Download as pdf or txt
You might also like
- HLTWHS002 - HO - HLTWHS002-Follow Safe Work Practices For Direct Client CareDocument34 pagesHLTWHS002 - HO - HLTWHS002-Follow Safe Work Practices For Direct Client CareTalhaFarrukh67% (6)
- Mount Carmel Medication Management Pocket GuideDocument2 pagesMount Carmel Medication Management Pocket GuideWOSU100% (1)
- Case Study CholecystitisDocument27 pagesCase Study Cholecystitisyhanne98% (225)
- Spectrophotometric Determination of Paracetamol in Some Manufactured Tablets in Iraqi MarketsDocument6 pagesSpectrophotometric Determination of Paracetamol in Some Manufactured Tablets in Iraqi MarketsDella AfizahNo ratings yet
- Chemical Restraint in The Horse: CommissionedDocument5 pagesChemical Restraint in The Horse: CommissionedKristoandi PoettingNo ratings yet
- Pico Silver Ver 1 Oct 29 2019 FINALDocument36 pagesPico Silver Ver 1 Oct 29 2019 FINALCondor FiveNo ratings yet
- Ambrisentan: James E. FramptonDocument12 pagesAmbrisentan: James E. FramptonElden Kyle BillonesNo ratings yet
- Wellington 2001Document10 pagesWellington 2001Minas AliNo ratings yet
- Ambrisentan: Jamie D. Croxtall and Susan J. KeamDocument10 pagesAmbrisentan: Jamie D. Croxtall and Susan J. KeamElden Kyle BillonesNo ratings yet
- Evans1997 PDFDocument13 pagesEvans1997 PDFMonica LozanoNo ratings yet
- Pregabalina en El Tratamiento de Neuralgia PostherpeticaDocument10 pagesPregabalina en El Tratamiento de Neuralgia PostherpeticaPaula Andrea MeloNo ratings yet
- 211321Orig1s000ClinPharmR PDFDocument71 pages211321Orig1s000ClinPharmR PDFLay LylyNo ratings yet
- Evans 2003Document12 pagesEvans 2003Paula RoccaNo ratings yet
- Keam 2002Document13 pagesKeam 2002Minas AliNo ratings yet
- Side Effects of PhenytoinDocument5 pagesSide Effects of PhenytoinRaluca ElenaNo ratings yet
- Clinical Use of Aripiprazole in Patients With Schizophrenia - A Real-Life Setting Results From TheDocument8 pagesClinical Use of Aripiprazole in Patients With Schizophrenia - A Real-Life Setting Results From TheCristobal Velasquez MonardezNo ratings yet
- Advances in Feline AnesthesiaDocument5 pagesAdvances in Feline AnesthesiaMabe AguirreNo ratings yet
- Desvenlafaxina 2Document9 pagesDesvenlafaxina 2Robert MovileanuNo ratings yet
- Abatacept Hervey2006Document9 pagesAbatacept Hervey2006Calvin Tanuwijaya Stick BolaNo ratings yet
- 17ß-Estradiol Levonorgestrel TransdermalDocument7 pages17ß-Estradiol Levonorgestrel TransdermalLokesh KhuranaNo ratings yet
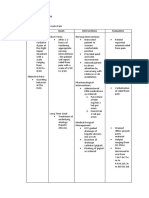
- Problem Goals Interventions EvaluationDocument5 pagesProblem Goals Interventions EvaluationJessa Mae TabladilloNo ratings yet
- Acute Pain Managemente - Scientific EvidenceDocument5 pagesAcute Pain Managemente - Scientific EvidenceSumroachNo ratings yet
- Esomeprazole: A N D PDocument9 pagesEsomeprazole: A N D PHadiNugrahaNo ratings yet
- Ketamine 1Document20 pagesKetamine 1fadil23No ratings yet
- Gabapentin Oi DesDocument11 pagesGabapentin Oi DesLuis Felipe Arteaga ArredondoNo ratings yet
- New Formulations of New AntidepressantsDocument16 pagesNew Formulations of New AntidepressantsGe NomNo ratings yet
- Green Focus Levomepromazina 2004Document5 pagesGreen Focus Levomepromazina 2004Psiquiatria Clinica ProyectarteNo ratings yet
- Design and in Vitro:in Vivo Evaluation of Extended Release Matrix Tablets of Nateglinide PDFDocument6 pagesDesign and in Vitro:in Vivo Evaluation of Extended Release Matrix Tablets of Nateglinide PDFDIKANo ratings yet
- Perioperative Applications of DexmedetomidineDocument8 pagesPerioperative Applications of Dexmedetomidinewen1190No ratings yet
- List of New Drugs Approved in The Year 2023decDocument4 pagesList of New Drugs Approved in The Year 2023decJassu J CNo ratings yet
- RemimazolamDocument9 pagesRemimazolammatheus galvãoNo ratings yet
- Cerenia InjectableDocument2 pagesCerenia InjectableRue BensonNo ratings yet
- Oral Ketamine in Treatment-Resistant Depression: Rief EportDocument4 pagesOral Ketamine in Treatment-Resistant Depression: Rief EportDeepaNo ratings yet
- Clinical Pharmacokinetics of Ibuprofen: The First 30 YearsDocument2 pagesClinical Pharmacokinetics of Ibuprofen: The First 30 YearsDwy AdyNo ratings yet
- Untitlednf Fli DJ Ig Tu JDocument30 pagesUntitlednf Fli DJ Ig Tu JBEST OF BESTNo ratings yet
- Topical Dorzolamide 2%/timolol 0.5% Ophthalmic SolutionDocument19 pagesTopical Dorzolamide 2%/timolol 0.5% Ophthalmic SolutionÇağla K.No ratings yet
- Long-Acting Injectable AntipsychoticsDocument18 pagesLong-Acting Injectable AntipsychoticsMia BlackattNo ratings yet
- Cat AnestheziaDocument9 pagesCat Anestheziataner_soysurenNo ratings yet
- Cabasis Drug StudyDocument3 pagesCabasis Drug StudyNick James CabasisNo ratings yet
- 2018 Top 5 Tips For Sedation & Anesthesia in Fractious DogsDocument6 pages2018 Top 5 Tips For Sedation & Anesthesia in Fractious DogsAdriele FernandesNo ratings yet
- Baldwin 2009Document9 pagesBaldwin 2009shahhareshNo ratings yet
- Clin Pharmacokinet 2001 40 8 573-85.pdffarmacocinetica SirolimusDocument13 pagesClin Pharmacokinet 2001 40 8 573-85.pdffarmacocinetica SirolimusMaria Marina Papaginovic LeivaNo ratings yet
- Dexmedetomidine: An Updated Review: Annals of Pharmacotherapy March 2007Document11 pagesDexmedetomidine: An Updated Review: Annals of Pharmacotherapy March 2007eriza amalia zainNo ratings yet
- Dexmedetomidine: An Updated Review: Annals of Pharmacotherapy March 2007Document11 pagesDexmedetomidine: An Updated Review: Annals of Pharmacotherapy March 2007eriza amalia zainNo ratings yet
- AN4 OA Sidharth-2Document6 pagesAN4 OA Sidharth-2Dede TarunaNo ratings yet
- JAMBALOS JERALDEEN BSN 4 2 DRUG STUDY FormatDocument3 pagesJAMBALOS JERALDEEN BSN 4 2 DRUG STUDY FormatJeraldeen JambalosNo ratings yet
- Week 7 Course TaskDocument13 pagesWeek 7 Course TaskRachelle CambaNo ratings yet
- II-118 High Alert Medications: PurposeDocument9 pagesII-118 High Alert Medications: PurposeAhmad Al-RusasiNo ratings yet
- 4 Anesthetic and Cardiopulmonary Effects of Butorphanol-Tiletamine-Zolazepam-Medetomidine and Tramadol-Tiletamine-Zolazepam-Medetomidine in DogsDocument7 pages4 Anesthetic and Cardiopulmonary Effects of Butorphanol-Tiletamine-Zolazepam-Medetomidine and Tramadol-Tiletamine-Zolazepam-Medetomidine in DogsRajesh KumarNo ratings yet
- Combined Alternative Meds MemoDocument62 pagesCombined Alternative Meds MemoFDRHPO North Country EMS Program AgencyNo ratings yet
- JPRHC: Research ArticleDocument9 pagesJPRHC: Research Articleabhijit_gothoskar6039No ratings yet
- AnalgesiaDocument43 pagesAnalgesiamiguelalmenarezNo ratings yet
- Quetiapina in SKDocument16 pagesQuetiapina in SKRobert MovileanuNo ratings yet
- The ABC's of Dopamine Receptor Partial Agonists - Aripiprazole, Brexpiprazole and CariprazineDocument10 pagesThe ABC's of Dopamine Receptor Partial Agonists - Aripiprazole, Brexpiprazole and Cariprazineolivukovic100% (1)
- Formulation and in Vitro Evaluation of Fesoterodine Fumarate Sustained Release TabletsDocument13 pagesFormulation and in Vitro Evaluation of Fesoterodine Fumarate Sustained Release TabletsBaru Chandrasekhar RaoNo ratings yet
- 9 Ketamine Drug StudyDocument7 pages9 Ketamine Drug Studyshadow gonzalezNo ratings yet
- Dex Review 2007Document11 pagesDex Review 2007Jackelyne VilelaNo ratings yet
- Journal Homepage: - : Manuscript HistoryDocument7 pagesJournal Homepage: - : Manuscript HistoryIJAR JOURNALNo ratings yet
- Partial Agonists2 of Dopamine Receptors Mechanisms and Clinical Effects of Aripiprazole Brexpiprazole and CariprazineDocument7 pagesPartial Agonists2 of Dopamine Receptors Mechanisms and Clinical Effects of Aripiprazole Brexpiprazole and CariprazineEsraa SaeedNo ratings yet
- DRUG StudyDocument43 pagesDRUG StudyNathalie Faith CotengNo ratings yet
- Literature 2 - Pregabalin Vs GabapentinDocument10 pagesLiterature 2 - Pregabalin Vs GabapentinKeke NechNo ratings yet
- Holliday 1995Document15 pagesHolliday 1995ronaldotimmNo ratings yet
- Liu Et Al, 2020Document4 pagesLiu Et Al, 2020adi suputraNo ratings yet
- Value Based Healthcare in SwitzerlandDocument90 pagesValue Based Healthcare in SwitzerlandJoel LehmannNo ratings yet
- Drug Administration Errors in Hospital Inpatients: A Systematic ReviewDocument11 pagesDrug Administration Errors in Hospital Inpatients: A Systematic ReviewPardon MeNo ratings yet
- Ijias 18 242 01Document6 pagesIjias 18 242 01Jude EmmanuelNo ratings yet
- BM PDFDocument6 pagesBM PDFrahmaNo ratings yet
- Evc Stroke State of Art 2020Document15 pagesEvc Stroke State of Art 2020marvin somozaNo ratings yet
- Gomez & Company: CharlesDocument7 pagesGomez & Company: Charlesheinfnfe3cxman29398No ratings yet
- The Effects of Active Break and Postural Shift Interventions On Recovery FromDocument8 pagesThe Effects of Active Break and Postural Shift Interventions On Recovery FromNiko TrogerNo ratings yet
- Diabetic Foot InfectionDocument40 pagesDiabetic Foot InfectionSuchie ILyasNo ratings yet
- Wound Care ManagementDocument44 pagesWound Care ManagementPrasanth BhujanNo ratings yet
- Research Paper Artificial Intelligence in Medical JEEV AI-IJRASETDocument8 pagesResearch Paper Artificial Intelligence in Medical JEEV AI-IJRASETIJRASETPublicationsNo ratings yet
- Clostridium Difficile Infection Fidaxomicin Esnm1Document11 pagesClostridium Difficile Infection Fidaxomicin Esnm1Pet UrNo ratings yet
- The New Parkland Hospital CampusDocument1 pageThe New Parkland Hospital CampusThe Dallas Morning NewsNo ratings yet
- Doctors Marketing Program FOR Organized Pharmacy Retail ChainDocument21 pagesDoctors Marketing Program FOR Organized Pharmacy Retail ChaindeepakashwaniNo ratings yet
- Kanu - Chatterjee Common - Problems in Cardiology PDFDocument332 pagesKanu - Chatterjee Common - Problems in Cardiology PDFSabyasachi MukhopadhyayNo ratings yet
- Silicon Induced LymphoafenopathyDocument5 pagesSilicon Induced LymphoafenopathyDiana RomanovaNo ratings yet
- Case Study of Stroke: Interprofessional Learning Maldives National University 26th October 2022Document43 pagesCase Study of Stroke: Interprofessional Learning Maldives National University 26th October 2022Riphu RashydNo ratings yet
- Kim 2021Document8 pagesKim 2021Arun AdhikariNo ratings yet
- GelpointDocument6 pagesGelpointnatalia mendozaNo ratings yet
- Medical Care On Board Ship and Ashore - Medical Chest, Recordkeeping and Responsibilities and Training For Medical Care MN-7-042-1 PDFDocument26 pagesMedical Care On Board Ship and Ashore - Medical Chest, Recordkeeping and Responsibilities and Training For Medical Care MN-7-042-1 PDFRamon Carlo AlmiranezNo ratings yet
- Medtech LawDocument16 pagesMedtech LawClaudine David0% (1)
- 35 - Eposter - Subhenjit Ray.Document1 page35 - Eposter - Subhenjit Ray.Subhenjit RoyNo ratings yet
- Topic 5 - Handbook of Medical Sociology Ch4 - 2Document23 pagesTopic 5 - Handbook of Medical Sociology Ch4 - 2AngellaNo ratings yet
- Appendix 4b - NIV Algorithm (ICHT)Document1 pageAppendix 4b - NIV Algorithm (ICHT)Josi JeremiaNo ratings yet
- Management of Chronic Hepatitis B in AdultsDocument76 pagesManagement of Chronic Hepatitis B in AdultsLan AllemNo ratings yet
- Wallenberg Syndrome: Publication DetailsDocument9 pagesWallenberg Syndrome: Publication DetailsHuang Jen Liang100% (1)
- Bee Venom CreamDocument2 pagesBee Venom CreamfabiandionisioNo ratings yet