
Rise and Fall
Rise and Fall
You might also like
- Reborn Apocalypse (A LitRPGWuxia Story) (Volume 1) (Kerr L.M.)Document515 pagesReborn Apocalypse (A LitRPGWuxia Story) (Volume 1) (Kerr L.M.)julian vegaNo ratings yet
- The Profit Motive and Patient CareDocument448 pagesThe Profit Motive and Patient CareTCFdotorgNo ratings yet
- NSG 436 Analysis of A UDocument6 pagesNSG 436 Analysis of A Uapi-521018364No ratings yet
- Cross Roads in Quality 2008Hlth AffairsDocument11 pagesCross Roads in Quality 2008Hlth AffairsVaida BankauskaiteNo ratings yet
- Further Reading 1Document24 pagesFurther Reading 1varian90No ratings yet
- Susan LoDocument10 pagesSusan Loapi-241538935No ratings yet
- American Medicine: The Quest for CompetenceFrom EverandAmerican Medicine: The Quest for CompetenceRating: 3 out of 5 stars3/5 (1)
- Health Care Reform Research Paper OutlineDocument7 pagesHealth Care Reform Research Paper Outlinevguomivnd100% (1)
- Research Paper On Health Care ReformDocument4 pagesResearch Paper On Health Care Reformgz7vhnpe100% (1)
- Changes in Hospital Competitive StrategyDocument23 pagesChanges in Hospital Competitive Strategyanantomi100% (1)
- Oh P Delivery SystemDocument14 pagesOh P Delivery SystemfrendirachmadNo ratings yet
- Jurnal HBMDocument10 pagesJurnal HBMSeindz OstenNo ratings yet
- And Purpose of Research: It Will Seek To Answer The Following QuestionsDocument91 pagesAnd Purpose of Research: It Will Seek To Answer The Following QuestionsAlex ClarkeNo ratings yet
- Nejmsa 063682Document8 pagesNejmsa 063682kehonemirandaNo ratings yet
- And Purpose of ResearchDocument42 pagesAnd Purpose of ResearchAlex ClarkeNo ratings yet
- FRANCO CreationHealthConsumerDocument21 pagesFRANCO CreationHealthConsumerRogerio Lima BarbosaNo ratings yet
- Analysis of Health Care System Initiatives in MA and SF, CA (Function, Cost, Outcome)Document7 pagesAnalysis of Health Care System Initiatives in MA and SF, CA (Function, Cost, Outcome)Wonder LostNo ratings yet
- Primary Health Care in CanadaDocument33 pagesPrimary Health Care in CanadaTengiz VerulavaNo ratings yet
- Managed CareDocument7 pagesManaged Carearun901No ratings yet
- Health Care Solutions From America's Business Community: The Path Forward For U.S. Health ReformDocument67 pagesHealth Care Solutions From America's Business Community: The Path Forward For U.S. Health ReformU.S. Chamber of CommerceNo ratings yet
- LWV RecentHealthCareChangesDocument4 pagesLWV RecentHealthCareChangesjrfh50No ratings yet
- United States Health Care Reform Progress To Date and Next StepsDocument9 pagesUnited States Health Care Reform Progress To Date and Next StepsEva MaglinteCanonNo ratings yet
- Research Paper Health Care ReformDocument4 pagesResearch Paper Health Care Reformsjcuwurif100% (1)
- Longman, Phillip - Vista Total Health - 20101005Document19 pagesLongman, Phillip - Vista Total Health - 20101005Sam SunshineNo ratings yet
- Answer 1Document8 pagesAnswer 1Hezekiah AtindaNo ratings yet
- Transformative Planning: How Your Healthcare Organization Can Strategize for an Uncertain FutureFrom EverandTransformative Planning: How Your Healthcare Organization Can Strategize for an Uncertain FutureNo ratings yet
- Health Care Reform - Why So Much Talk and So Little Action?: PerspectiveDocument2 pagesHealth Care Reform - Why So Much Talk and So Little Action?: PerspectiveKizito LubanoNo ratings yet
- Gaynor Et Al Final Report v11Document40 pagesGaynor Et Al Final Report v11padmanaban manickavelanNo ratings yet
- Health Care Reform DissertationDocument6 pagesHealth Care Reform DissertationDoMyPaperForMeEverett100% (1)
- Controlling Hospital Cost Inflation NewDocument14 pagesControlling Hospital Cost Inflation Newnasru hajiNo ratings yet
- Healthcare Policy Names InstitutionDocument29 pagesHealthcare Policy Names InstitutionMaestro WritersNo ratings yet
- TennCare, One State's Experiment with Medicaid ExpansionFrom EverandTennCare, One State's Experiment with Medicaid ExpansionNo ratings yet
- Evidence Based SurgeryDocument2 pagesEvidence Based SurgeryMegan LewisNo ratings yet
- Healthy Competition: What's Holding Back Health Care and How to Free ItFrom EverandHealthy Competition: What's Holding Back Health Care and How to Free ItNo ratings yet
- Policy at The Intersection of Health, Health Care andDocument21 pagesPolicy at The Intersection of Health, Health Care andIsmaNo ratings yet
- Senate Hearing, 111TH Congress - Delivery Reform: The Roles of Primary and Specialty Care in Innovative New Delivery ModelsDocument65 pagesSenate Hearing, 111TH Congress - Delivery Reform: The Roles of Primary and Specialty Care in Innovative New Delivery ModelsScribd Government DocsNo ratings yet
- Reforming The Swedish Health Services - The International Context.Document13 pagesReforming The Swedish Health Services - The International Context.Junca VictorNo ratings yet
- Imelda Mcdermott, Lynsey Warwick-Giles, Oz Gore, Valerie Moran, Donna Bramwell, Anna Coleman, and Kath ChecklandDocument11 pagesImelda Mcdermott, Lynsey Warwick-Giles, Oz Gore, Valerie Moran, Donna Bramwell, Anna Coleman, and Kath ChecklandhppnukNo ratings yet
- Solution Manual For American Public Policy An Introduction 11th EditionDocument19 pagesSolution Manual For American Public Policy An Introduction 11th EditionScottWyattognje100% (47)
- Research Paper On Healthcare in The United StatesDocument8 pagesResearch Paper On Healthcare in The United Statesafedetbma100% (1)
- Health Care Policy and Delivery Systems SyllabusDocument6 pagesHealth Care Policy and Delivery Systems SyllabusDeekay100% (1)
- Eview F Herapeutics: Economic Evaluations of Clinical Pharmacy Services: 2006 - 2010Document23 pagesEview F Herapeutics: Economic Evaluations of Clinical Pharmacy Services: 2006 - 2010Igor SilvaNo ratings yet
- AHA Patient Centered Medical HomeDocument21 pagesAHA Patient Centered Medical Homein678No ratings yet
- Medicina Basada en La EvidenciaDocument6 pagesMedicina Basada en La EvidenciaJulivaiNo ratings yet
- Analyzing The Different Socio Economic Factors Affecting The Demand For Health Care Facilities and Services in The Province of PampangaDocument15 pagesAnalyzing The Different Socio Economic Factors Affecting The Demand For Health Care Facilities and Services in The Province of PampangaMaxine GarraNo ratings yet
- 1 bmj00038-0042Document4 pages1 bmj00038-0042Sam GuillermoNo ratings yet
- WHAT CONCERNS CMOs IN THE MOVE FROM VOLUME TO VALUEDocument5 pagesWHAT CONCERNS CMOs IN THE MOVE FROM VOLUME TO VALUERussell ThayerNo ratings yet
- NJHCFFA Final ReportDocument111 pagesNJHCFFA Final ReportHealthcare FinanceNo ratings yet
- Political Analysis of Health Reform in The Dominican RepublicDocument12 pagesPolitical Analysis of Health Reform in The Dominican RepublicMarcel MejiaNo ratings yet
- No 362524 3Document5 pagesNo 362524 3My EscrowNo ratings yet
- Why Not User Charges? The Real Issues: Greg Stoddart Morris Barer Robert Evans Vandna BhatiaDocument34 pagesWhy Not User Charges? The Real Issues: Greg Stoddart Morris Barer Robert Evans Vandna BhatiaUmair JumaniNo ratings yet
- Responding to Healthcare Reform: A Strategy Guide for Healthcare LeadersFrom EverandResponding to Healthcare Reform: A Strategy Guide for Healthcare LeadersNo ratings yet
- The Impactofthe Affordable Care Acton North Carolinas Uninsured PopulationDocument6 pagesThe Impactofthe Affordable Care Acton North Carolinas Uninsured PopulationLori A. DixonNo ratings yet
- Kinney: The Potential of Captive Medical Liability Insurance Carriers and Damage Caps For Real Malpractice ReformDocument15 pagesKinney: The Potential of Captive Medical Liability Insurance Carriers and Damage Caps For Real Malpractice ReformNew England Law ReviewNo ratings yet
- Case Study LifeSpanDocument17 pagesCase Study LifeSpanxebraNo ratings yet
- Lang - Diskusija ObameDocument7 pagesLang - Diskusija ObameanlaucNo ratings yet
- Ogl 481 Choosing An Org CompletedDocument4 pagesOgl 481 Choosing An Org Completedapi-701146001No ratings yet
- TAVR CostsDocument11 pagesTAVR CostsTom BiusoNo ratings yet
- Healthy DietsDocument17 pagesHealthy DietsTom BiusoNo ratings yet
- C SuiteDocument10 pagesC SuiteTom BiusoNo ratings yet
- Bill Evans - Quiet NowDocument9 pagesBill Evans - Quiet NowTom Biuso100% (2)
- SGLT2 IDocument23 pagesSGLT2 ITom BiusoNo ratings yet
- PE AcquisitionDocument3 pagesPE AcquisitionTom BiusoNo ratings yet
- Chronic Kidney DiseaseDocument12 pagesChronic Kidney DiseaseTom BiusoNo ratings yet
- HL-474834 PreviewDocument2 pagesHL-474834 PreviewTom BiusoNo ratings yet
- Insurer Market PowerDocument7 pagesInsurer Market PowerTom BiusoNo ratings yet
- STLDDocument9 pagesSTLDTom BiusoNo ratings yet
- TAVR Low RiskDocument5 pagesTAVR Low RiskTom BiusoNo ratings yet
- Capital StructureDocument12 pagesCapital StructureTom BiusoNo ratings yet
- ECGsDocument4 pagesECGsTom BiusoNo ratings yet
- Aortic StenosisDocument11 pagesAortic StenosisTom BiusoNo ratings yet
- Pharmacologic Diabetes 2022Document19 pagesPharmacologic Diabetes 2022Tom BiusoNo ratings yet
- Where To InvestDocument7 pagesWhere To InvestTom BiusoNo ratings yet
- NCDRDocument9 pagesNCDRTom BiusoNo ratings yet
- Home Based CareDocument13 pagesHome Based CareTom BiusoNo ratings yet
- Acute Inferior Wall Myocardial Infarction: What Is The Culprit Artery?Document3 pagesAcute Inferior Wall Myocardial Infarction: What Is The Culprit Artery?Tom BiusoNo ratings yet
- How Should I Use Rapid COVID Tests?: and Why We Desperately Need More of ThemDocument10 pagesHow Should I Use Rapid COVID Tests?: and Why We Desperately Need More of ThemTom BiusoNo ratings yet
- Cardiovascular Diabetes 2022Document31 pagesCardiovascular Diabetes 2022Tom BiusoNo ratings yet
- Anaphylaxis: Emergency Department TreatmentDocument14 pagesAnaphylaxis: Emergency Department TreatmentTom BiusoNo ratings yet
- When Do I Give Fluids?Document14 pagesWhen Do I Give Fluids?Tom BiusoNo ratings yet
- Guidelines PDFDocument12 pagesGuidelines PDFTom BiusoNo ratings yet
- The Medical Letter: On Drugs and TherapeuticsDocument11 pagesThe Medical Letter: On Drugs and TherapeuticsTom BiusoNo ratings yet
- COVID-19 Vaccines - Final VersionDocument11 pagesCOVID-19 Vaccines - Final VersionTom BiusoNo ratings yet
- Ngspice ManualDocument592 pagesNgspice ManualRommel Joshua OrtegaNo ratings yet
- Data Science HindiDocument29 pagesData Science HindiSyed Bilal Armaan100% (2)
- Flight InstrumentsDocument42 pagesFlight InstrumentsShiwani HoodaNo ratings yet
- De Thi Thu TN THPT 2024 Tieng Anh So GD Ha NoiDocument23 pagesDe Thi Thu TN THPT 2024 Tieng Anh So GD Ha NoiQuang Lê Hồ DuyNo ratings yet
- Bearing Inspection SOPDocument7 pagesBearing Inspection SOPRianAwangga100% (1)
- CMC Vellore Admission InstructionsDocument57 pagesCMC Vellore Admission InstructionsNaveen JaiNo ratings yet
- Listening and Note-Taking Week 01Document6 pagesListening and Note-Taking Week 01AlvinPennNo ratings yet
- Quantum Tunneling and Spin 14Document14 pagesQuantum Tunneling and Spin 14plfratarNo ratings yet
- Expansion of LiquidsDocument2 pagesExpansion of LiquidsKenith GamageNo ratings yet
- Lesson 2Document16 pagesLesson 2Vusani NeguyuniNo ratings yet
- History: The History of The Hospitality Industry Dates All The WayDocument10 pagesHistory: The History of The Hospitality Industry Dates All The WaySAKET TYAGINo ratings yet
- Communication Protocol For T300CDocument14 pagesCommunication Protocol For T300CChristian Vásquez SánchezNo ratings yet
- Jeppview For Windows: General Information Communication Information General InformationDocument34 pagesJeppview For Windows: General Information Communication Information General InformationAviation WithvoiceNo ratings yet
- Mooka's Pancha ShatiDocument16 pagesMooka's Pancha ShatiSudarsanan NesamonyNo ratings yet
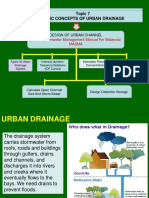
- Topic 7 Basic Concepts of Urban Drainage: (Urban Stormwater Management Manual For Malaysia) MasmaDocument29 pagesTopic 7 Basic Concepts of Urban Drainage: (Urban Stormwater Management Manual For Malaysia) MasmaAzhar SabriNo ratings yet
- AIS (Automatic Identification System) WorkingDocument8 pagesAIS (Automatic Identification System) Workingkhanjamil1250% (2)
- 0743 Windows 10 Backup Restore PDFDocument11 pages0743 Windows 10 Backup Restore PDFsumyNo ratings yet
- 211-Article Text-399-1-10-20180522 PDFDocument42 pages211-Article Text-399-1-10-20180522 PDFAlex KanathNo ratings yet
- Short Notes For Heat Transfer - Docx 97.docx 93Document18 pagesShort Notes For Heat Transfer - Docx 97.docx 93kumarsumit1942No ratings yet
- Ques Risk and Return & CAPM (S-17Revised)Document6 pagesQues Risk and Return & CAPM (S-17Revised)Najia SiddiquiNo ratings yet
- Analyzing IoT Data in Python Chapter1Document27 pagesAnalyzing IoT Data in Python Chapter1FgpeqwNo ratings yet
- Memory Hierarchy & Cache MemoryDocument40 pagesMemory Hierarchy & Cache MemorybiliNo ratings yet
- Chronic Suppurative Otitis MediaDocument37 pagesChronic Suppurative Otitis Media43 Mohamed RazikNo ratings yet
- HK TSA Writing Paper 2 2020 - 3ERW2Document12 pagesHK TSA Writing Paper 2 2020 - 3ERW2RachelNo ratings yet
- GeM Bidding 4660207Document5 pagesGeM Bidding 4660207Hemanth KumarNo ratings yet
- Surajs Nair Resume 5Document4 pagesSurajs Nair Resume 5suraj.sNo ratings yet
- Method Statement Ceiling RemovalDocument7 pagesMethod Statement Ceiling RemovalSimpol MathNo ratings yet
- Forestry QuestionnaireDocument5 pagesForestry QuestionnaireJasmin QuebidoNo ratings yet
- System Analysis & Design in A Changing World Chapter 13 Problems and ExercisesDocument8 pagesSystem Analysis & Design in A Changing World Chapter 13 Problems and ExercisesbriandonaldNo ratings yet


















































































































Download as pdf or txt
You might also like
- Reborn Apocalypse (A LitRPGWuxia Story) (Volume 1) (Kerr L.M.)Document515 pagesReborn Apocalypse (A LitRPGWuxia Story) (Volume 1) (Kerr L.M.)julian vegaNo ratings yet
- The Profit Motive and Patient CareDocument448 pagesThe Profit Motive and Patient CareTCFdotorgNo ratings yet
- NSG 436 Analysis of A UDocument6 pagesNSG 436 Analysis of A Uapi-521018364No ratings yet
- Cross Roads in Quality 2008Hlth AffairsDocument11 pagesCross Roads in Quality 2008Hlth AffairsVaida BankauskaiteNo ratings yet
- Further Reading 1Document24 pagesFurther Reading 1varian90No ratings yet
- Susan LoDocument10 pagesSusan Loapi-241538935No ratings yet
- American Medicine: The Quest for CompetenceFrom EverandAmerican Medicine: The Quest for CompetenceRating: 3 out of 5 stars3/5 (1)
- Health Care Reform Research Paper OutlineDocument7 pagesHealth Care Reform Research Paper Outlinevguomivnd100% (1)
- Research Paper On Health Care ReformDocument4 pagesResearch Paper On Health Care Reformgz7vhnpe100% (1)
- Changes in Hospital Competitive StrategyDocument23 pagesChanges in Hospital Competitive Strategyanantomi100% (1)
- Oh P Delivery SystemDocument14 pagesOh P Delivery SystemfrendirachmadNo ratings yet
- Jurnal HBMDocument10 pagesJurnal HBMSeindz OstenNo ratings yet
- And Purpose of Research: It Will Seek To Answer The Following QuestionsDocument91 pagesAnd Purpose of Research: It Will Seek To Answer The Following QuestionsAlex ClarkeNo ratings yet
- Nejmsa 063682Document8 pagesNejmsa 063682kehonemirandaNo ratings yet
- And Purpose of ResearchDocument42 pagesAnd Purpose of ResearchAlex ClarkeNo ratings yet
- FRANCO CreationHealthConsumerDocument21 pagesFRANCO CreationHealthConsumerRogerio Lima BarbosaNo ratings yet
- Analysis of Health Care System Initiatives in MA and SF, CA (Function, Cost, Outcome)Document7 pagesAnalysis of Health Care System Initiatives in MA and SF, CA (Function, Cost, Outcome)Wonder LostNo ratings yet
- Primary Health Care in CanadaDocument33 pagesPrimary Health Care in CanadaTengiz VerulavaNo ratings yet
- Managed CareDocument7 pagesManaged Carearun901No ratings yet
- Health Care Solutions From America's Business Community: The Path Forward For U.S. Health ReformDocument67 pagesHealth Care Solutions From America's Business Community: The Path Forward For U.S. Health ReformU.S. Chamber of CommerceNo ratings yet
- LWV RecentHealthCareChangesDocument4 pagesLWV RecentHealthCareChangesjrfh50No ratings yet
- United States Health Care Reform Progress To Date and Next StepsDocument9 pagesUnited States Health Care Reform Progress To Date and Next StepsEva MaglinteCanonNo ratings yet
- Research Paper Health Care ReformDocument4 pagesResearch Paper Health Care Reformsjcuwurif100% (1)
- Longman, Phillip - Vista Total Health - 20101005Document19 pagesLongman, Phillip - Vista Total Health - 20101005Sam SunshineNo ratings yet
- Answer 1Document8 pagesAnswer 1Hezekiah AtindaNo ratings yet
- Transformative Planning: How Your Healthcare Organization Can Strategize for an Uncertain FutureFrom EverandTransformative Planning: How Your Healthcare Organization Can Strategize for an Uncertain FutureNo ratings yet
- Health Care Reform - Why So Much Talk and So Little Action?: PerspectiveDocument2 pagesHealth Care Reform - Why So Much Talk and So Little Action?: PerspectiveKizito LubanoNo ratings yet
- Gaynor Et Al Final Report v11Document40 pagesGaynor Et Al Final Report v11padmanaban manickavelanNo ratings yet
- Health Care Reform DissertationDocument6 pagesHealth Care Reform DissertationDoMyPaperForMeEverett100% (1)
- Controlling Hospital Cost Inflation NewDocument14 pagesControlling Hospital Cost Inflation Newnasru hajiNo ratings yet
- Healthcare Policy Names InstitutionDocument29 pagesHealthcare Policy Names InstitutionMaestro WritersNo ratings yet
- TennCare, One State's Experiment with Medicaid ExpansionFrom EverandTennCare, One State's Experiment with Medicaid ExpansionNo ratings yet
- Evidence Based SurgeryDocument2 pagesEvidence Based SurgeryMegan LewisNo ratings yet
- Healthy Competition: What's Holding Back Health Care and How to Free ItFrom EverandHealthy Competition: What's Holding Back Health Care and How to Free ItNo ratings yet
- Policy at The Intersection of Health, Health Care andDocument21 pagesPolicy at The Intersection of Health, Health Care andIsmaNo ratings yet
- Senate Hearing, 111TH Congress - Delivery Reform: The Roles of Primary and Specialty Care in Innovative New Delivery ModelsDocument65 pagesSenate Hearing, 111TH Congress - Delivery Reform: The Roles of Primary and Specialty Care in Innovative New Delivery ModelsScribd Government DocsNo ratings yet
- Reforming The Swedish Health Services - The International Context.Document13 pagesReforming The Swedish Health Services - The International Context.Junca VictorNo ratings yet
- Imelda Mcdermott, Lynsey Warwick-Giles, Oz Gore, Valerie Moran, Donna Bramwell, Anna Coleman, and Kath ChecklandDocument11 pagesImelda Mcdermott, Lynsey Warwick-Giles, Oz Gore, Valerie Moran, Donna Bramwell, Anna Coleman, and Kath ChecklandhppnukNo ratings yet
- Solution Manual For American Public Policy An Introduction 11th EditionDocument19 pagesSolution Manual For American Public Policy An Introduction 11th EditionScottWyattognje100% (47)
- Research Paper On Healthcare in The United StatesDocument8 pagesResearch Paper On Healthcare in The United Statesafedetbma100% (1)
- Health Care Policy and Delivery Systems SyllabusDocument6 pagesHealth Care Policy and Delivery Systems SyllabusDeekay100% (1)
- Eview F Herapeutics: Economic Evaluations of Clinical Pharmacy Services: 2006 - 2010Document23 pagesEview F Herapeutics: Economic Evaluations of Clinical Pharmacy Services: 2006 - 2010Igor SilvaNo ratings yet
- AHA Patient Centered Medical HomeDocument21 pagesAHA Patient Centered Medical Homein678No ratings yet
- Medicina Basada en La EvidenciaDocument6 pagesMedicina Basada en La EvidenciaJulivaiNo ratings yet
- Analyzing The Different Socio Economic Factors Affecting The Demand For Health Care Facilities and Services in The Province of PampangaDocument15 pagesAnalyzing The Different Socio Economic Factors Affecting The Demand For Health Care Facilities and Services in The Province of PampangaMaxine GarraNo ratings yet
- 1 bmj00038-0042Document4 pages1 bmj00038-0042Sam GuillermoNo ratings yet
- WHAT CONCERNS CMOs IN THE MOVE FROM VOLUME TO VALUEDocument5 pagesWHAT CONCERNS CMOs IN THE MOVE FROM VOLUME TO VALUERussell ThayerNo ratings yet
- NJHCFFA Final ReportDocument111 pagesNJHCFFA Final ReportHealthcare FinanceNo ratings yet
- Political Analysis of Health Reform in The Dominican RepublicDocument12 pagesPolitical Analysis of Health Reform in The Dominican RepublicMarcel MejiaNo ratings yet
- No 362524 3Document5 pagesNo 362524 3My EscrowNo ratings yet
- Why Not User Charges? The Real Issues: Greg Stoddart Morris Barer Robert Evans Vandna BhatiaDocument34 pagesWhy Not User Charges? The Real Issues: Greg Stoddart Morris Barer Robert Evans Vandna BhatiaUmair JumaniNo ratings yet
- Responding to Healthcare Reform: A Strategy Guide for Healthcare LeadersFrom EverandResponding to Healthcare Reform: A Strategy Guide for Healthcare LeadersNo ratings yet
- The Impactofthe Affordable Care Acton North Carolinas Uninsured PopulationDocument6 pagesThe Impactofthe Affordable Care Acton North Carolinas Uninsured PopulationLori A. DixonNo ratings yet
- Kinney: The Potential of Captive Medical Liability Insurance Carriers and Damage Caps For Real Malpractice ReformDocument15 pagesKinney: The Potential of Captive Medical Liability Insurance Carriers and Damage Caps For Real Malpractice ReformNew England Law ReviewNo ratings yet
- Case Study LifeSpanDocument17 pagesCase Study LifeSpanxebraNo ratings yet
- Lang - Diskusija ObameDocument7 pagesLang - Diskusija ObameanlaucNo ratings yet
- Ogl 481 Choosing An Org CompletedDocument4 pagesOgl 481 Choosing An Org Completedapi-701146001No ratings yet
- TAVR CostsDocument11 pagesTAVR CostsTom BiusoNo ratings yet
- Healthy DietsDocument17 pagesHealthy DietsTom BiusoNo ratings yet
- C SuiteDocument10 pagesC SuiteTom BiusoNo ratings yet
- Bill Evans - Quiet NowDocument9 pagesBill Evans - Quiet NowTom Biuso100% (2)
- SGLT2 IDocument23 pagesSGLT2 ITom BiusoNo ratings yet
- PE AcquisitionDocument3 pagesPE AcquisitionTom BiusoNo ratings yet
- Chronic Kidney DiseaseDocument12 pagesChronic Kidney DiseaseTom BiusoNo ratings yet
- HL-474834 PreviewDocument2 pagesHL-474834 PreviewTom BiusoNo ratings yet
- Insurer Market PowerDocument7 pagesInsurer Market PowerTom BiusoNo ratings yet
- STLDDocument9 pagesSTLDTom BiusoNo ratings yet
- TAVR Low RiskDocument5 pagesTAVR Low RiskTom BiusoNo ratings yet
- Capital StructureDocument12 pagesCapital StructureTom BiusoNo ratings yet
- ECGsDocument4 pagesECGsTom BiusoNo ratings yet
- Aortic StenosisDocument11 pagesAortic StenosisTom BiusoNo ratings yet
- Pharmacologic Diabetes 2022Document19 pagesPharmacologic Diabetes 2022Tom BiusoNo ratings yet
- Where To InvestDocument7 pagesWhere To InvestTom BiusoNo ratings yet
- NCDRDocument9 pagesNCDRTom BiusoNo ratings yet
- Home Based CareDocument13 pagesHome Based CareTom BiusoNo ratings yet
- Acute Inferior Wall Myocardial Infarction: What Is The Culprit Artery?Document3 pagesAcute Inferior Wall Myocardial Infarction: What Is The Culprit Artery?Tom BiusoNo ratings yet
- How Should I Use Rapid COVID Tests?: and Why We Desperately Need More of ThemDocument10 pagesHow Should I Use Rapid COVID Tests?: and Why We Desperately Need More of ThemTom BiusoNo ratings yet
- Cardiovascular Diabetes 2022Document31 pagesCardiovascular Diabetes 2022Tom BiusoNo ratings yet
- Anaphylaxis: Emergency Department TreatmentDocument14 pagesAnaphylaxis: Emergency Department TreatmentTom BiusoNo ratings yet
- When Do I Give Fluids?Document14 pagesWhen Do I Give Fluids?Tom BiusoNo ratings yet
- Guidelines PDFDocument12 pagesGuidelines PDFTom BiusoNo ratings yet
- The Medical Letter: On Drugs and TherapeuticsDocument11 pagesThe Medical Letter: On Drugs and TherapeuticsTom BiusoNo ratings yet
- COVID-19 Vaccines - Final VersionDocument11 pagesCOVID-19 Vaccines - Final VersionTom BiusoNo ratings yet
- Ngspice ManualDocument592 pagesNgspice ManualRommel Joshua OrtegaNo ratings yet
- Data Science HindiDocument29 pagesData Science HindiSyed Bilal Armaan100% (2)
- Flight InstrumentsDocument42 pagesFlight InstrumentsShiwani HoodaNo ratings yet
- De Thi Thu TN THPT 2024 Tieng Anh So GD Ha NoiDocument23 pagesDe Thi Thu TN THPT 2024 Tieng Anh So GD Ha NoiQuang Lê Hồ DuyNo ratings yet
- Bearing Inspection SOPDocument7 pagesBearing Inspection SOPRianAwangga100% (1)
- CMC Vellore Admission InstructionsDocument57 pagesCMC Vellore Admission InstructionsNaveen JaiNo ratings yet
- Listening and Note-Taking Week 01Document6 pagesListening and Note-Taking Week 01AlvinPennNo ratings yet
- Quantum Tunneling and Spin 14Document14 pagesQuantum Tunneling and Spin 14plfratarNo ratings yet
- Expansion of LiquidsDocument2 pagesExpansion of LiquidsKenith GamageNo ratings yet
- Lesson 2Document16 pagesLesson 2Vusani NeguyuniNo ratings yet
- History: The History of The Hospitality Industry Dates All The WayDocument10 pagesHistory: The History of The Hospitality Industry Dates All The WaySAKET TYAGINo ratings yet
- Communication Protocol For T300CDocument14 pagesCommunication Protocol For T300CChristian Vásquez SánchezNo ratings yet
- Jeppview For Windows: General Information Communication Information General InformationDocument34 pagesJeppview For Windows: General Information Communication Information General InformationAviation WithvoiceNo ratings yet
- Mooka's Pancha ShatiDocument16 pagesMooka's Pancha ShatiSudarsanan NesamonyNo ratings yet
- Topic 7 Basic Concepts of Urban Drainage: (Urban Stormwater Management Manual For Malaysia) MasmaDocument29 pagesTopic 7 Basic Concepts of Urban Drainage: (Urban Stormwater Management Manual For Malaysia) MasmaAzhar SabriNo ratings yet
- AIS (Automatic Identification System) WorkingDocument8 pagesAIS (Automatic Identification System) Workingkhanjamil1250% (2)
- 0743 Windows 10 Backup Restore PDFDocument11 pages0743 Windows 10 Backup Restore PDFsumyNo ratings yet
- 211-Article Text-399-1-10-20180522 PDFDocument42 pages211-Article Text-399-1-10-20180522 PDFAlex KanathNo ratings yet
- Short Notes For Heat Transfer - Docx 97.docx 93Document18 pagesShort Notes For Heat Transfer - Docx 97.docx 93kumarsumit1942No ratings yet
- Ques Risk and Return & CAPM (S-17Revised)Document6 pagesQues Risk and Return & CAPM (S-17Revised)Najia SiddiquiNo ratings yet
- Analyzing IoT Data in Python Chapter1Document27 pagesAnalyzing IoT Data in Python Chapter1FgpeqwNo ratings yet
- Memory Hierarchy & Cache MemoryDocument40 pagesMemory Hierarchy & Cache MemorybiliNo ratings yet
- Chronic Suppurative Otitis MediaDocument37 pagesChronic Suppurative Otitis Media43 Mohamed RazikNo ratings yet
- HK TSA Writing Paper 2 2020 - 3ERW2Document12 pagesHK TSA Writing Paper 2 2020 - 3ERW2RachelNo ratings yet
- GeM Bidding 4660207Document5 pagesGeM Bidding 4660207Hemanth KumarNo ratings yet
- Surajs Nair Resume 5Document4 pagesSurajs Nair Resume 5suraj.sNo ratings yet
- Method Statement Ceiling RemovalDocument7 pagesMethod Statement Ceiling RemovalSimpol MathNo ratings yet
- Forestry QuestionnaireDocument5 pagesForestry QuestionnaireJasmin QuebidoNo ratings yet
- System Analysis & Design in A Changing World Chapter 13 Problems and ExercisesDocument8 pagesSystem Analysis & Design in A Changing World Chapter 13 Problems and ExercisesbriandonaldNo ratings yet