Download as pdf or txt
You might also like
- Full Download Comprehensive Medical Assisting Administrative and Clinical Competencies 6th Edition Lindh Solutions Manual PDF Full ChapterDocument35 pagesFull Download Comprehensive Medical Assisting Administrative and Clinical Competencies 6th Edition Lindh Solutions Manual PDF Full Chapterboxengoliardgpd40100% (20)
- Cidesco Case Histories BookletDocument11 pagesCidesco Case Histories Bookletmatina papaspyrou100% (1)
- Massage and All Facial Tratments (AutoRecovered)Document9 pagesMassage and All Facial Tratments (AutoRecovered)Vivi AnaNo ratings yet
- Case Study 5Document9 pagesCase Study 5Vivi AnaNo ratings yet
- Case Study Template BeautyDocument8 pagesCase Study Template BeautyVivi AnaNo ratings yet
- Case Study Template BeautyDocument8 pagesCase Study Template BeautyVivi VivianaNo ratings yet
- Facial Client Intake Form: by Signing This Form, The Client Agrees To The FollowingDocument1 pageFacial Client Intake Form: by Signing This Form, The Client Agrees To The Followingarasan2297No ratings yet
- Treatment Evidence Form: iUBT431 - Facial Electrical TreatmentsDocument5 pagesTreatment Evidence Form: iUBT431 - Facial Electrical TreatmentsVivi AnaNo ratings yet
- PENGKAJIANDocument3 pagesPENGKAJIANIRSAD SADAMNo ratings yet
- 37901-IUBT353 Treatment Evidence Form v1Document4 pages37901-IUBT353 Treatment Evidence Form v1MoreblessingNo ratings yet
- Whitereyes - Ocular/Medical/General Information: Glasses HistoryDocument6 pagesWhitereyes - Ocular/Medical/General Information: Glasses HistoryAnand PatelNo ratings yet
- 36316-IUCT22 Client Consultation Form v1Document7 pages36316-IUCT22 Client Consultation Form v1michellepayne1806No ratings yet
- Peme Form B - Rev 20201020Document5 pagesPeme Form B - Rev 20201020Click TechnologyNo ratings yet
- PEME - Form B - Rev.29.10Document4 pagesPEME - Form B - Rev.29.10Hector ValleNo ratings yet
- First Aid Kit Cheat Sheet: by ViaDocument1 pageFirst Aid Kit Cheat Sheet: by ViaKathlene YuNo ratings yet
- External Eye DiseasesDocument15 pagesExternal Eye Diseasesmarianne.bilaoen09No ratings yet
- New Patient Medical History Form 2023 03 29Document2 pagesNew Patient Medical History Form 2023 03 29Trouvaille medicoNo ratings yet
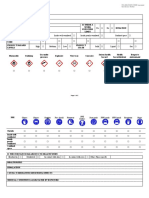
- COSHH AssessmentDocument5 pagesCOSHH AssessmentGlen StrakerNo ratings yet
- COSHH AssessmentDocument5 pagesCOSHH AssessmentGlen StrakerNo ratings yet
- Substance / Material Suppliers Address and Phone Number Contents / Ingredients of Product Is There A Work Exposure Limit DurationDocument4 pagesSubstance / Material Suppliers Address and Phone Number Contents / Ingredients of Product Is There A Work Exposure Limit DurationAli Salih100% (1)
- 009 Incident Investigation Report-Kantilo-2Document5 pages009 Incident Investigation Report-Kantilo-2Er Jyotirmaya DalaiNo ratings yet
- 37821-iUCT32 Consultation Form v2Document11 pages37821-iUCT32 Consultation Form v2taraturgooseNo ratings yet
- CP1 - Baiq Regita Cahyami Surya (H1A016016)Document39 pagesCP1 - Baiq Regita Cahyami Surya (H1A016016)Baiq RegitaNo ratings yet
- Injury or Illness Investigation Report Document Ref. Ama-Hs-Frm-0012 H&S Management Revision 00Document3 pagesInjury or Illness Investigation Report Document Ref. Ama-Hs-Frm-0012 H&S Management Revision 00Idris AdeniranNo ratings yet
- Red Eye - Conjunctivitis I Dr. Nuke Erlina Mayasari, SPMDocument23 pagesRed Eye - Conjunctivitis I Dr. Nuke Erlina Mayasari, SPMismkipendprowil2No ratings yet
- Chronic Wound Managment HMIDocument37 pagesChronic Wound Managment HMIannisa edwarNo ratings yet
- iUBT320 - Treatment - Evidence - Form - Back & Neck MassageDocument4 pagesiUBT320 - Treatment - Evidence - Form - Back & Neck MassageNomsaNo ratings yet
- Cossh Risk Assessment - E45 Barrier CreamDocument3 pagesCossh Risk Assessment - E45 Barrier CreamKishor KoshyNo ratings yet
- Health Assessment Proforma of School StudentsDocument4 pagesHealth Assessment Proforma of School StudentsMantu Roy100% (1)
- L5 - Ocular Emergencies and Red EyeDocument35 pagesL5 - Ocular Emergencies and Red EyeConger CongerNo ratings yet
- Waxing Full LegDocument4 pagesWaxing Full LegLionel YdeNo ratings yet
- Hem - Onc ReviewDocument70 pagesHem - Onc Reviewshellers24No ratings yet
- Wound Management MDocument43 pagesWound Management MMeenuNo ratings yet
- Packing List TravelfornoobsDocument3 pagesPacking List TravelfornoobsFlávia ViduedoNo ratings yet
- IELTS Speaking September-December'22 2Document3 pagesIELTS Speaking September-December'22 2Гузель МаматкуловаNo ratings yet
- Categories and Sub-Categories Car Park Community Oil & GasDocument2 pagesCategories and Sub-Categories Car Park Community Oil & GasPhạm LinhNo ratings yet
- Earthworm Pre LabDocument2 pagesEarthworm Pre Labapi-342334216No ratings yet
- Hydration Risk Assessment Tool PDFDocument1 pageHydration Risk Assessment Tool PDFStan CiprianNo ratings yet
- Aberdeenvaricoseveinsquestionnaire PDFDocument4 pagesAberdeenvaricoseveinsquestionnaire PDFdesyislamiatiNo ratings yet
- Patient NameDocument2 pagesPatient NameShujaRehmanNo ratings yet
- PANAMADocument3 pagesPANAMA7vs8ndtrrcNo ratings yet
- COSHH Assessment Dulux Undercoat Oil BasedDocument3 pagesCOSHH Assessment Dulux Undercoat Oil BasedrajamohamdedhanaNo ratings yet
- Point of Work Assessment - Stop Think ActDocument1 pagePoint of Work Assessment - Stop Think ActgvengveNo ratings yet
- Pre-Departure List: DocumentsDocument3 pagesPre-Departure List: DocumentsfirearlymyNo ratings yet
- General ExaminationDocument31 pagesGeneral ExaminationjjNo ratings yet
- UntitledDocument56 pagesUntitledKal El AndayaNo ratings yet
- 3-Painless Red EyeDocument40 pages3-Painless Red Eyetaha obaidNo ratings yet
- Introduction To Endocrine Disorder - Common Short - 240317 - 180114Document57 pagesIntroduction To Endocrine Disorder - Common Short - 240317 - 180114Durrah Abd GafarNo ratings yet
- Employee Accident Report Form - PDFDocument6 pagesEmployee Accident Report Form - PDFthiruvilanNo ratings yet
- IBKV2 UAS Notes 2022Document24 pagesIBKV2 UAS Notes 2022Anna TohNo ratings yet
- Checklist CompilationDocument16 pagesChecklist CompilationMaria JuanilloNo ratings yet
- 06-05-2021 - Turaif - First Aid Injuries - Investigation ReportDocument6 pages06-05-2021 - Turaif - First Aid Injuries - Investigation ReportMohamedNo ratings yet
- Lecture Chronic Red EyeDocument25 pagesLecture Chronic Red Eyejustforfun219No ratings yet
- Ilmu Kesehatan Mata PDFDocument164 pagesIlmu Kesehatan Mata PDFTania Silvia Alexandra100% (1)
- New Patient Registration FormDocument4 pagesNew Patient Registration Formapi-358908929No ratings yet
- 01 - Sexual Anatomy and PhysiologyDocument6 pages01 - Sexual Anatomy and PhysiologyKyrriel CNo ratings yet
- FullChecklistRev10 22Document10 pagesFullChecklistRev10 22Vishmitha NNo ratings yet
- MicrobiologyDocument3 pagesMicrobiologyMuhammad HaneefNo ratings yet
- Arm WaxingDocument5 pagesArm Waxinggfmstn75jjNo ratings yet
- Tragedy Into Drama: An American History of Tourniquet Use in The Current WarDocument22 pagesTragedy Into Drama: An American History of Tourniquet Use in The Current Waraithor91No ratings yet
- Ipi 167868Document6 pagesIpi 167868M Isyhaduul IslamNo ratings yet
- (Download PDF) Expertddx Musculoskeletal 2Nd Edition Kirkland W Davis Online Ebook All Chapter PDFDocument42 pages(Download PDF) Expertddx Musculoskeletal 2Nd Edition Kirkland W Davis Online Ebook All Chapter PDFdennis.holbrook719100% (12)
- Therapeutic Options For Management of Pharyngoesophageal Corrosive StricturesDocument10 pagesTherapeutic Options For Management of Pharyngoesophageal Corrosive StricturesSuril VithalaniNo ratings yet
- Obat-Obat Yang Tersedia Di Klinik Pratama RizkyDocument2 pagesObat-Obat Yang Tersedia Di Klinik Pratama RizkyabdulrozakNo ratings yet
- 6 - Skill 3Document4 pages6 - Skill 3Adistya VirginNo ratings yet
- Philhealth Pre-Auth CataractDocument6 pagesPhilhealth Pre-Auth Cataractwmarasigan2610No ratings yet
- Daftar Harga 13 Agustus 2022Document27 pagesDaftar Harga 13 Agustus 2022Dhamar SetiaNo ratings yet
- NURS FPX 6612 Assessment 3 Patient Discharge Care PlanningDocument5 pagesNURS FPX 6612 Assessment 3 Patient Discharge Care Planningfarwaamjad771No ratings yet
- Prueba Traspasos 16.03.2024Document3,750 pagesPrueba Traspasos 16.03.2024albertoipc7No ratings yet
- The Tapecript IELTS Exercise 1Document5 pagesThe Tapecript IELTS Exercise 1DheaaNo ratings yet
- VerbosDocument14 pagesVerbosFrancisco CaballeroNo ratings yet
- Psychotropic Drugs II. Pharmacology. Pharmacotherapy. PharmacyDocument7 pagesPsychotropic Drugs II. Pharmacology. Pharmacotherapy. PharmacyJorge Medina FernandezNo ratings yet
- Collaborative Practice Agreement 2024Document3 pagesCollaborative Practice Agreement 2024marlontapit1115No ratings yet
- Rab Alkes PoliklinikDocument9 pagesRab Alkes PoliklinikWahyu saputraNo ratings yet
- What Are Casts Made Of?: Medical and Surgical Medicine Labe . Casting The CastDocument3 pagesWhat Are Casts Made Of?: Medical and Surgical Medicine Labe . Casting The Castزين آل راضيNo ratings yet
- MOHAMMED Health Passport 05-11-2022 1.1Document1 pageMOHAMMED Health Passport 05-11-2022 1.1EXPERTISE STORENo ratings yet
- Modul English 1 - MuklaDocument13 pagesModul English 1 - MuklaFia Nur HaryaniNo ratings yet
- X-Ray Technologists 06-2023Document7 pagesX-Ray Technologists 06-2023PRC BaguioNo ratings yet
- Physical Health Assessment Pre-Sim PrepDocument3 pagesPhysical Health Assessment Pre-Sim PrepaliNo ratings yet
- 1990 03 10-11 Kochi Proceeding Ay Seminar On CancerDocument160 pages1990 03 10-11 Kochi Proceeding Ay Seminar On CancerMSKCNo ratings yet
- Solna TR K 11809-23 Aktbil 2, Bilaga 1, BetalningsuppmaningDocument169 pagesSolna TR K 11809-23 Aktbil 2, Bilaga 1, BetalningsuppmaningvgarunachalNo ratings yet
- Core Measure Functional Gait Assessment - FinalDocument5 pagesCore Measure Functional Gait Assessment - FinalStefan AlbuNo ratings yet
- Item Description Total Tablets/units VerifierDocument7 pagesItem Description Total Tablets/units VerifierLions NgosuaniNo ratings yet
- Chapter 19Document8 pagesChapter 19knotstmNo ratings yet
- Pharmacy Technician Cover LetterDocument8 pagesPharmacy Technician Cover Lettergtbwf3g2100% (1)
- Dho Letter PNDTDocument5 pagesDho Letter PNDTNatvar M PatelNo ratings yet
- Montaje Luz Limitador Carga Fassi PDFDocument2 pagesMontaje Luz Limitador Carga Fassi PDFAlfredo Dominguez ArandaNo ratings yet
- Am24 Prelim Program-2Document16 pagesAm24 Prelim Program-2Jamshaid MirNo ratings yet