Download as pdf or txt
You might also like
- Hypothyroidism Type 2 - The Epid - Mark Starr MD-lin PDFDocument280 pagesHypothyroidism Type 2 - The Epid - Mark Starr MD-lin PDFLi Lin100% (4)
- The Adrenal Reset Diet by Alan Christianson, NMD - ExcerptDocument39 pagesThe Adrenal Reset Diet by Alan Christianson, NMD - ExcerptCrown Publishing Group56% (9)
- Disorders of The Thyroid Gland Harrison's Principles of Internal Medicine, 19eDocument21 pagesDisorders of The Thyroid Gland Harrison's Principles of Internal Medicine, 19ePeterNo ratings yet
- Thyroid GlandDocument49 pagesThyroid Glandjuliefe pinionNo ratings yet
- Laboratory Diagnostics of (Selected) Endocrine DisordersDocument48 pagesLaboratory Diagnostics of (Selected) Endocrine DisordersPaulina PaskeviciuteNo ratings yet
- Hypothyroid in Pregnancy Andi CakraDocument32 pagesHypothyroid in Pregnancy Andi CakraCakraEkky100% (1)
- Therapeutics: Thyroid DisordersDocument24 pagesTherapeutics: Thyroid DisordersSharas FarhadNo ratings yet
- Thyroid DisordersDocument55 pagesThyroid DisordersNsubuga Ivan100% (1)
- Endocrine 160110083024Document65 pagesEndocrine 160110083024Ryan CracknellNo ratings yet
- Gds137 Slide HyperthyroidismDocument30 pagesGds137 Slide HyperthyroidismLouie Kem Anthony BabaranNo ratings yet
- Graves' Hyperthyroidism in Pregnancy: A Clinical ReviewDocument22 pagesGraves' Hyperthyroidism in Pregnancy: A Clinical ReviewAnisa Dinda NurlianaNo ratings yet
- HYPOTHYROIDISMDocument30 pagesHYPOTHYROIDISMTopeNo ratings yet
- Thyroid Disorders During PregnancyDocument25 pagesThyroid Disorders During PregnancyA.H.ANo ratings yet
- Diagnosis of HypothyroidismDocument10 pagesDiagnosis of HypothyroidismHanzla IrfanNo ratings yet
- Biol 460 Case StudyDocument11 pagesBiol 460 Case Studyapi-353888678No ratings yet
- Variations, Errors, and QualityDocument46 pagesVariations, Errors, and QualityJohn Reden RomeroNo ratings yet
- Hyperthyroidsm: EpidemiologyDocument6 pagesHyperthyroidsm: EpidemiologyEllieNo ratings yet
- Guidelines of The American Thyroid Association PREGNANCY PDFDocument47 pagesGuidelines of The American Thyroid Association PREGNANCY PDFIqra AnugerahNo ratings yet
- 1-Good Health Gold Package - PO2257496339-951Document1 page1-Good Health Gold Package - PO2257496339-951Aafaq BhuttoNo ratings yet
- Abnormal Thyroid Function in PregnancyDocument54 pagesAbnormal Thyroid Function in Pregnancyasri khazaliNo ratings yet
- Conference Brochure With Link7Document16 pagesConference Brochure With Link7Shrutik AshiyaniNo ratings yet
- Thyroid DX PXLDocument62 pagesThyroid DX PXLabduljebarNo ratings yet
- Hypothyroidism in PregnancyDocument14 pagesHypothyroidism in PregnancyShajia ZafarNo ratings yet
- Week 3 Pharmaco Part 2Document34 pagesWeek 3 Pharmaco Part 2Tiko JomidavaNo ratings yet
- FunctionTests Brochure PDFDocument2 pagesFunctionTests Brochure PDFArslan SaleemNo ratings yet
- Goiter and Malignant Thyroid DiseaseDocument24 pagesGoiter and Malignant Thyroid Diseaseshaza ewisNo ratings yet
- Thyroid Function Test (TFT'S) : Presented By: Shoaib Ahmad Usama Maqsood Kamran AnjumDocument52 pagesThyroid Function Test (TFT'S) : Presented By: Shoaib Ahmad Usama Maqsood Kamran AnjumpriyaNo ratings yet
- TPO in PregnancyDocument18 pagesTPO in PregnancyRoxana TudorNo ratings yet
- Thyroid Function Test Results: APFCB Masterclass in Interpretative CommentingDocument58 pagesThyroid Function Test Results: APFCB Masterclass in Interpretative CommentingGPNNo ratings yet
- Lab Report NewDocument2 pagesLab Report Newnsdh5v5v5sNo ratings yet
- Presentation SlideDocument63 pagesPresentation SlideJENNIFER ENEKWECHINo ratings yet
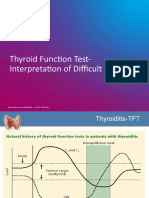
- TFT Interpretation of Difficult CasesDocument51 pagesTFT Interpretation of Difficult CasesAditya GautamNo ratings yet
- The Role of Maternal Thyroid Status On Pregnancy Outcome For Motherand NewbornDocument36 pagesThe Role of Maternal Thyroid Status On Pregnancy Outcome For Motherand NewbornRahmayantiYuliaNo ratings yet
- CHN1 Health Care Delivery System2Document22 pagesCHN1 Health Care Delivery System2MicaNo ratings yet
- HyperthyroidDocument12 pagesHyperthyroidChristine Joy PepitoNo ratings yet
- Thyroid Profile (Total T3, Total T4, TSH), Serum: EcliaDocument3 pagesThyroid Profile (Total T3, Total T4, TSH), Serum: EcliaRoopa gowdaNo ratings yet
- Pemeriksaaan Laboratorium Kelainan Thyroid: DR - Budi Dermawan Lubis, SPPK DR - Siti Hajar, M.Ked, SPPKDocument12 pagesPemeriksaaan Laboratorium Kelainan Thyroid: DR - Budi Dermawan Lubis, SPPK DR - Siti Hajar, M.Ked, SPPKBonitavanyNo ratings yet
- Deepika.R:::: Patient Age / Sex 26 Y / Female BranchDocument2 pagesDeepika.R:::: Patient Age / Sex 26 Y / Female BranchkannanNo ratings yet
- Surgical Pathology For Dentistry Students - Surgical Pathology of Thyroid and Adrenal GlandsDocument38 pagesSurgical Pathology For Dentistry Students - Surgical Pathology of Thyroid and Adrenal Glandssorin niky mocanu100% (1)
- Hypothyroidism in PregnancyDocument29 pagesHypothyroidism in PregnancyhanaddulNo ratings yet
- Dneerajalaxmi 20220611120615333Document1 pageDneerajalaxmi 20220611120615333Donthula SripathiNo ratings yet
- Clinical Practice Guidelines For Hypothyroidism in Adults: AACE and ATA 2012Document63 pagesClinical Practice Guidelines For Hypothyroidism in Adults: AACE and ATA 2012Nur Rakhma AkmaliaNo ratings yet
- Critical Aspect Analytical Test Review: Jakarta 14 December 2017 Speaker: Heru Purnomo, STDocument24 pagesCritical Aspect Analytical Test Review: Jakarta 14 December 2017 Speaker: Heru Purnomo, STMohammad Naufal AliefNo ratings yet
- Thyroid and Adrenal MedullaDocument32 pagesThyroid and Adrenal MedullaDipika RawatNo ratings yet
- Thyroid CancerDocument19 pagesThyroid CancerPowell Tabogoc100% (1)
- Thyroid and InfertilityDocument36 pagesThyroid and InfertilitySairindri SahooNo ratings yet
- Thyroid DisordersDocument34 pagesThyroid DisordersAbdulhameed Mohamed100% (1)
- Lec#17+18 Adrenal DisordersDocument101 pagesLec#17+18 Adrenal DisordersKhaldoun AlmomaniNo ratings yet
- Im Testing For Endocrine DisordersDocument7 pagesIm Testing For Endocrine DisordersChristine MendozaNo ratings yet
- THYROIDDocument100 pagesTHYROIDFrance PalNo ratings yet
- Thyroid Neoplasm: Dr. M. Abrar BarakzaiDocument38 pagesThyroid Neoplasm: Dr. M. Abrar Barakzaimohammed alrubaiaanNo ratings yet
- GOITERDocument4 pagesGOITERJerika Shane MañosoNo ratings yet
- Hyperprolactinem IaDocument63 pagesHyperprolactinem Iakhadzx100% (2)
- Thyroid Disease: Presentation By: Pimundu Vicent Audo Ritah Tutor: Dr. Fualal JaneDocument41 pagesThyroid Disease: Presentation By: Pimundu Vicent Audo Ritah Tutor: Dr. Fualal JaneEsther AumaNo ratings yet
- Thyroid Emergencies: Abrar AlharbiDocument35 pagesThyroid Emergencies: Abrar AlharbiabrarNo ratings yet
- Autoverification ImplementationDocument53 pagesAutoverification ImplementationEi JamNo ratings yet
- Sheehan SyndromeDocument6 pagesSheehan SyndromeArvie TagnongNo ratings yet
- HYPERTHYROIDISMDocument40 pagesHYPERTHYROIDISMEmmanuelNo ratings yet
- WHO MEC-wheel PDFDocument8 pagesWHO MEC-wheel PDFBillyNicolasNo ratings yet
- Endocrinology Board Review: Thyroid DisordersDocument46 pagesEndocrinology Board Review: Thyroid DisordersDemuel Dee L. BertoNo ratings yet
- What Is HypothyroidismDocument16 pagesWhat Is HypothyroidismvinhannyNo ratings yet
- Anemia in PregnancyDocument34 pagesAnemia in PregnancyHannah Halim100% (1)
- Internal Med. EndoDocument35 pagesInternal Med. EndoEdwin OkonNo ratings yet
- IM III Final Exam (2018) BatchDocument19 pagesIM III Final Exam (2018) BatchAli Murtaza AbbasNo ratings yet
- 14-Rheumatoid Arthritis 2021Document54 pages14-Rheumatoid Arthritis 2021Ali Murtaza AbbasNo ratings yet
- 1-2022 Gastric CancerDocument95 pages1-2022 Gastric CancerAli Murtaza AbbasNo ratings yet
- SecondDocument28 pagesSecondAli Murtaza AbbasNo ratings yet
- Maths Test 01Document4 pagesMaths Test 01Ali Murtaza AbbasNo ratings yet
- Physics Test 01Document6 pagesPhysics Test 01Ali Murtaza AbbasNo ratings yet
- Biology Test 01Document6 pagesBiology Test 01Ali Murtaza AbbasNo ratings yet
- Chronic Complications of Diabetes MellitusDocument53 pagesChronic Complications of Diabetes MellitusAli Murtaza AbbasNo ratings yet
- Ultrasound in Gynecology and ObstetricsDocument197 pagesUltrasound in Gynecology and ObstetricsAli Murtaza AbbasNo ratings yet
- MED1 Samplex Rationale 6 - Endocrine DisordersDocument6 pagesMED1 Samplex Rationale 6 - Endocrine DisordersMartina GarciaNo ratings yet
- Menopause Homeopathy PDFDocument14 pagesMenopause Homeopathy PDFaftabbd5765100% (1)
- Eanm Guideline Radioiodine Therapy Benign Thyroid DiseaseDocument25 pagesEanm Guideline Radioiodine Therapy Benign Thyroid Diseasechrisgiang552No ratings yet
- Laboratory Diagnostics of (Selected) Endocrine DisordersDocument48 pagesLaboratory Diagnostics of (Selected) Endocrine DisordersPaulina PaskeviciuteNo ratings yet
- Ple TipsDocument14 pagesPle TipsChristine Evan HoNo ratings yet
- Diagnostic Test For Endocrine DisordersDocument15 pagesDiagnostic Test For Endocrine DisordersRichard Deo R. Alave100% (1)
- Obstetrics MCQ: Amanda Leow AFP NHS Lothian 20 Jan 2021Document62 pagesObstetrics MCQ: Amanda Leow AFP NHS Lothian 20 Jan 2021Amanda LeowNo ratings yet
- DNB Gen Surgery Old Question Papers 1Document28 pagesDNB Gen Surgery Old Question Papers 1sidorai100% (1)
- Hypo & HyperthyroidismDocument13 pagesHypo & Hyperthyroidismgolden fleeceNo ratings yet
- Thyroid FunctionDocument12 pagesThyroid Functionسلطان القلحNo ratings yet
- Thyroid Hormones: K.Ramachandran M.Sc. Medical Biochemistry SRM Medical CollegeDocument31 pagesThyroid Hormones: K.Ramachandran M.Sc. Medical Biochemistry SRM Medical CollegeKuzhandai VeluNo ratings yet
- Thyroid Function Test and Its Interpretation: Journal of Pathology of Nepal March 2014Document8 pagesThyroid Function Test and Its Interpretation: Journal of Pathology of Nepal March 2014citraNo ratings yet
- A Critical Review of Kanchanara Guggulu A Poly Herbal FormulationDocument6 pagesA Critical Review of Kanchanara Guggulu A Poly Herbal FormulationEditor IJTSRDNo ratings yet
- Hyperthyroidism During Pregnancy: Etiology, Diagnosis and ManagementDocument9 pagesHyperthyroidism During Pregnancy: Etiology, Diagnosis and ManagementAdi PratamaNo ratings yet
- Thyroid DisorderDocument2 pagesThyroid Disordermaulikmd21No ratings yet
- Oxford Case Histories in Obstetric Medicine Charlotte Frise Full ChapterDocument67 pagesOxford Case Histories in Obstetric Medicine Charlotte Frise Full Chapterdavid.lucero121100% (7)
- ESMO Guidelines Immunotherapy Toxicities7 PDFDocument24 pagesESMO Guidelines Immunotherapy Toxicities7 PDFOscar MerinoNo ratings yet
- (1479683X - European Journal of Endocrinology) MECHANISMS IN ENDOCRINOLOGY - Autoimmune Thyroid Disease - Old and New PlayersDocument12 pages(1479683X - European Journal of Endocrinology) MECHANISMS IN ENDOCRINOLOGY - Autoimmune Thyroid Disease - Old and New PlayersIoana BodescuNo ratings yet
- Thyroid Disorders Testing AlgorithmDocument1 pageThyroid Disorders Testing AlgorithmRezi HelperNo ratings yet
- Survey For Thyroidism Patient 1111Document90 pagesSurvey For Thyroidism Patient 1111BvayNo ratings yet
- The Complete Thyroid Cookbook Easy Recipes and Meal Plans For Hypothyroidism and Hashimoto S ReliefDocument231 pagesThe Complete Thyroid Cookbook Easy Recipes and Meal Plans For Hypothyroidism and Hashimoto S Relieflunita.lmdsNo ratings yet
- A Case Study On Thyroid CystDocument83 pagesA Case Study On Thyroid CystJobeth DacupNo ratings yet
- Thyroid DisordersDocument5 pagesThyroid DisordersAnggunNMNo ratings yet
- Hyperthyroidism in PregnancyDocument21 pagesHyperthyroidism in PregnancyCharisse Aser Flores AquinoNo ratings yet
- Thyroid Function TestDocument28 pagesThyroid Function TestDhinesh Muthusamy100% (1)
- L37 - Mr. Ashish Narang - FPSC Paramount Tulip Shop No.9, Paramount Tulip, Delhi Road, SAHARANPUR, UP. C-8629994444, 8629990007Document13 pagesL37 - Mr. Ashish Narang - FPSC Paramount Tulip Shop No.9, Paramount Tulip, Delhi Road, SAHARANPUR, UP. C-8629994444, 8629990007vishal pundirNo ratings yet
- CC2 Lab 13Document10 pagesCC2 Lab 13Junea SeeNo ratings yet