Download as pdf or txt
You might also like
- Electronic Patient Report FormDocument6 pagesElectronic Patient Report FormDS Systems0% (1)
- Nurse - Resignation LetterDocument1 pageNurse - Resignation LetterphoenixdashNo ratings yet
- Post Mortem Care ProcedureDocument3 pagesPost Mortem Care ProcedureCarmel Bianca Delatore Bayno86% (14)
- ORS Patient PortalDocument1 pageORS Patient PortalEr Akshat Jain100% (1)
- VedantaDocument3 pagesVedantaSomesh Siddharth100% (1)
- 40.causation & Remoteness of Damage Revision AidDocument5 pages40.causation & Remoteness of Damage Revision AidAik AwaazNo ratings yet
- 004 Chapter Four Trade 2Document27 pages004 Chapter Four Trade 2OKWARO JONE BROOKS ARUNGANo ratings yet
- Negligence OutlineDocument10 pagesNegligence OutlinejohnNo ratings yet
- S1 - Introduction Aims FunctionsDocument4 pagesS1 - Introduction Aims Functionsyahya2001ysNo ratings yet
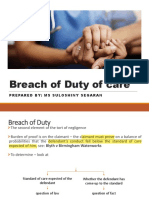
- Breach of Duty of CareDocument46 pagesBreach of Duty of CareJavier LimNo ratings yet
- 41.economic Loss Revision AidDocument5 pages41.economic Loss Revision AidAik AwaazNo ratings yet
- Breach of DutyDocument9 pagesBreach of Dutyodahkasim100% (1)
- Medical Negligence HandoutDocument3 pagesMedical Negligence Handoutcriskot21No ratings yet
- Final Exam Notes Duty 1Document14 pagesFinal Exam Notes Duty 1Ashleigh Ah Chee100% (1)
- English Law For The Surgeon III: Loss of Chance:: Gregg V Scott RevisitedDocument5 pagesEnglish Law For The Surgeon III: Loss of Chance:: Gregg V Scott RevisitedZuzana Val-VikarskáNo ratings yet
- Torts Week1Document10 pagesTorts Week1PoojakisholiNo ratings yet
- Negligence-Breach of Duty-Cont.Document31 pagesNegligence-Breach of Duty-Cont.najah hani saziliNo ratings yet
- Torts Cases BriefsDocument60 pagesTorts Cases Briefssungyeonh1234100% (1)
- Module 5 NegligenceDocument7 pagesModule 5 NegligencePalak ShethNo ratings yet
- Case CompilationDocument7 pagesCase CompilationRitesh RajNo ratings yet
- The Tort of NegligenceDocument11 pagesThe Tort of NegligenceTania C GamageNo ratings yet
- Law of NegligenceDocument16 pagesLaw of NegligenceSufyan SallehNo ratings yet
- Lecture 8 - Prof LiabilityDocument13 pagesLecture 8 - Prof LiabilityMuhammad AzRiNo ratings yet
- Torts BriefsDocument14 pagesTorts BriefsDamonde DickersonNo ratings yet
- Breach of DutyDocument2 pagesBreach of Dutyq9z9bkn5wzNo ratings yet
- Medical Negligence SampleDocument7 pagesMedical Negligence SampleRajesh ToolseeNo ratings yet
- Negligence-TORTS NOTESDocument50 pagesNegligence-TORTS NOTESMusa MomohNo ratings yet
- ArticleDocument8 pagesArticleFathima Zainab MarkarNo ratings yet
- 3-Standard and BreachDocument4 pages3-Standard and BreachABDOULIENo ratings yet
- School Moot Case Summaries 2015Document15 pagesSchool Moot Case Summaries 2015miichaeelNo ratings yet
- Tort - 17-01-2020 Paris V Stepney Borough CouncilDocument11 pagesTort - 17-01-2020 Paris V Stepney Borough CouncilSultan MughalNo ratings yet
- 12 Professional + Clinical NegligenceDocument8 pages12 Professional + Clinical NegligencenarcoticamishraNo ratings yet
- 6..Negligence-Part IIDocument14 pages6..Negligence-Part IITee Khai ChenNo ratings yet
- Negligence Per Se in Medical NegligenceDocument4 pagesNegligence Per Se in Medical NegligenceattyrichiereyNo ratings yet
- Negligence in A Nutshell - PDF Version 1Document53 pagesNegligence in A Nutshell - PDF Version 1Tasnim TabassumNo ratings yet
- NegligenceDocument9 pagesNegligencesheriyfNo ratings yet
- Tort CW 3Document3 pagesTort CW 3tracyharono18No ratings yet
- Breach of DutyDocument4 pagesBreach of DutyLady Bernadette PayumoNo ratings yet
- Negligence Part IIDocument22 pagesNegligence Part IIritha57No ratings yet
- Tort Revision SheetsDocument11 pagesTort Revision SheetsSab SameemNo ratings yet
- Case Summaries TortsDocument8 pagesCase Summaries Tortssiwasna deoNo ratings yet
- From Bolam To Bolitho Unravelling Medical ProtectionismDocument12 pagesFrom Bolam To Bolitho Unravelling Medical ProtectionismNatasha SieNo ratings yet
- 11 NegligenceDocument11 pages11 Negligencenatsu lolNo ratings yet
- 11 NegligenceDocument11 pages11 Negligencenatsu lolNo ratings yet
- 11 NegligenceDocument11 pages11 Negligencenatsu lolNo ratings yet
- 11 NegligenceDocument11 pages11 Negligencenatsu lolNo ratings yet
- Negligence ChecklistDocument5 pagesNegligence ChecklistFifi Jarrett100% (1)
- Causation: Barnett V Chelsea & Kensington Hospital Management Committee (1969) 1 QB 428Document13 pagesCausation: Barnett V Chelsea & Kensington Hospital Management Committee (1969) 1 QB 428Brandon CopemanNo ratings yet
- Lecture 6 (LSL) TortDocument4 pagesLecture 6 (LSL) TortOsamah BakhshNo ratings yet
- Causation IDocument5 pagesCausation INabil Ahmed KhanNo ratings yet
- Negligence 1 FinalDocument7 pagesNegligence 1 FinalSafa ShujaNo ratings yet
- MootDocument3 pagesMootPatrycja EppelléNo ratings yet
- Worksheet 3 - Negligence - Breach of DutyDocument13 pagesWorksheet 3 - Negligence - Breach of DutyBrian PetersNo ratings yet
- Obligation Married Couple Loan Bank Agreement Bankrupt CreditorDocument5 pagesObligation Married Couple Loan Bank Agreement Bankrupt Creditorjmac_411_409786403No ratings yet
- Tort of Simple Negligence (NEGLIGENCE)Document8 pagesTort of Simple Negligence (NEGLIGENCE)cs4rsrtnksNo ratings yet
- Critically Analyse The Criteria Used by The Courts in Determining Whether There Has Been A Breach of A Duty of Care Under The Law of TortDocument13 pagesCritically Analyse The Criteria Used by The Courts in Determining Whether There Has Been A Breach of A Duty of Care Under The Law of TortAbdul-Baki AbdulaiNo ratings yet
- Liability Duty of Care Neighbour CaparoDocument10 pagesLiability Duty of Care Neighbour CaparoReady GoNo ratings yet
- Bits of Law: Duty of Care: LiabilityDocument10 pagesBits of Law: Duty of Care: LiabilityReady GoNo ratings yet
- Good Medical Practice: September 2018Document49 pagesGood Medical Practice: September 2018gabrielNo ratings yet
- Negligence - DoC NotesDocument9 pagesNegligence - DoC NotesprincessdlNo ratings yet
- Law School Torts Outline - University of Denver Spring 2012Document12 pagesLaw School Torts Outline - University of Denver Spring 2012cmm1221100% (1)
- 41.psychiatric Injury Answer OutlineDocument8 pages41.psychiatric Injury Answer OutlineAik AwaazNo ratings yet
- Negligence: As A TortDocument40 pagesNegligence: As A TortVastavNo ratings yet
- CASES For Delict - TEST 1Document7 pagesCASES For Delict - TEST 1Asanda MlamboNo ratings yet
- English Language 10th GradeDocument19 pagesEnglish Language 10th GradeAik AwaazNo ratings yet
- English Language Trial LessonDocument28 pagesEnglish Language Trial LessonAik AwaazNo ratings yet
- 41.psychiatric Injury Answer OutlineDocument8 pages41.psychiatric Injury Answer OutlineAik AwaazNo ratings yet
- 41.economic Loss Answer OutlineDocument6 pages41.economic Loss Answer OutlineAik AwaazNo ratings yet
- 11) Roe DeerDocument4 pages11) Roe DeerAik AwaazNo ratings yet
- 9) The Harvest MoonDocument3 pages9) The Harvest MoonAik AwaazNo ratings yet
- 12) A MemoryDocument4 pages12) A MemoryAik Awaaz100% (1)
- 13) Telegraph WiresDocument3 pages13) Telegraph WiresAik Awaaz0% (1)
- 10) Football at SlackDocument4 pages10) Football at SlackAik Awaaz100% (1)
- 4) WindDocument3 pages4) WindAik AwaazNo ratings yet
- CBAHI Accredited Hospitals Full ListDocument1 pageCBAHI Accredited Hospitals Full ListRashed AlibrahemNo ratings yet
- Tarporley Talk Feb 2013Document84 pagesTarporley Talk Feb 2013Talkabout PublishingNo ratings yet
- List of Expository Essay TopicsDocument4 pagesList of Expository Essay Topicsafibojmbjifexj100% (2)
- 2022 10 27 Batch Post Intern Vacancy List Pending For ObservationsDocument44 pages2022 10 27 Batch Post Intern Vacancy List Pending For ObservationsChamindra100% (1)
- Massachusetts General HospitalDocument4 pagesMassachusetts General Hospitalí•Ꮇᴀͷ ᏚчᴀᴢᏊᴀиNo ratings yet
- 2022 EMST Course ScheduleDocument1 page2022 EMST Course ScheduleAJ JeyakumarNo ratings yet
- HKIE Ebook 202207Document66 pagesHKIE Ebook 202207Raymond LamNo ratings yet
- Tito IRBRPDocument13 pagesTito IRBRPTito TiehiNo ratings yet
- Business Proposal For Sathya Sai HospitalDocument3 pagesBusiness Proposal For Sathya Sai HospitalTriveni ChopraNo ratings yet
- History of Air Ambulance and MedevacDocument4 pagesHistory of Air Ambulance and Medevacapi-267200582No ratings yet
- Case Study D6 PDFDocument11 pagesCase Study D6 PDFAmr El SokkaryNo ratings yet
- Horn International University College: Colleege of Health ScienceDocument27 pagesHorn International University College: Colleege of Health Sciencekaise AbdiNo ratings yet
- ApprovedSchools 2023Document28 pagesApprovedSchools 2023mosesgodspower666No ratings yet
- Private EDocument205 pagesPrivate Ejayesh nitoreNo ratings yet
- ResumeDocument2 pagesResumeapi-503876999No ratings yet
- Form Must Be Returned Within 15 Days. Parts 1-3 Must Be Completed For The Application To Be ApprovedDocument1 pageForm Must Be Returned Within 15 Days. Parts 1-3 Must Be Completed For The Application To Be ApprovedKenneth SandersNo ratings yet
- Mental Health Services, Patient Pathway 2020Document18 pagesMental Health Services, Patient Pathway 2020Regina PunNo ratings yet
- Adamjee In-Patient Claim Reimbursement FormDocument2 pagesAdamjee In-Patient Claim Reimbursement Formhashamqazi100% (1)
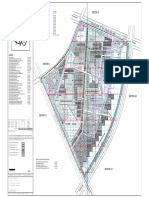
- Sector 7 Jhajjar Sector PlanDocument1 pageSector 7 Jhajjar Sector PlanRohit KoriNo ratings yet
- Home Nursing, Health Care, and Elderly Care Services in IndiaDocument11 pagesHome Nursing, Health Care, and Elderly Care Services in IndiaHome Nursing IndiaNo ratings yet
- West Midlands Acute Oncology, Directory of Services.: MSCC, AO and CUP Expert Advisory GroupDocument17 pagesWest Midlands Acute Oncology, Directory of Services.: MSCC, AO and CUP Expert Advisory GroupfidhaNo ratings yet
- Rozzano Locsin:: Technological Competence As Caring in NursingDocument22 pagesRozzano Locsin:: Technological Competence As Caring in NursingJeng100% (1)
- POC CHWO HW Solutions PDFDocument5 pagesPOC CHWO HW Solutions PDFakashkr619No ratings yet
- Ana Liezl Mendoza Illescas1 1 1 1Document3 pagesAna Liezl Mendoza Illescas1 1 1 1Prinze SereguineNo ratings yet
- Unapplied and Unidentified Receipts DetailDocument24 pagesUnapplied and Unidentified Receipts DetailMariano ManuNo ratings yet