Download as docx, pdf, or txt
You might also like
- End - Life of Care PPT 1 MainDocument48 pagesEnd - Life of Care PPT 1 MainNancy Singh63% (16)
- Condition That Mimic Brain DeathDocument20 pagesCondition That Mimic Brain DeathTan Chuan Hsin100% (1)
- Chapter 2: Foundations of Resident Care: CommunicationDocument43 pagesChapter 2: Foundations of Resident Care: Communicationapi-227612210No ratings yet
- END OF LIFE CareDocument25 pagesEND OF LIFE Caregireeshsachin100% (1)
- Z Score CompiledDocument36 pagesZ Score CompiledKamille Anne Valdez DavidNo ratings yet
- End of Life Care Workshop ANPDocument34 pagesEnd of Life Care Workshop ANPArjumand ZargarNo ratings yet
- Presentation - 2 End of Life CareDocument32 pagesPresentation - 2 End of Life CareDaneshwari Sahu100% (1)
- Final End of Life CareDocument38 pagesFinal End of Life CareArchana Panika100% (4)
- RLE 9 Post Mortem Care and DischargingDocument18 pagesRLE 9 Post Mortem Care and Dischargingryuichie100% (2)
- Loss & GrievingDocument7 pagesLoss & GrievingAmmar BhattiNo ratings yet
- Palliative Care and Post-Mortem Care: Report By: MECA M. GALIGADocument35 pagesPalliative Care and Post-Mortem Care: Report By: MECA M. GALIGAMeca GaligaNo ratings yet
- Concept of Loss, Grieving Death & DyingDocument33 pagesConcept of Loss, Grieving Death & DyingAbdullah Bhatti100% (1)
- The Dying Process Death Is Defined AsDocument5 pagesThe Dying Process Death Is Defined AsKenn yahweexNo ratings yet
- End of Life CareDocument12 pagesEnd of Life CarePATEL NEHAKUMARI VIMALBHAINo ratings yet
- Loss, Death, and Grieving - PPTX 222222-1Document37 pagesLoss, Death, and Grieving - PPTX 222222-1Muhammad Abbas Wali100% (1)
- Fundamentals of Nursing OutlineDocument4 pagesFundamentals of Nursing OutlineNina Anne ParacadNo ratings yet
- Post Mortem CareDocument14 pagesPost Mortem CareJan Oliver YaresNo ratings yet
- Thanatology: in All AspectsDocument113 pagesThanatology: in All AspectsVasantha PhutaneNo ratings yet
- End of Life Issues - EhicsDocument11 pagesEnd of Life Issues - EhicsVenu D DonNo ratings yet
- Salcedo-FUNDA LEC 15 End of LIfe CareDocument37 pagesSalcedo-FUNDA LEC 15 End of LIfe CarebaynNo ratings yet
- Palliative Care at The End of LifeDocument14 pagesPalliative Care at The End of LifeJoyce DreuNo ratings yet
- Post Mortem Care Revised PDFDocument31 pagesPost Mortem Care Revised PDFShana NikopNo ratings yet
- Care of Dying PatientDocument27 pagesCare of Dying PatientAbinaya Ranganathan100% (1)
- Hospice and Palliative Nursing: Rainier C. Moreno-Lacalle NLAC-SON Clinical InstructorDocument67 pagesHospice and Palliative Nursing: Rainier C. Moreno-Lacalle NLAC-SON Clinical InstructorRainier Moreno-LacalleNo ratings yet
- NUR 306 Palliative Care at End of LifeDocument6 pagesNUR 306 Palliative Care at End of LifeJulx0No ratings yet
- Coping With Loss, Death and GrievingDocument43 pagesCoping With Loss, Death and GrievingKishore RathoreNo ratings yet
- Govt. College of Nusing C.R.P. Line Indore (M.P.) : Subject-Advanced Nursing PracticeDocument17 pagesGovt. College of Nusing C.R.P. Line Indore (M.P.) : Subject-Advanced Nursing PracticeMamta YadavNo ratings yet
- Last Hours PDFDocument28 pagesLast Hours PDFNoshin MalekiNo ratings yet
- End of Life CareDocument19 pagesEnd of Life CareArjumand ZargarNo ratings yet
- Coping With Loss, Grieving and DeathDocument17 pagesCoping With Loss, Grieving and DeathElija Leigh MauricioNo ratings yet
- Postmortem Care Duty!!!!!!!!Document3 pagesPostmortem Care Duty!!!!!!!!Roselyn ApeladoNo ratings yet
- Care of Dying PatientDocument17 pagesCare of Dying PatientPoova RagavanNo ratings yet
- Care of Terminally IllDocument34 pagesCare of Terminally Illbemina jaNo ratings yet
- Approaching DeathDocument14 pagesApproaching DeathBhawna PandhuNo ratings yet
- Healthy-Aging ImportantDocument98 pagesHealthy-Aging Importantmasterdoctor.clinicNo ratings yet
- Progression Late Stage Alzheimer SocietyDocument6 pagesProgression Late Stage Alzheimer Societys009935No ratings yet
- Introduction To Palliative Care: by Yonas T. (BSC, MSC)Document64 pagesIntroduction To Palliative Care: by Yonas T. (BSC, MSC)Abdi Mohammed100% (1)
- Illness and Injury: Medical EmergenciesDocument23 pagesIllness and Injury: Medical EmergenciesbrentupdegraffNo ratings yet
- Palliative Care and End of Life CareDocument27 pagesPalliative Care and End of Life CaregodzahadesNo ratings yet
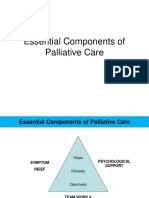
- Essential Components of Palliative CareDocument20 pagesEssential Components of Palliative CareJonah R. Merano60% (5)
- Stroke and Long-Term DisabilityDocument26 pagesStroke and Long-Term DisabilityRienaAbrahamsNo ratings yet
- Care of Terminally IllDocument34 pagesCare of Terminally Illbemina jaNo ratings yet
- DELIRIUM 21122022 114323amDocument36 pagesDELIRIUM 21122022 114323amNasreen BegumNo ratings yet
- Geriatrics: Elderly. It Aims To Promote Health and To Prevent and Treat Diseases and Disabilities in Older AdultsDocument36 pagesGeriatrics: Elderly. It Aims To Promote Health and To Prevent and Treat Diseases and Disabilities in Older Adultskhubaib InfoNo ratings yet
- About HospiceDocument6 pagesAbout HospicemonabertNo ratings yet
- Loss, Grief and DyingDocument18 pagesLoss, Grief and DyingLliryc Sotnas OleusnocNo ratings yet
- Shock and FaintingDocument31 pagesShock and Faintingafuaserwaa489No ratings yet
- Aspects of DyingDocument8 pagesAspects of Dyingnicole hope luzaNo ratings yet
- End of Life CareDocument21 pagesEnd of Life CareVandana BhasinNo ratings yet
- Gerontological PrelimDocument126 pagesGerontological PrelimAyessa Yvonne PanganibanNo ratings yet
- Ethics in Ped CCM (PICUCOURSE)Document42 pagesEthics in Ped CCM (PICUCOURSE)surasuarezlopezNo ratings yet
- Concepts of First AidDocument102 pagesConcepts of First AidDafchen Nio MahasolNo ratings yet
- Geriatric Functional Assessment: The Geriatric Review of SystemsDocument35 pagesGeriatric Functional Assessment: The Geriatric Review of SystemsNunu MirNo ratings yet
- End of Life CareDocument12 pagesEnd of Life CaregerajassoNo ratings yet
- CHP 43 QuizletDocument3 pagesCHP 43 QuizletJacqueline GreerNo ratings yet
- End-of-Life Care For The Newly Licensed Practical Nurse: State of Nebraska Transition GrantDocument8 pagesEnd-of-Life Care For The Newly Licensed Practical Nurse: State of Nebraska Transition GrantGee YorkNo ratings yet
- Elderly, Death DyingDocument74 pagesElderly, Death DyingAmy100% (1)
- Legal Aspects N Ethical Problems in EmergencyDocument121 pagesLegal Aspects N Ethical Problems in EmergencyElizeus HaninditoNo ratings yet
- Geriatric Care: James Valley Vocational Technical CenterDocument64 pagesGeriatric Care: James Valley Vocational Technical CenterMaibe JoseNo ratings yet
- Hypothermia, A Simple Guide To The Condition, Treatment And Related ConditionsFrom EverandHypothermia, A Simple Guide To The Condition, Treatment And Related ConditionsNo ratings yet
- Important Information:: Ingersoll-Rand Winch or Hoist. The Manual Form Numbers Are As FollowsDocument45 pagesImportant Information:: Ingersoll-Rand Winch or Hoist. The Manual Form Numbers Are As FollowsfreddNo ratings yet
- SEJARAH DAN PERKEMBANGAN ILMU BEDAH September 2017Document18 pagesSEJARAH DAN PERKEMBANGAN ILMU BEDAH September 2017Dipo Mas Suyudi100% (2)
- Banning Eid Homecoming By: AccangDocument1 pageBanning Eid Homecoming By: AccangRezkianiNo ratings yet
- BPK 180W - Office Ergonomics Evaluation - FinalDocument46 pagesBPK 180W - Office Ergonomics Evaluation - FinalShayla ShabkhizNo ratings yet
- Project Selection-Numeric ModelsDocument39 pagesProject Selection-Numeric Modelsshrutimsawant835No ratings yet
- COMAH Guidance For The Surface Engineering Sector: Comah Major Accident Scenarios and Risk ReductionDocument15 pagesCOMAH Guidance For The Surface Engineering Sector: Comah Major Accident Scenarios and Risk ReductionHaroon RasheedNo ratings yet
- Sodium Hypochlorite 6 % MSDSDocument5 pagesSodium Hypochlorite 6 % MSDScataztropherNo ratings yet
- Chapter 2 Review of LiteratureDocument13 pagesChapter 2 Review of LiteratureReeya PatelNo ratings yet
- Reply Third Engineer Eduardo SalasDocument19 pagesReply Third Engineer Eduardo SalasHaroldRamosNo ratings yet
- Passage - 1 I. Read The Passage Given BelowDocument17 pagesPassage - 1 I. Read The Passage Given BelowAngad SinghNo ratings yet
- Script MMHRDCDocument4 pagesScript MMHRDCrodolfo opidoNo ratings yet
- Stressors, Affectivity, and Self - Efficacy As Predictors of Librarians' Thriving at WorkDocument12 pagesStressors, Affectivity, and Self - Efficacy As Predictors of Librarians' Thriving at WorkIOER International Multidisciplinary Research Journal ( IIMRJ)No ratings yet
- Labu Farmasi Februari 2021 PDFDocument15 pagesLabu Farmasi Februari 2021 PDFWulantikaNo ratings yet
- Reaction Paper On Mental HealthDocument2 pagesReaction Paper On Mental HealthMary Louise Vapor Uyvico100% (1)
- Practical Neurosidom Elizaga 6yymbDocument22 pagesPractical Neurosidom Elizaga 6yymbAlina AbinetNo ratings yet
- Pharmacy: Pharmacist Intervention Program at Different Rent Levels of Geriatric HealthcareDocument8 pagesPharmacy: Pharmacist Intervention Program at Different Rent Levels of Geriatric HealthcareAstiNo ratings yet
- Disability, Health and DifferenceDocument20 pagesDisability, Health and DifferenceYerko CubillosNo ratings yet
- Corporate Behavioural Skills - Soft Skills - TrainingDocument7 pagesCorporate Behavioural Skills - Soft Skills - Trainingvikubhardwaj9224No ratings yet
- HIV Psychiatry - A Practical Guide PDFDocument591 pagesHIV Psychiatry - A Practical Guide PDFdanielson1986No ratings yet
- Beeps, Buzzers and Alarms: The Hemodialysis MachineDocument50 pagesBeeps, Buzzers and Alarms: The Hemodialysis MachineAndreea StreuleaNo ratings yet
- Phil Carriers v. NLRCDocument8 pagesPhil Carriers v. NLRCJohn BernalNo ratings yet
- Credentialing Pathways For Aesthetic Medicine Practice in Pakistan 13th JUNE 2022Document14 pagesCredentialing Pathways For Aesthetic Medicine Practice in Pakistan 13th JUNE 2022tasawwur zahoorNo ratings yet
- Workplace Safety ProcedureDocument12 pagesWorkplace Safety ProcedureLindsay CandolitaNo ratings yet
- Nursing Diagnosis: Impaired Physical Mobility Assessment Planning Intervention Rationale EvaluationDocument3 pagesNursing Diagnosis: Impaired Physical Mobility Assessment Planning Intervention Rationale EvaluationSheril Sularte CasanesNo ratings yet
- Miracle of Life QuestionsDocument4 pagesMiracle of Life QuestionsS. Spencer80% (5)
- Unit #7 - Basic Quality Control For The Clinical LaboratoryDocument28 pagesUnit #7 - Basic Quality Control For The Clinical LaboratoryFaisal JamshedNo ratings yet
- Gender Based ViolenceDocument12 pagesGender Based Violenceethelteng.80No ratings yet
- 20230321-Sdb-Grameen America-WestDocument23 pages20230321-Sdb-Grameen America-WestBassel HassanNo ratings yet
- Questions and Answers A Guide To Fitness and Wellness 3Rd Edition Liguori Test Bank Full Chapter PDFDocument48 pagesQuestions and Answers A Guide To Fitness and Wellness 3Rd Edition Liguori Test Bank Full Chapter PDFmathewsandersa13j100% (9)