineHen DriNo ratings yet
- nsg-430cc Care Plan 2Document10 pagesnsg-430cc Care Plan 2api-509452165No ratings yet
- Nbe Thesis ProtocolDocument8 pagesNbe Thesis Protocolsarahdavisjackson100% (2)
- Diagnosa Ri Dan Kode Ina CBGDocument7 pagesDiagnosa Ri Dan Kode Ina CBGUjang YayaNo ratings yet
- Orthodontics in 3 MillenniaDocument6 pagesOrthodontics in 3 MillenniamelovebeingmeNo ratings yet
- Dental InstrumentsDocument92 pagesDental InstrumentsGabriela Cocieru Motelica100% (1)
- Vol06 b2 32-33strDocument2 pagesVol06 b2 32-33strAyuAnggayantiNo ratings yet
- COVID 19 and DiabetesDocument3 pagesCOVID 19 and DiabetesAynun JMNo ratings yet
- PhlebotomyDocument5 pagesPhlebotomyFuture TrekingNo ratings yet
- Review On DIY Ventilator Using Arduino - Formatted PaperDocument3 pagesReview On DIY Ventilator Using Arduino - Formatted Paperrogergold199No ratings yet
- F.A.S.T.H.U.G: I W. AryabiantaraDocument35 pagesF.A.S.T.H.U.G: I W. Aryabiantaraarnawaiputu60No ratings yet
- Odontogenickeratocyst Clinically Mimicking Osteomyelitis - A Rare Case ReportDocument4 pagesOdontogenickeratocyst Clinically Mimicking Osteomyelitis - A Rare Case ReportInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- Chapter 6. The Circulatory System: Short QuestionsDocument31 pagesChapter 6. The Circulatory System: Short QuestionsParardha DharNo ratings yet