Download as pdf or txt
You might also like
- Small Animal Cardiovascular Medicine PDFDocument1,832 pagesSmall Animal Cardiovascular Medicine PDFJordan Peters100% (1)
- Sexuality of Aging Adults A Case Study Using Narrative TherapyDocument9 pagesSexuality of Aging Adults A Case Study Using Narrative TherapyChristian RiveraNo ratings yet
- Rosenfield & Mouzon (2013) - Gender and Mental HealthDocument20 pagesRosenfield & Mouzon (2013) - Gender and Mental HealthAlejandro CNo ratings yet
- Brannon ch07Document27 pagesBrannon ch07Vlad EugenNo ratings yet
- Nihon Kohden Life Scope BSM 6000 SeriesDocument394 pagesNihon Kohden Life Scope BSM 6000 SeriesPavel Timotin60% (5)
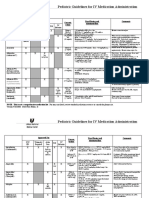
- Pediatric Guidelines For MedicationsDocument24 pagesPediatric Guidelines For MedicationsjonatasmartinezNo ratings yet
- Nelson 2016Document8 pagesNelson 2016Uzi SuruziNo ratings yet
- GBX 027Document11 pagesGBX 027one pieceNo ratings yet
- Loneliness in Older Women A Review of The LiteratureDocument20 pagesLoneliness in Older Women A Review of The LiteratureEdłardo Fłentes GonzálezNo ratings yet
- Life SatisfactionDocument15 pagesLife Satisfactionfernandez.s1299No ratings yet
- Counseling AgedDocument26 pagesCounseling AgedSalima HabeebNo ratings yet
- Ageism - We Are Our Own Worst Enemy - Kerry Sargent - CoxDocument8 pagesAgeism - We Are Our Own Worst Enemy - Kerry Sargent - Coxsaba amiriNo ratings yet
- Aging and Women's Sexuality Research PAPERDocument9 pagesAging and Women's Sexuality Research PAPERCristina ObregonNo ratings yet
- Sneed2005 PDFDocument14 pagesSneed2005 PDFAulya OctaviaNo ratings yet
- Chaffin COGNITIVE LEARNING APPLIED TO OLDER ADULTDocument30 pagesChaffin COGNITIVE LEARNING APPLIED TO OLDER ADULTPierre UlysseNo ratings yet
- Age (Chapter 12)Document63 pagesAge (Chapter 12)Audra GreenNo ratings yet
- Ageism The Myth of Growing OldDocument10 pagesAgeism The Myth of Growing OldSherrie D. LarchNo ratings yet
- Artikel LGBT 2020Document18 pagesArtikel LGBT 20200120 Annafia HanifNo ratings yet
- Fighting AgeismDocument8 pagesFighting AgeismApple Esteban CalmaNo ratings yet
- A Sharp Drop or A Gentle Slope? Aging, The Elderly, and Mass Media ConsumptionDocument24 pagesA Sharp Drop or A Gentle Slope? Aging, The Elderly, and Mass Media ConsumptionRendorn GuerrinNo ratings yet
- How Do Stereotypes Appear in SocietyDocument4 pagesHow Do Stereotypes Appear in SocietyGabriel DelfinNo ratings yet
- Socioemotional Development in Late AdulthoodDocument15 pagesSocioemotional Development in Late Adulthoodsonali mishraNo ratings yet
- A - Week 5 - Ageism (2016 - 09 - 25 18 - 04 - 03 Utc)Document12 pagesA - Week 5 - Ageism (2016 - 09 - 25 18 - 04 - 03 Utc)KalaNo ratings yet
- Research Paper AgeismDocument8 pagesResearch Paper Ageismapeuyqznd100% (1)
- Old Age Consists of Ages Nearing or Surpassing The Average Life Span of HumanDocument13 pagesOld Age Consists of Ages Nearing or Surpassing The Average Life Span of HumanVarun JainNo ratings yet
- Allen & Roberto 2009-2 PDFDocument12 pagesAllen & Roberto 2009-2 PDFAnonymous ucxe58O4No ratings yet
- E BP Older AdultsDocument13 pagesE BP Older AdultsMihaelaSiVictoriaNo ratings yet
- Disabled EducationDocument8 pagesDisabled EducationfazahiNo ratings yet
- Aging in The MediaDocument6 pagesAging in The MediaGeoffrey MuendoNo ratings yet
- Kaplan - Senior Moment - A Typical Example of How Older People Are OtheredDocument7 pagesKaplan - Senior Moment - A Typical Example of How Older People Are OtheredcorreoaquiNo ratings yet
- Psychological Practice Girls Women PDFDocument38 pagesPsychological Practice Girls Women PDFBhargav100% (1)
- Watter, Sexuality and AgingDocument14 pagesWatter, Sexuality and AgingjajajaNo ratings yet
- In Aging Today July/August 2011Document1 pageIn Aging Today July/August 2011UGADAYouthMovementNo ratings yet
- Trajectories of Depressive Symptomatology and Loneliness in Older Adult Sexual Minorities and Heterosexual GroupsDocument14 pagesTrajectories of Depressive Symptomatology and Loneliness in Older Adult Sexual Minorities and Heterosexual GroupsalinemariarizzonNo ratings yet
- Elderly Baby BoomersDocument2 pagesElderly Baby BoomerscesararroyoNo ratings yet
- Mercado - Social PsychologyDocument26 pagesMercado - Social PsychologynessaNo ratings yet
- How Discrimination and Stress Affects Self-Esteem Among Dominican Immigrant Women: An Exploratory StudyDocument20 pagesHow Discrimination and Stress Affects Self-Esteem Among Dominican Immigrant Women: An Exploratory StudyYong YangNo ratings yet
- Sexuality Among Older Adults-Holmes sp20Document11 pagesSexuality Among Older Adults-Holmes sp20api-437977619No ratings yet
- Attitude Towards The Elderly in The Modern WorldDocument2 pagesAttitude Towards The Elderly in The Modern Worldrnld0% (1)
- Ageism in The United StatesDocument8 pagesAgeism in The United StatesMia MyoNo ratings yet
- Longevity Increased by Positive Self-Perceptions of Aging: Attitudes and Social CognitionDocument10 pagesLongevity Increased by Positive Self-Perceptions of Aging: Attitudes and Social CognitionMaximiliano xDNo ratings yet
- Age Disparity Between GendersDocument22 pagesAge Disparity Between Gendersapi-659623153No ratings yet
- Aging Deviation - EditedDocument7 pagesAging Deviation - EditedmoureenNo ratings yet
- AGEISMDocument12 pagesAGEISMKalaNo ratings yet
- Gender and DisabilityDocument14 pagesGender and DisabilityefunctionNo ratings yet
- Background Scope of The Problem Risk Factors Case Studies of Youth Suicide Conclusions and Recommendations ReferencesDocument13 pagesBackground Scope of The Problem Risk Factors Case Studies of Youth Suicide Conclusions and Recommendations ReferencesbntmaniNo ratings yet
- BSN3B Zerrudo Introduction To Geriatric NursingDocument3 pagesBSN3B Zerrudo Introduction To Geriatric NursingGlen DaleNo ratings yet
- Effects of Gender Roles On Men and WomenDocument9 pagesEffects of Gender Roles On Men and WomenGabz GabbyNo ratings yet
- Ringkasan End of Life IssuesDocument7 pagesRingkasan End of Life IssuesKevin Satya GanandaNo ratings yet
- Old Age 2Document2 pagesOld Age 2Sumit NegiNo ratings yet
- χριστακηςDocument15 pagesχριστακηςElizabeth HensleyNo ratings yet
- How Travel Can Counteract Social IsolationDocument31 pagesHow Travel Can Counteract Social IsolationAnne MacIverNo ratings yet
- Issues by KryzelleDocument4 pagesIssues by KryzellekiezerNo ratings yet
- Gender Differences in Psychosocial Determinants of Self Perceived Health Among Portuguese Older Adults in Nursing HomesDocument9 pagesGender Differences in Psychosocial Determinants of Self Perceived Health Among Portuguese Older Adults in Nursing HomesAnaNo ratings yet
- Atypical Gender DevelopmentDocument20 pagesAtypical Gender Developmenth_drummerNo ratings yet
- Ageing Myth RealityDocument44 pagesAgeing Myth RealityVijaya RaniNo ratings yet
- 21 Hypersexual in Dementia PDFDocument6 pages21 Hypersexual in Dementia PDFSusi RutmalemNo ratings yet
- Assignment GerontologyDocument18 pagesAssignment GerontologySawera KasiNo ratings yet
- Lived Experiences of Elder Individuals in "Balay Taripato"Document6 pagesLived Experiences of Elder Individuals in "Balay Taripato"rnrmmanphdNo ratings yet
- Vanderminden Esala 2018 Beyond Symptoms Race and Gender Predict Anxiety Disorder DiagnosisDocument15 pagesVanderminden Esala 2018 Beyond Symptoms Race and Gender Predict Anxiety Disorder DiagnosisAulia rahmaNo ratings yet
- Ageism and Mistreatment of Older Workers: Current Reality, Future SolutionsFrom EverandAgeism and Mistreatment of Older Workers: Current Reality, Future SolutionsNo ratings yet
- 10.1007@s12094 019 02107 WDocument6 pages10.1007@s12094 019 02107 WUzi SuruziNo ratings yet
- Cinamon 2016Document12 pagesCinamon 2016Uzi SuruziNo ratings yet
- (Career Skills Library) Infobase Publishing - Leadership Skills-Ferguson (2009)Document169 pages(Career Skills Library) Infobase Publishing - Leadership Skills-Ferguson (2009)Uzi SuruziNo ratings yet
- Moocs As A Means To Provide Education Equity in Indonesia: An Empirical Study at A Private University of YogyakartaDocument7 pagesMoocs As A Means To Provide Education Equity in Indonesia: An Empirical Study at A Private University of YogyakartaUzi SuruziNo ratings yet
- Kamus Ilmiah Populer: Rating: (40 Votes) ID Number: KA-1F7426AEECFFB85 - Format: EnglishDocument2 pagesKamus Ilmiah Populer: Rating: (40 Votes) ID Number: KA-1F7426AEECFFB85 - Format: EnglishUzi SuruziNo ratings yet
- Continuous Quality Improvement in Implementation of Equity-Based EducationDocument4 pagesContinuous Quality Improvement in Implementation of Equity-Based EducationUzi SuruziNo ratings yet
- Oer and Oep For Access Equity Equality Quality Inclusiveness and Empowering Lifelong LearningDocument24 pagesOer and Oep For Access Equity Equality Quality Inclusiveness and Empowering Lifelong LearningUzi SuruziNo ratings yet
- The Multicultural Organizations: Perceptions of Diversity Challenges and InitiativesDocument13 pagesThe Multicultural Organizations: Perceptions of Diversity Challenges and InitiativesUzi SuruziNo ratings yet
- Your Abstract Title Should Use This Font Type and SizeDocument1 pageYour Abstract Title Should Use This Font Type and SizeUzi SuruziNo ratings yet
- Usantara: A Comparative Study On The Oral ProficiencyDocument4 pagesUsantara: A Comparative Study On The Oral ProficiencyUzi SuruziNo ratings yet
- 8c99f2 PDFDocument52 pages8c99f2 PDFKrisParadajsNo ratings yet
- Spiritual Chi PDFDocument4 pagesSpiritual Chi PDFPedro MoralesNo ratings yet
- NCP For ChildrenDocument17 pagesNCP For ChildrenRachel Niu IINo ratings yet
- Problem 1 Emergency Medicine Block: Agustina Cynthia Cesari S 405140066 Group 1Document90 pagesProblem 1 Emergency Medicine Block: Agustina Cynthia Cesari S 405140066 Group 1Astri GunardiNo ratings yet
- 150 Practice EcgsDocument151 pages150 Practice EcgsTimothy ChungNo ratings yet
- Advanced Paediatric Life Support - A0 PDFDocument1 pageAdvanced Paediatric Life Support - A0 PDFiulia-uroNo ratings yet
- Narrative ReportDocument1 pageNarrative ReportMichaelNo ratings yet
- Wearable Bio Sensors Og Report AneesDocument22 pagesWearable Bio Sensors Og Report AneesSufail ANo ratings yet
- Heart SoundsDocument23 pagesHeart SoundsK.R.RaguramNo ratings yet
- Basic Coronary Angiography All SlidesDocument55 pagesBasic Coronary Angiography All SlidesSaud ShirwanNo ratings yet
- Lecture 21 ReptileDocument5 pagesLecture 21 ReptileLol MdrNo ratings yet
- Anatomical EponymsDocument14 pagesAnatomical EponymsscribdarnabNo ratings yet
- Lecture and Q and A Series in Medico Legal PDFDocument942 pagesLecture and Q and A Series in Medico Legal PDFArjhade Sarita100% (2)
- Cardiac Cycle: Presenter: DR Hairul Anuar Bin MahatDocument23 pagesCardiac Cycle: Presenter: DR Hairul Anuar Bin MahatHairul AnuarNo ratings yet
- Cambridge International AS & A Level: Biology 9700/12Document20 pagesCambridge International AS & A Level: Biology 9700/12Pranav Ramesh BadrinathNo ratings yet
- Betnesol InformationDocument6 pagesBetnesol InformationsmazNo ratings yet
- Easi MonitorDocument14 pagesEasi MonitorRaisya AfiaNo ratings yet
- CSEC Human & Social Biology - January 2015 Paper 1Document11 pagesCSEC Human & Social Biology - January 2015 Paper 1Kimari Blackwood100% (1)
- SDI Forms 16 Medical QuestionnaireDocument15 pagesSDI Forms 16 Medical Questionnaireadityajain93No ratings yet
- PHD Thesis Topics Public HealthDocument6 pagesPHD Thesis Topics Public Healthbsgnqj4n100% (2)
- Especificaciones S5 V1.4Document6 pagesEspecificaciones S5 V1.4Soporte BiosummaNo ratings yet
- Practical Workbook Answers: Exam-Style Questions Practical Investigation 1.1Document27 pagesPractical Workbook Answers: Exam-Style Questions Practical Investigation 1.1Adah Joshi100% (1)
- Cambridge Primary Checkpoint - Science (0846) October 2021 Paper 1 MSDocument20 pagesCambridge Primary Checkpoint - Science (0846) October 2021 Paper 1 MSflameriderbby100% (3)
- Daftar PustakaDocument4 pagesDaftar PustakaDesi MardianiNo ratings yet
- Revista Colombiana de Anestesiología: Evidence-Based Clinical Practice Manual: Cardiopulmonary-Cerebral ResuscitationDocument11 pagesRevista Colombiana de Anestesiología: Evidence-Based Clinical Practice Manual: Cardiopulmonary-Cerebral Resuscitationkuriakosejane6No ratings yet
- Music Has The Power To HealDocument16 pagesMusic Has The Power To HealBalajiNo ratings yet
- Minimal Invasive Extra-Corporeal Circulation (MiECC) - A RevolutionaryDocument3 pagesMinimal Invasive Extra-Corporeal Circulation (MiECC) - A RevolutionaryAhmadNo ratings yet