Download as pdf or txt
You might also like
- The Relay Testing Handbook-Generator Relay Protection Testing TOC-ToF-BibDocument36 pagesThe Relay Testing Handbook-Generator Relay Protection Testing TOC-ToF-BibMartin Goodnough100% (1)
- Acute Kidney Injury - Seminar Lancet 2019Document16 pagesAcute Kidney Injury - Seminar Lancet 2019Giliana P. García AcevedoNo ratings yet
- Chippewa Park Master Plan ReportDocument28 pagesChippewa Park Master Plan ReportinforumdocsNo ratings yet
- Investment Project Management SampleDocument9 pagesInvestment Project Management SampleShaneel PrasadNo ratings yet
- NDT - Sepsis-Associated Acute Kidney Injury Treatment StandardDocument10 pagesNDT - Sepsis-Associated Acute Kidney Injury Treatment Standardsebah.feitosaNo ratings yet
- HHS Public Access: Sepsis-Induced AKI Revisited: Pathophysiology, Prevention and Future TherapiesDocument13 pagesHHS Public Access: Sepsis-Induced AKI Revisited: Pathophysiology, Prevention and Future TherapiesromiNo ratings yet
- AKI PathogenesisDocument11 pagesAKI PathogenesisKaren RamNo ratings yet
- Acute Kidney Injury1Document16 pagesAcute Kidney Injury1Hmn07No ratings yet
- Potential Interventions in Sepsis-Related Acute Kidney InjuryDocument14 pagesPotential Interventions in Sepsis-Related Acute Kidney InjurynudhakoNo ratings yet
- Personalized Acute Kidney Injury TreatmentDocument8 pagesPersonalized Acute Kidney Injury TreatmentGabriela PachecoNo ratings yet
- Acute Kidney Injury From Sepsis Current ConceptsDocument33 pagesAcute Kidney Injury From Sepsis Current ConceptsUntuk DownloadNo ratings yet
- Subphenotypes of Acute Kidney Injury 2022Document6 pagesSubphenotypes of Acute Kidney Injury 2022Juan Diego JImenez AlvizoNo ratings yet
- Acute Kidney Injury 2019Document16 pagesAcute Kidney Injury 2019ShadowK 99No ratings yet
- Diagnosis and Treatment of Acute Kidney Injury in PediatricsDocument13 pagesDiagnosis and Treatment of Acute Kidney Injury in PediatricsagungNo ratings yet
- Acute Kidney Injury: Current Concepts and New Insights: Key WordsDocument5 pagesAcute Kidney Injury: Current Concepts and New Insights: Key WordsIHNo ratings yet
- Prerenalacutekidneyinjury 2020Document9 pagesPrerenalacutekidneyinjury 2020diana ramirezNo ratings yet
- 10 1097@MCC 0000000000000356Document8 pages10 1097@MCC 0000000000000356Elena StepanNo ratings yet
- Jurnal 2Document6 pagesJurnal 2tataNo ratings yet
- Sepsis and Acute Kidney Injury.7Document8 pagesSepsis and Acute Kidney Injury.7ansylaeNo ratings yet
- Critical Care Nephrology Core Curriculum 2019Document34 pagesCritical Care Nephrology Core Curriculum 2019Edmilson R. LimaNo ratings yet
- Acute Kidney InjuryDocument16 pagesAcute Kidney InjuryAdo QuirozNo ratings yet
- Paper 2Document15 pagesPaper 2constanzanazarethNo ratings yet
- Periop AKIDocument12 pagesPeriop AKINavjot KaurNo ratings yet
- Study of Etiology, Clinical Profile and Outcome of Acute Kidney (AKI) in Medical Intensive Care UnitDocument4 pagesStudy of Etiology, Clinical Profile and Outcome of Acute Kidney (AKI) in Medical Intensive Care UnitDavid Al HavizNo ratings yet
- Nihms 300455Document22 pagesNihms 300455Maria Eduarda CardosoNo ratings yet
- Acute Kidney Injury From Sepsis: Current Concepts, Epidemiology, Pathophysiology, Prevention and TreatmentDocument17 pagesAcute Kidney Injury From Sepsis: Current Concepts, Epidemiology, Pathophysiology, Prevention and TreatmentValentina MartinezNo ratings yet
- Epidemio AkiDocument10 pagesEpidemio AkiSoniamartilovaNo ratings yet
- Acute Kidney Injury Lancet RoncoDocument16 pagesAcute Kidney Injury Lancet RoncoRogelio MarchanNo ratings yet
- AKI Perioperatif 2Document12 pagesAKI Perioperatif 2Kevin JohanesNo ratings yet
- The Japanese Clinical Practice Guideline For Acute Kidney Injury 2016Document55 pagesThe Japanese Clinical Practice Guideline For Acute Kidney Injury 2016RobertNo ratings yet
- Sepsis en IRADocument16 pagesSepsis en IRAKev Jose Ruiz RojasNo ratings yet
- Sepsis-Associated Acute Kidney Injury: Consensus Report of The 28th Acute Disease Quality Initiative WorkgroupDocument17 pagesSepsis-Associated Acute Kidney Injury: Consensus Report of The 28th Acute Disease Quality Initiative WorkgroupDaniel AmezcuaNo ratings yet
- Oxidative Stress in AKIDocument21 pagesOxidative Stress in AKIRania T. SabriNo ratings yet
- Study of Clinical Profile of Patient With Acute Kidney DiseaseDocument7 pagesStudy of Clinical Profile of Patient With Acute Kidney DiseaseIJAR JOURNALNo ratings yet
- Arifin 2018 IOP Conf. Ser. Earth Environ. Sci. 125 012085Document6 pagesArifin 2018 IOP Conf. Ser. Earth Environ. Sci. 125 012085محمود صابرNo ratings yet
- JPC c0502005Document7 pagesJPC c0502005Sabelo ZeeNo ratings yet
- Ajm S 23 01275Document28 pagesAjm S 23 01275Noreen PunjwaniNo ratings yet
- Update of Sepsis in The Intensive Care Unit: Innate ImmunityDocument15 pagesUpdate of Sepsis in The Intensive Care Unit: Innate ImmunityAmirullah AbdiNo ratings yet
- Renal Hemodynamic Evaluation Protocol Based On The PathophysiologicalDocument13 pagesRenal Hemodynamic Evaluation Protocol Based On The Pathophysiologicalmiguel aghelNo ratings yet
- Sepsis For The Anaesthetist: M. E. NunnallyDocument8 pagesSepsis For The Anaesthetist: M. E. NunnallySucii Sekar NingrumNo ratings yet
- AKI7Document14 pagesAKI7Kholida NabilaNo ratings yet
- JournalDocument17 pagesJournaljust for download matterNo ratings yet
- Aki To CKDDocument22 pagesAki To CKDSrinivas PingaliNo ratings yet
- Best Practice & Research Clinical AnaesthesiologyDocument10 pagesBest Practice & Research Clinical AnaesthesiologyAdam JohnsonNo ratings yet
- Role of Kidney Injury in Sepsis: Review Open AccessDocument6 pagesRole of Kidney Injury in Sepsis: Review Open AccessnudhakoNo ratings yet
- Ben-Haim Et Al. 2022 - Forced Diuresis With Matched Isotonic Intravenous Hydration Prevents Renal Contrast Media Accumulation PDFDocument10 pagesBen-Haim Et Al. 2022 - Forced Diuresis With Matched Isotonic Intravenous Hydration Prevents Renal Contrast Media Accumulation PDFadm kdmyNo ratings yet
- The Rationale For Extracorporeal Therapies in SepsisDocument9 pagesThe Rationale For Extracorporeal Therapies in SepsisLoudry ElfaNo ratings yet
- Dengue Associated Acute Kidney Infection...Document9 pagesDengue Associated Acute Kidney Infection...Mono KoromoNo ratings yet
- Management of Acute Kidney Injury in Sepsis KirimDocument5 pagesManagement of Acute Kidney Injury in Sepsis KirimRicky ImranNo ratings yet
- Definitions, Epidemiology and PathophysiologyDocument8 pagesDefinitions, Epidemiology and PathophysiologyFanny Ari SandyNo ratings yet
- WJH 13 533Document11 pagesWJH 13 533CIRUGÍA ONCOLÓGICA ABDOMENNo ratings yet
- 2015 Anaesthesiology Intensive Therapy ManagementofabdomminalsepsisaparadigmshiftDocument10 pages2015 Anaesthesiology Intensive Therapy ManagementofabdomminalsepsisaparadigmshiftdwimellyndaNo ratings yet
- HHS Public Access: The Role of Acute Kidney Injury in Chronic Kidney DiseaseDocument18 pagesHHS Public Access: The Role of Acute Kidney Injury in Chronic Kidney DiseaseAndi NunuNo ratings yet
- Global Epidemiology and Outcomes of Acute Kidney InjuryDocument19 pagesGlobal Epidemiology and Outcomes of Acute Kidney Injuryredouane bennaiNo ratings yet
- Critical Care Nephrology Core Curriculum 2020 PDFDocument18 pagesCritical Care Nephrology Core Curriculum 2020 PDFMartín FleiNo ratings yet
- 16 PDFDocument8 pages16 PDFAkhileshNo ratings yet
- Acute Kidney Injury Pathology and PathophysiologyDocument11 pagesAcute Kidney Injury Pathology and Pathophysiologyhossein kasiriNo ratings yet
- Low-Flow Acute Kidney InjuryDocument11 pagesLow-Flow Acute Kidney InjuryJuan Manuel Lopez VargasNo ratings yet
- Acute KidneyDocument4 pagesAcute KidneyEliDavidNo ratings yet
- Tubuus ProximalDocument24 pagesTubuus ProximalJundiNo ratings yet
- The Evolving Landscape of Liver Cirrhosis ManagementFrom EverandThe Evolving Landscape of Liver Cirrhosis ManagementHitoshi YoshijiNo ratings yet
- Comprehensive Perspectives in Abdominal Compartment Syndrome: Understanding, Management, and Future DirectionsFrom EverandComprehensive Perspectives in Abdominal Compartment Syndrome: Understanding, Management, and Future DirectionsNo ratings yet
- Recent Advances of Sarcopenia and Frailty in CKDFrom EverandRecent Advances of Sarcopenia and Frailty in CKDAkihiko KatoNo ratings yet
- Synopsis Four PawsDocument7 pagesSynopsis Four PawsAnmol DubeyNo ratings yet
- L-s20 Specification For Road Lighting InstallationDocument82 pagesL-s20 Specification For Road Lighting Installationzamanhuri junidNo ratings yet
- Twinkle For Heather Challenge V2Document63 pagesTwinkle For Heather Challenge V2gillian.cartwrightNo ratings yet
- Training Report of IoclDocument68 pagesTraining Report of IoclAnupam SrivastavNo ratings yet
- Dwaraka Nadh K: Mobile:8504080654,8500353334Document3 pagesDwaraka Nadh K: Mobile:8504080654,8500353334anon_396084846No ratings yet
- Dampak Bencana Alam Bagi Sektor Pariwisata Di Bali Ni Ketut Sutrisnawati AKPAR DenpasarDocument10 pagesDampak Bencana Alam Bagi Sektor Pariwisata Di Bali Ni Ketut Sutrisnawati AKPAR DenpasarRihar KoharNo ratings yet
- ISO 00426-1-1983 ScanDocument5 pagesISO 00426-1-1983 ScanthangNo ratings yet
- 3D Marine Seismic Survey Design PDFDocument129 pages3D Marine Seismic Survey Design PDFgeophenryNo ratings yet
- 2015 - Soil Mechanics II - Final - enDocument7 pages2015 - Soil Mechanics II - Final - enjohn cambixNo ratings yet
- pBrain-HexEngine Configuration Guide v1.2Document35 pagespBrain-HexEngine Configuration Guide v1.2lazer155No ratings yet
- Me 335 Exp 2Document8 pagesMe 335 Exp 2Brian AliasgharNo ratings yet
- NavAid Module 2.0Document21 pagesNavAid Module 2.0Kiel HerreraNo ratings yet
- Daftar Singkatan SMF JAntungDocument5 pagesDaftar Singkatan SMF JAntungBobby RahmantoNo ratings yet
- BFB2 PDFDocument4 pagesBFB2 PDFQuang HuyNo ratings yet
- Assign 01 (8610) Wajahat Ali Ghulam BU607455 B.ed 1.5 YearsDocument9 pagesAssign 01 (8610) Wajahat Ali Ghulam BU607455 B.ed 1.5 YearsAima Kha KhanNo ratings yet
- Digestibility Evaluation of Fish Meal, Rice Bran, Soya Bean Meal, Pollard On Ongole Cross Breed Cattle and Frisien Holstein Cross BreedDocument7 pagesDigestibility Evaluation of Fish Meal, Rice Bran, Soya Bean Meal, Pollard On Ongole Cross Breed Cattle and Frisien Holstein Cross BreedFailal Ulfi MauliahNo ratings yet
- Meter Box Covers and Lids - EJDocument32 pagesMeter Box Covers and Lids - EJironworkNo ratings yet
- The Summer Internship at Limited: Hindustan AeronauticsDocument59 pagesThe Summer Internship at Limited: Hindustan AeronauticsAbhishek StarkNo ratings yet
- Capacity PlanDocument1 pageCapacity PlanbishnuNo ratings yet
- Task 2 Overview and Instructions 2021Document3 pagesTask 2 Overview and Instructions 2021alindafitrotNo ratings yet
- XT0223S16128 Smart调试说明书 ENDocument81 pagesXT0223S16128 Smart调试说明书 ENBagwis100% (1)
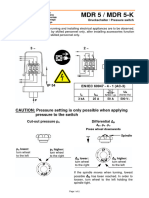
- Pressure Switch MDR5Document4 pagesPressure Switch MDR5Fidelis NdanoNo ratings yet
- Pronoun Reference - Exercise 5: Correction Should Sound Natural and Be LogicalDocument4 pagesPronoun Reference - Exercise 5: Correction Should Sound Natural and Be LogicalPreecha ChanlaNo ratings yet
- Class VI Science Chap - 3 TP Solution (Date 19-07-2019)Document3 pagesClass VI Science Chap - 3 TP Solution (Date 19-07-2019)Gopal ShuklaNo ratings yet
- Dopamine D23 Receptor Antagonism Reduces Activity-Based AnorexiaDocument10 pagesDopamine D23 Receptor Antagonism Reduces Activity-Based AnorexiaJeffery TaylorNo ratings yet
- Mobile Division: Service Parts ListDocument20 pagesMobile Division: Service Parts Listwag008No ratings yet
- Helicopter SafetyDocument11 pagesHelicopter SafetyWilliam Greco100% (2)