Download as pdf or txt
You might also like
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5834)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1093)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (852)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (590)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (903)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (541)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (350)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (824)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (122)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (405)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (74)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- Biomedx Workshop AgendaDocument6 pagesBiomedx Workshop AgendabiomedxNo ratings yet
- Parasnis - 1951 - Study Rock MidlandsDocument20 pagesParasnis - 1951 - Study Rock MidlandsIsaac KandaNo ratings yet
- Setting GuideDocument12 pagesSetting GuideJamesNo ratings yet
- Binary Vapor Liquid Equilibrium (Vle) Calculator PDFDocument11 pagesBinary Vapor Liquid Equilibrium (Vle) Calculator PDFSalman ZafarNo ratings yet
- Rahmania Tbi 6 D Soe...Document9 pagesRahmania Tbi 6 D Soe...Rahmania Aulia PurwagunifaNo ratings yet
- OceanofPDF - Com Strictly Research - Terry TowersDocument284 pagesOceanofPDF - Com Strictly Research - Terry TowersKenny SimNo ratings yet
- Testbank: Applying Ifrs Standards 4eDocument11 pagesTestbank: Applying Ifrs Standards 4eSyed Bilal AliNo ratings yet
- Georgina Smith - Resume 1Document3 pagesGeorgina Smith - Resume 1api-559062488No ratings yet
- Respuestas Evaluacion 1Document9 pagesRespuestas Evaluacion 1Juan Carlos Ospina ReyesNo ratings yet
- Labour Law and Employment in Slovakia - 2019 GuideDocument13 pagesLabour Law and Employment in Slovakia - 2019 GuideAccaceNo ratings yet
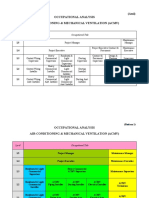
- Occupational StructureDocument3 pagesOccupational StructureEmirul FairuzNo ratings yet
- Gcrouch@wsu - Edu Rmancini@wsu - Edu Andreakl@wsu - Edu: Groups/chem.345Document5 pagesGcrouch@wsu - Edu Rmancini@wsu - Edu Andreakl@wsu - Edu: Groups/chem.345Daniel McDermottNo ratings yet
- Sir Syed University of Engineering & Technology.: OGDCL Internship Report 2021Document16 pagesSir Syed University of Engineering & Technology.: OGDCL Internship Report 2021Aisha KhanNo ratings yet
- BGR AnuualReport 2022-23Document88 pagesBGR AnuualReport 2022-23Rk SharafatNo ratings yet
- ADM Marketing Module 4 Lesson 4 Promotional ToolsDocument20 pagesADM Marketing Module 4 Lesson 4 Promotional ToolsMariel Santos75% (8)
- B.inggris-Daily ActivitiesDocument11 pagesB.inggris-Daily ActivitiesDadang SopianNo ratings yet
- 10 Best JobsitesDocument14 pages10 Best JobsitesHemansu PathakNo ratings yet
- (00 Cari) - Iso - 8466 1 1990Document5 pages(00 Cari) - Iso - 8466 1 1990faridsidikNo ratings yet
- BRR Course 5Document19 pagesBRR Course 5Wade SperryNo ratings yet
- 2018 Weekly CalendarDocument3 pages2018 Weekly CalendarFabian FebianoNo ratings yet
- Conceptual FrameworkDocument4 pagesConceptual FrameworkEustass KiddNo ratings yet
- UpsDocument31 pagesUpsThuyaNo ratings yet
- Edc 2Document103 pagesEdc 2abhi_engg06No ratings yet
- Ozone Therapy Is Safest Known TherapyDocument35 pagesOzone Therapy Is Safest Known Therapyherdin2008100% (1)
- Experiencing Postsocialist CapitalismDocument251 pagesExperiencing Postsocialist CapitalismjelisNo ratings yet
- Presentation - Pragati MaidanDocument22 pagesPresentation - Pragati MaidanMohamed Anas100% (4)
- Revisit of Harriott's Method For Process ControlDocument3 pagesRevisit of Harriott's Method For Process ControlkiddhoNo ratings yet
- Comparative Investment ReportDocument8 pagesComparative Investment ReportNelby Actub MacalaguingNo ratings yet
- AfPS&CS Ch-01Document10 pagesAfPS&CS Ch-01Amelwork AlchoNo ratings yet
- Tic EbookDocument215 pagesTic EbookTaju Deen100% (1)