Download as pdf or txt
You might also like
- Endodontic MCQ PDFDocument17 pagesEndodontic MCQ PDFYousef Hussain Ghannam89% (66)
- Case Study Addison's Disease Part 1Document27 pagesCase Study Addison's Disease Part 1Whitney PierreNo ratings yet
- Behavioral Psychosis in DementiaDocument62 pagesBehavioral Psychosis in DementiaAlexander NavarraNo ratings yet
- Pharm PPT SubmitDocument29 pagesPharm PPT SubmitCarla Ward TiptonNo ratings yet
- Eating Disorders 1Document17 pagesEating Disorders 1Heba_Al_Khozae100% (1)
- Anti-Aging Therapeutics Volume XIIIFrom EverandAnti-Aging Therapeutics Volume XIIINo ratings yet
- End of Life Care: Presented by Pankaj Nurse Practitioner 2 Yr Moderator Dr. Sushant Khanduri Associate ProfessorDocument43 pagesEnd of Life Care: Presented by Pankaj Nurse Practitioner 2 Yr Moderator Dr. Sushant Khanduri Associate ProfessorQudrat Un NissaNo ratings yet
- Alzheimers DiseaseDocument85 pagesAlzheimers DiseaseThe ChannelNo ratings yet
- DeprDocument26 pagesDeprmalika hmisNo ratings yet
- MCInfoSheet FatigueDocument3 pagesMCInfoSheet Fatigueazeezsharique4No ratings yet
- Palliative Care Lecture 2022Document20 pagesPalliative Care Lecture 2022Shreyas WalvekarNo ratings yet
- Multiple SclerosisDocument44 pagesMultiple SclerosisVijaya LakshmiNo ratings yet
- Depressive DisordersDocument7 pagesDepressive DisordersEllen JulianNo ratings yet
- GG Menstruasi - Dysmenorea DLLDocument35 pagesGG Menstruasi - Dysmenorea DLLPSC 119 Kota TegalNo ratings yet
- Depression at Family PracticeDocument38 pagesDepression at Family PracticehananNo ratings yet
- Epec-O m03c Anxiety PHDocument10 pagesEpec-O m03c Anxiety PHsanalcrazyNo ratings yet
- Cu7 - Pain 1Document18 pagesCu7 - Pain 1FERMIL PASGALANo ratings yet
- Symptom Management in Palliative CareDocument56 pagesSymptom Management in Palliative CareDisala RanaweeraNo ratings yet
- Approach To FatigueDocument27 pagesApproach To FatigueBasil Hussam100% (1)
- DepressionDocument29 pagesDepressionBushra EjazNo ratings yet
- Eating Disorder 1Document20 pagesEating Disorder 1BEA RADANo ratings yet
- Management of Anxiety and Breathlessness in A PalliativeDocument46 pagesManagement of Anxiety and Breathlessness in A PalliativeSayan DasNo ratings yet
- Lesson 4 - EatingdisorderDocument41 pagesLesson 4 - EatingdisorderAna CauinianNo ratings yet
- Mood DisordersDocument14 pagesMood DisordersHayat AL AKOUMNo ratings yet
- Pat 11052014Document18 pagesPat 11052014api-300362983No ratings yet
- Headache 2Document21 pagesHeadache 2geeeelzy07No ratings yet
- Pat 1 Medsurg 2Document18 pagesPat 1 Medsurg 2api-294300618No ratings yet
- Bezuidenhout 2018 DysmenorrhoeaanoverviewDocument6 pagesBezuidenhout 2018 Dysmenorrhoeaanoverviewcarladabboura79No ratings yet
- The Disease of AddictionDocument60 pagesThe Disease of AddictionBodj OdejarNo ratings yet
- Eating Disorders and Its Dental ImpactDocument4 pagesEating Disorders and Its Dental ImpactInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- PREMENSTRUAL SYNDROME (PMS) - Rafael Costa Gouveia Mariz Group 01Document15 pagesPREMENSTRUAL SYNDROME (PMS) - Rafael Costa Gouveia Mariz Group 01Rafael100% (1)
- Anxiety NeurosisDocument6 pagesAnxiety NeurosisSuyash TambeNo ratings yet
- Pain Management in Elderly Persons: UCLA Multicampus Program of Geriatrics and GerontologyDocument20 pagesPain Management in Elderly Persons: UCLA Multicampus Program of Geriatrics and GerontologyTommy_charwinNo ratings yet
- Psychopharmacology NotesDocument33 pagesPsychopharmacology NotesIshita VermaNo ratings yet
- Case Study Number FourDocument5 pagesCase Study Number FourYessamin Paith RoderosNo ratings yet
- Preassignment Work-Careplan #2Document30 pagesPreassignment Work-Careplan #2djbhetaNo ratings yet
- Pat Revised 2013 1Document19 pagesPat Revised 2013 1api-300362033No ratings yet
- HES-005-Session-10-SASDocument10 pagesHES-005-Session-10-SASDave Ortiz Robert MaglasangNo ratings yet
- 07 Presentation Ferris Common SymptomsDocument55 pages07 Presentation Ferris Common SymptomsLakshmi PrathyushaNo ratings yet
- Polypharmacy in The: The Bagful of Pills: ElderlyDocument34 pagesPolypharmacy in The: The Bagful of Pills: ElderlyrandatagNo ratings yet
- Palliative Care in Multiple MyelomaDocument45 pagesPalliative Care in Multiple MyelomamadvincyNo ratings yet
- DepressionDocument47 pagesDepressionJean Pierre FakhouryNo ratings yet
- Marchesi 2008Document14 pagesMarchesi 2008Mauro JacobsNo ratings yet
- AnorexiaDocument11 pagesAnorexiaRAHMANI NOURELHOUDANo ratings yet
- Anxiety Disorders: Samantha Meltzer-Brody, M.D., M.P.H. Assistant Professor UNC Department of PsychiatryDocument62 pagesAnxiety Disorders: Samantha Meltzer-Brody, M.D., M.P.H. Assistant Professor UNC Department of PsychiatryPRHSTNo ratings yet
- Spring Pat 2Document22 pagesSpring Pat 2api-241359111No ratings yet
- Substance AbuseDocument55 pagesSubstance Abusenikolamatejic100% (1)
- Pat Semester 1Document17 pagesPat Semester 1api-300946501No ratings yet
- Pathophysiology: Depressed Mood Loss of Interest and Pleasure in ActivitiesDocument4 pagesPathophysiology: Depressed Mood Loss of Interest and Pleasure in ActivitiesBrittany VandermeulenNo ratings yet
- Depression and Anxiety in Palliative Care - DR Richard LimDocument39 pagesDepression and Anxiety in Palliative Care - DR Richard Limmalaysianhospicecouncil6240No ratings yet
- Pat1 Med Surg 1Document19 pagesPat1 Med Surg 1api-339132978No ratings yet
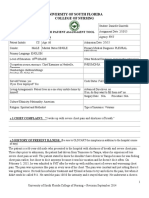
- Patient Assessment Tool ms2Document27 pagesPatient Assessment Tool ms2api-280998981No ratings yet
- Group 4 Substance Abuse and DepressionDocument22 pagesGroup 4 Substance Abuse and DepressionALIZA BAKILNo ratings yet
- Old Age Booklet RechcedDocument26 pagesOld Age Booklet Rechcedsandeep singh cheemaNo ratings yet
- Eating Disorders and Their Implications On Oral Health - Role of DentistsDocument6 pagesEating Disorders and Their Implications On Oral Health - Role of DentistsThaily MoralesNo ratings yet
- Depression: Psychiatric DisordersDocument21 pagesDepression: Psychiatric DisordersNdoo NdooNo ratings yet
- Migraine and Its Relation With LifestyleDocument7 pagesMigraine and Its Relation With LifestyleMehram JuttNo ratings yet
- Psycho Therapy On EduDocument6 pagesPsycho Therapy On EduLone MusaibNo ratings yet
- Premenstrual Syndrome: DR Abdul MoizDocument21 pagesPremenstrual Syndrome: DR Abdul MoizAbdul MoizNo ratings yet
- Chronic Fatigue Syndrome Cure: Powerful Techniques to Stimulate Your Hormones, Improve Metabolism, And Boost Your Energy LevelsFrom EverandChronic Fatigue Syndrome Cure: Powerful Techniques to Stimulate Your Hormones, Improve Metabolism, And Boost Your Energy LevelsNo ratings yet
- The Vitamin Cure for Chronic Fatigue Syndrome: How to Prevent and Treat Chronic Fatigue Syndrome Using Safe and Effective Natural TherapiesFrom EverandThe Vitamin Cure for Chronic Fatigue Syndrome: How to Prevent and Treat Chronic Fatigue Syndrome Using Safe and Effective Natural TherapiesNo ratings yet
- Preservatives Used in Eye Drops: Paytaxt Private Institute Pharmacy Department 1 StageDocument7 pagesPreservatives Used in Eye Drops: Paytaxt Private Institute Pharmacy Department 1 StageShakar Ezaddin AbdullahNo ratings yet
- Antibiotic Resistance: Key PointsDocument7 pagesAntibiotic Resistance: Key Pointsgeorgi.annaNo ratings yet
- Khodayari, 2011Document5 pagesKhodayari, 2011KharismaNisaNo ratings yet
- Lilyasari2019 Article EconomicEvaluationOfSildenafilDocument9 pagesLilyasari2019 Article EconomicEvaluationOfSildenafilNajib Al FatinNo ratings yet
- Republic of Iraq: Medical DevicesDocument5 pagesRepublic of Iraq: Medical Devicesالحارث فخري فياض احمدNo ratings yet
- Descripción PVF Xistencias: Desc%Document18 pagesDescripción PVF Xistencias: Desc%Nelly NoemiNo ratings yet
- Product Datasheet: MCM7 Antibody NBP1-85721Document5 pagesProduct Datasheet: MCM7 Antibody NBP1-85721JoaoNo ratings yet
- Kidney Specialist in Pune - Kidney Doctor in PuneDocument4 pagesKidney Specialist in Pune - Kidney Doctor in PunePriime NephrocareNo ratings yet
- MCQ THDocument200 pagesMCQ THarushrushNo ratings yet
- Fajo 990Document238 pagesFajo 990Mohamed A SalehNo ratings yet
- Physiotherapy Scoliosis-Specific Exercises - A Comprehensive Review of Seven Major SchoolsDocument76 pagesPhysiotherapy Scoliosis-Specific Exercises - A Comprehensive Review of Seven Major SchoolskoriatsuNo ratings yet
- Don'T Exercise Cellercise!: by Rica E. VillalonDocument21 pagesDon'T Exercise Cellercise!: by Rica E. VillalonMónica SastoqueNo ratings yet
- Management of Preoperative Anemia: Laura Mendez-Pino,, Andrés Zorrilla-Vaca,, David L. HepnerDocument9 pagesManagement of Preoperative Anemia: Laura Mendez-Pino,, Andrés Zorrilla-Vaca,, David L. HepneryenuginNo ratings yet
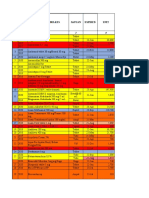
- No Tahun Nama Obat / Perbelkes Satuan Expired UnitDocument5 pagesNo Tahun Nama Obat / Perbelkes Satuan Expired UnitBayu Firmansyah AlitNo ratings yet
- Otology Fellowships 2019Document5 pagesOtology Fellowships 2019Sandra SandrinaNo ratings yet
- Practical Guide and Atlas For The Diagnosis of Fungal InfectionsDocument68 pagesPractical Guide and Atlas For The Diagnosis of Fungal Infectionsasfwegere100% (1)
- Daftar PustakaDocument3 pagesDaftar PustakarestyNZNo ratings yet
- Audiological Evaluation: Dr. Shakuntala Misra National Rehabilitation University, LucknowDocument3 pagesAudiological Evaluation: Dr. Shakuntala Misra National Rehabilitation University, LucknowHarshit AmbeshNo ratings yet
- Post Abortion CareDocument35 pagesPost Abortion CareNatukunda DianahNo ratings yet
- Trauma Thoraks PDFDocument86 pagesTrauma Thoraks PDFMiftahurrahmiNo ratings yet
- Siberia Medical TrainDocument1 pageSiberia Medical TrainSantiago CarreñoNo ratings yet
- Alzheimer WorksheetDocument3 pagesAlzheimer WorksheetRoberto Queiroz GomesNo ratings yet
- Chapter 7 Cystic FibrosisDocument9 pagesChapter 7 Cystic FibrosisMariana DariiNo ratings yet
- Solanum - Zombiepedia - FandomDocument5 pagesSolanum - Zombiepedia - FandomJohn SutphinNo ratings yet
- High Liver GGT EnzymesDocument4 pagesHigh Liver GGT EnzymesJavier Mendoza100% (2)
- Pregnancy Induced HypertensionDocument13 pagesPregnancy Induced HypertensionSally JaneNo ratings yet
- Common Dermatology Multiple Choice Questions and Answers - 6Document3 pagesCommon Dermatology Multiple Choice Questions and Answers - 6Atul Kumar Mishra100% (1)
- Microbiology, USMLE ENDPOINT (1) - 135-139Document5 pagesMicrobiology, USMLE ENDPOINT (1) - 135-139Yazan M Abu-FaraNo ratings yet
- Visitacion Act 1 Tdee Stats ReportDocument3 pagesVisitacion Act 1 Tdee Stats ReportHannah VisitacionNo ratings yet