Download as pdf or txt
You might also like
- Endocrine Board Review 2020 PDFDocument256 pagesEndocrine Board Review 2020 PDFVikrant67% (6)
- Ra Uru Hu - PHS I. Semester 1. The Mechanics of The Vehicle PDFDocument252 pagesRa Uru Hu - PHS I. Semester 1. The Mechanics of The Vehicle PDFИрина Терещенко93% (30)
- Project Proposal On Iodized Salt Production Factory: Promoted By: Mr. Abdulsemed NegashDocument54 pagesProject Proposal On Iodized Salt Production Factory: Promoted By: Mr. Abdulsemed NegashTegegne Aklilu95% (21)
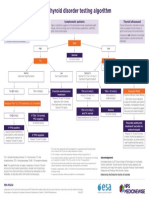
- NPS MedicineWise Thyroid Testing Algorithm v3Document1 pageNPS MedicineWise Thyroid Testing Algorithm v3Mikhael JHNo ratings yet
- Case 1 EndocrineDocument5 pagesCase 1 EndocrineRegine Mae EncinadaNo ratings yet
- 0a27thyroid Function TestDocument35 pages0a27thyroid Function TestAshokvardhan Chowdary Nandigam67% (3)
- MCQs of Digestive SystemDocument4 pagesMCQs of Digestive Systemالموعظة الحسنه chanel100% (15)
- Approach To A Low TSH Level - Patience Is A Virtue PDFDocument10 pagesApproach To A Low TSH Level - Patience Is A Virtue PDFDonovan KyleNo ratings yet
- 10 16 Thyroid Function NitinDocument7 pages10 16 Thyroid Function NitinStrawberry ShortcakeNo ratings yet
- B Rajkovich 1983Document3 pagesB Rajkovich 1983ktyhekNo ratings yet
- Clinical Practice Guidelines For Hypothyroidism in Adults: AACE and ATA 2012Document63 pagesClinical Practice Guidelines For Hypothyroidism in Adults: AACE and ATA 2012Nur Rakhma AkmaliaNo ratings yet
- Thyroid Tests and ResultsDocument9 pagesThyroid Tests and ResultsKristel BelgicaNo ratings yet
- TFT Interpretation of Difficult CasesDocument51 pagesTFT Interpretation of Difficult CasesAditya GautamNo ratings yet
- Circadian Rhythm: I. Basic of The Thyroid Function: Fundamentals in Laboratory MedicineDocument6 pagesCircadian Rhythm: I. Basic of The Thyroid Function: Fundamentals in Laboratory MedicineNIGHT tubeNo ratings yet
- Thyroid Function Tests (TFT'S) : Roll No 04Document22 pagesThyroid Function Tests (TFT'S) : Roll No 04Ajay YANo ratings yet
- Thyroid Function TestsDocument15 pagesThyroid Function TestsJoseline AliceNo ratings yet
- Thyroid Function TestDocument28 pagesThyroid Function TestDhinesh Muthusamy100% (1)
- Ok Bab 20 Reproduction and Thyroid (Ky)Document22 pagesOk Bab 20 Reproduction and Thyroid (Ky)rista silvanaNo ratings yet
- Thyroid Functions TestDocument11 pagesThyroid Functions TestFatima AsgharNo ratings yet
- Thyroid Function Test 12-2-09Document69 pagesThyroid Function Test 12-2-09Romaysaamohamed AlyNo ratings yet
- Biol 460 Case StudyDocument11 pagesBiol 460 Case Studyapi-353888678No ratings yet
- Managing Thyroid Disease in General PracticeDocument6 pagesManaging Thyroid Disease in General PracticeEmir SaricNo ratings yet
- Chapter 47Document19 pagesChapter 47Javier Burgos CárdenasNo ratings yet
- (Health) Thyroid Functions TestsDocument4 pages(Health) Thyroid Functions Testsmahendra3107No ratings yet
- Thyroid Tests: What Is The Thyroid?Document8 pagesThyroid Tests: What Is The Thyroid?JyotiNo ratings yet
- FunctionTests BrochureDocument2 pagesFunctionTests Brochurejonalyntonato09No ratings yet
- Investigating Low TSH (BMJ 2013) Endocrine DisordersDocument4 pagesInvestigating Low TSH (BMJ 2013) Endocrine DisordersLouiseNo ratings yet
- Hypothyroidism Diagnosis FlowchartDocument1 pageHypothyroidism Diagnosis FlowchartKim Yang ChongNo ratings yet
- Thyroid Function Test and Adrenal Function TestsDocument64 pagesThyroid Function Test and Adrenal Function TestsDr Abhinav Manish MDNo ratings yet
- Interpretation of Thyroid Function TestsDocument6 pagesInterpretation of Thyroid Function TestsJuan CanoNo ratings yet
- Zak Notes Hypothyroidism (Juma)Document34 pagesZak Notes Hypothyroidism (Juma)82cxp4n46wNo ratings yet
- Biochemical Testing of The Thyroid: TSH Is The Best And, Oftentimes, Only Test Needed - A Review For Primary CareDocument10 pagesBiochemical Testing of The Thyroid: TSH Is The Best And, Oftentimes, Only Test Needed - A Review For Primary CareElsaBorrellGarcíaNo ratings yet
- Thyroid DisordersDocument22 pagesThyroid DisordersNimer Abdelhadi AliNo ratings yet
- Kirkegaard 1998Document9 pagesKirkegaard 1998coolgirl4realzNo ratings yet
- Thyroid Function Test PDFDocument2 pagesThyroid Function Test PDFAlizaPinkyNo ratings yet
- Laboratory Diagnostics of (Selected) Endocrine DisordersDocument48 pagesLaboratory Diagnostics of (Selected) Endocrine DisordersPaulina PaskeviciuteNo ratings yet
- ReportDocument1 pageReportanshumanshinde12040No ratings yet
- Thyroid Function Tests and Goitre SV 24-4-21Document51 pagesThyroid Function Tests and Goitre SV 24-4-21Lal KhanNo ratings yet
- FunctionTests Brochure PDFDocument2 pagesFunctionTests Brochure PDFArslan SaleemNo ratings yet
- Management of Subclinical Hyperthyroidism PDFDocument1 pageManagement of Subclinical Hyperthyroidism PDFRovelyn CalinawaganNo ratings yet
- Assessment of Thyroid FunctionDocument7 pagesAssessment of Thyroid FunctionDewi Paramita YuniarahmiNo ratings yet
- Thyroid Function TestDocument11 pagesThyroid Function TestBookmyscansNo ratings yet
- How To Interpret Thyroid Function TestsDocument5 pagesHow To Interpret Thyroid Function TestsnonieshzNo ratings yet
- Thyroid Function Test: The "Hidden" Health ProblemDocument34 pagesThyroid Function Test: The "Hidden" Health Problemvjanand07100% (1)
- Endocrinology Part 2Document4 pagesEndocrinology Part 2Alondra SagarioNo ratings yet
- Thyroid Function Test (TFT)Document16 pagesThyroid Function Test (TFT)PAPUN KUMAR ROUT100% (1)
- Thyroid Function TestDocument2 pagesThyroid Function Testhannah lanasaNo ratings yet
- Interpretasi TiroidDocument6 pagesInterpretasi TiroidSagita MuliaNo ratings yet
- Hypothalamic Pitutary Axis and Thyroid Hormone SynthesisDocument5 pagesHypothalamic Pitutary Axis and Thyroid Hormone Synthesis78 shivangi mauryaNo ratings yet
- Thyroid GlandDocument49 pagesThyroid Glandjuliefe pinionNo ratings yet
- Thyroid Talk-FMD RdsDocument58 pagesThyroid Talk-FMD RdsSriman YarrarapuNo ratings yet
- Thyroid Storm SeminarDocument33 pagesThyroid Storm SeminarDishani DeyNo ratings yet
- Kate PlanchetDocument29 pagesKate Planchetsundance127No ratings yet
- Diagnosis of HypothyroidismDocument10 pagesDiagnosis of HypothyroidismHanzla IrfanNo ratings yet
- Diagnosis of and Screening For Hypothyroidism in Nonpregnant AdultsDocument22 pagesDiagnosis of and Screening For Hypothyroidism in Nonpregnant AdultsJoseline Stephanie Pérez ChacónNo ratings yet
- Subclinical Hyperthyroidism: To Treat or Not To Treat?: Best PracticeDocument5 pagesSubclinical Hyperthyroidism: To Treat or Not To Treat?: Best PracticeRaka MahasaduNo ratings yet
- TRH Stimulation TestDocument3 pagesTRH Stimulation TestsakuraleeshaoranNo ratings yet
- Stop The Thyroid Madness Sanjay Dixit MDDocument68 pagesStop The Thyroid Madness Sanjay Dixit MDdb50% (2)
- Thyroid FunctionDocument12 pagesThyroid Functionسلطان القلحNo ratings yet
- Thyroid Function Tests: What Is The Thyroid Gland?Document8 pagesThyroid Function Tests: What Is The Thyroid Gland?Rahadiyan HadinataNo ratings yet
- T4 Reactiv ChemiluminiscentaDocument5 pagesT4 Reactiv ChemiluminiscentaLidia NarbNo ratings yet
- Diagnosis of and Screening For Hypothyroidism in Nonpregnant Adults - UpToDateDocument15 pagesDiagnosis of and Screening For Hypothyroidism in Nonpregnant Adults - UpToDateDiego NamucheNo ratings yet
- 121-2023 16.06.2023Document2 pages121-2023 16.06.2023SuvNo ratings yet
- 8 Cardiorespiratory FitnessDocument10 pages8 Cardiorespiratory FitnessSuvNo ratings yet
- How To Give A Scientific Presentation - 0Document20 pagesHow To Give A Scientific Presentation - 0SuvNo ratings yet
- Scope, Coverage and Methodology Used For Preparing The UGC-approved List of JournalsDocument1 pageScope, Coverage and Methodology Used For Preparing The UGC-approved List of JournalsSuvNo ratings yet
- "Sandhya" Realizing Conjunctions of Life: Sayan Sandhya. All These Are Sandhyas, and A Dwija Does Gayatri atDocument5 pages"Sandhya" Realizing Conjunctions of Life: Sayan Sandhya. All These Are Sandhyas, and A Dwija Does Gayatri atSuvNo ratings yet
- Animal EthicsDocument57 pagesAnimal EthicsSuvNo ratings yet
- Animal EthicsDocument57 pagesAnimal EthicsSuvNo ratings yet
- Thyroid and Antithyroid Agent-VDocument60 pagesThyroid and Antithyroid Agent-VVine100% (1)
- Trouble Shooting Elecsys2 010v53Document142 pagesTrouble Shooting Elecsys2 010v53Hồ Thế NguyênNo ratings yet
- Ujjayi PranayamaDocument2 pagesUjjayi PranayamaArun C. RaoNo ratings yet
- Thyroid Function and Obesity: Translational Thyroidology / ReviewDocument9 pagesThyroid Function and Obesity: Translational Thyroidology / ReviewXochitemiqui YoacihualtNo ratings yet
- Endocrine Lab ManualDocument9 pagesEndocrine Lab ManualApril Joy de LimaNo ratings yet
- S60 - LPL - Noida 3 N-27, Sec-18, Commercial Complex, Near. Atta Market, Noida.120-3029866/3142530 NoidaDocument2 pagesS60 - LPL - Noida 3 N-27, Sec-18, Commercial Complex, Near. Atta Market, Noida.120-3029866/3142530 Noidavimal kumar dwivediNo ratings yet
- FRM Patient View All ReportDocument3 pagesFRM Patient View All ReportRajeev KumarNo ratings yet
- Congenital Hypothyroidism: Screening, Diagnosis, Management, and OutcomeDocument7 pagesCongenital Hypothyroidism: Screening, Diagnosis, Management, and OutcomeIbrahim Abdul KareemNo ratings yet
- 2 - Thyroxine and Treatment of Hypothyroidism - 2019Document8 pages2 - Thyroxine and Treatment of Hypothyroidism - 2019Johanna Bustos NutricionistaNo ratings yet
- Thyroid DisorersDocument23 pagesThyroid DisorersBryan Lloyd RayatNo ratings yet
- Thyroid DissertationDocument7 pagesThyroid DissertationCustomPaperWritingServiceNorthLasVegas100% (1)
- MASSAGE YOUR NECK WITH RED ONION AND SEE WHAT HAPPENS, INCREDIBLE! - FAHACKS - Fashion, DIY, Hacks and More PDFDocument5 pagesMASSAGE YOUR NECK WITH RED ONION AND SEE WHAT HAPPENS, INCREDIBLE! - FAHACKS - Fashion, DIY, Hacks and More PDFNikola DukuzovskiNo ratings yet
- Key Points - RevisionDocument58 pagesKey Points - RevisionsophieNo ratings yet
- Endocrine System: MSN 4006 Advanced PsychopathophysiologyDocument15 pagesEndocrine System: MSN 4006 Advanced Psychopathophysiologybane1925No ratings yet
- Deepika.R:::: Patient Age / Sex 26 Y / Female BranchDocument2 pagesDeepika.R:::: Patient Age / Sex 26 Y / Female BranchkannanNo ratings yet
- What Is The Endocrine System?Document4 pagesWhat Is The Endocrine System?ROXANNE V. LOPEZNo ratings yet
- Journal AnalysisDocument2 pagesJournal AnalysisJust yor Regular CavegirlNo ratings yet
- The Endocrine SystemDocument2 pagesThe Endocrine SystempengxnNo ratings yet
- Ultrasound Imaging of The NeckDocument25 pagesUltrasound Imaging of The Neckmark jacob dela rosaNo ratings yet
- Chakra Balancing Meditation Program by Ascension BeatsDocument2 pagesChakra Balancing Meditation Program by Ascension BeatsDeepak Satsangi100% (1)
- J Ejrad 2015 02 009Document5 pagesJ Ejrad 2015 02 009sujit naikNo ratings yet
- ChandanKumar 632972Document11 pagesChandanKumar 632972Chandan JhaNo ratings yet
- Factors Influencing Human DevelopmentDocument4 pagesFactors Influencing Human Developmentcarina30_rcgNo ratings yet
- Bone Remodeling: Vitamin A Vitamin C Vitamin D Vitamins K and B The Insulin-Like Growth Factors (Igfs)Document2 pagesBone Remodeling: Vitamin A Vitamin C Vitamin D Vitamins K and B The Insulin-Like Growth Factors (Igfs)Lainie ZefiahNo ratings yet
- Subclinical Hyperthyroidism: When To Consider TreatmentDocument7 pagesSubclinical Hyperthyroidism: When To Consider TreatmentAnisa Iswari Pombaile-NgurawanNo ratings yet
- My Mudole ScienceDocument4 pagesMy Mudole ScienceNasrimah IbrahimNo ratings yet