
EC Epirubicin Cyclophosphamide Adjuvant Neo-Adjuvant Regimen Protocol V1.0
EC Epirubicin Cyclophosphamide Adjuvant Neo-Adjuvant Regimen Protocol V1.0
You might also like
- Etoposide Oral Sarcoma Protocol V1.0Document3 pagesEtoposide Oral Sarcoma Protocol V1.0أبو عبد الرحمن المحموديNo ratings yet
- Docetaxel Protocol V1.0Document6 pagesDocetaxel Protocol V1.0أبو عبد الرحمن المحموديNo ratings yet
- Protokol SarcomaDocument4 pagesProtokol SarcomaHep PutNo ratings yet
- Temozolomide Adjuvant NHSDocument5 pagesTemozolomide Adjuvant NHSSyed Touseef AhmedNo ratings yet
- Antimicrobial Dosage Adjustments in Renal Impairment For FormularyDocument20 pagesAntimicrobial Dosage Adjustments in Renal Impairment For Formularyangkatanjuli2019No ratings yet
- Carboplatin With Pemetrexed Pembrolizumab Non Squamous Non-Small Cell Lung Cancer Protocol V1.1Document8 pagesCarboplatin With Pemetrexed Pembrolizumab Non Squamous Non-Small Cell Lung Cancer Protocol V1.1Olaru DianaNo ratings yet
- 311 Topotecan Monotherapy 5 DayDocument4 pages311 Topotecan Monotherapy 5 DayRuxandra BănicăNo ratings yet
- Oncology Antiemetic PolicyDocument8 pagesOncology Antiemetic PolicyAnggy L, dr.No ratings yet
- Avelumab Merkel Cell Carcinoma Protocol V1.1Document6 pagesAvelumab Merkel Cell Carcinoma Protocol V1.1Vlad CroitoruNo ratings yet
- Aida Protocol For Apl: InductionDocument4 pagesAida Protocol For Apl: InductionGabrielNo ratings yet
- Heparin Dose Adjustment in The Prescence of Renal ImpairmentDocument5 pagesHeparin Dose Adjustment in The Prescence of Renal ImpairmentRPR KSVNo ratings yet
- SAAI Protocol KankerDocument4 pagesSAAI Protocol KankerSadha MahardhikaNo ratings yet
- Paclitaxel With Dose Dense EC Adjuvant or Neo-Adjuvant Protocol V1.0Document7 pagesPaclitaxel With Dose Dense EC Adjuvant or Neo-Adjuvant Protocol V1.0smokkerNo ratings yet
- CHLVPP (Hodgkin'S Lymphoma) : (Max: 10Mg) (Max: 10Mg)Document3 pagesCHLVPP (Hodgkin'S Lymphoma) : (Max: 10Mg) (Max: 10Mg)Sindu SankarNo ratings yet
- Imatinib For Philadelphia Chromosome Positive CML, First LineDocument4 pagesImatinib For Philadelphia Chromosome Positive CML, First LinehendranuraminNo ratings yet
- Neratinib Adjuvant Treatment Breast Cancer Protocol V1.1Document6 pagesNeratinib Adjuvant Treatment Breast Cancer Protocol V1.1smokkerNo ratings yet
- CVP Plus Rituximab (R-CVP) For Lymphoma: Page 1 of 2Document2 pagesCVP Plus Rituximab (R-CVP) For Lymphoma: Page 1 of 2Andreea NeculceaNo ratings yet
- EC-DH Epirubicin Cyclophosphamide Followed by Docetaxel With Trastuzumab Protocol V1.1Document11 pagesEC-DH Epirubicin Cyclophosphamide Followed by Docetaxel With Trastuzumab Protocol V1.1smokkerNo ratings yet
- Cyclophosphamide Doxorubicin Ver 1.1Document6 pagesCyclophosphamide Doxorubicin Ver 1.1Yudi ApriyantoNo ratings yet
- ASWCS10 HN001 Weekly Cisp and Radtx Final 110325 - AmendedJuly2012Document3 pagesASWCS10 HN001 Weekly Cisp and Radtx Final 110325 - AmendedJuly2012Kurnia AnharNo ratings yet
- Drug Study GentamicinDocument3 pagesDrug Study GentamicinEARL GERALD RICAFRANCANo ratings yet
- 1.13 Hyper-CVAD-MA Version 2.1Document5 pages1.13 Hyper-CVAD-MA Version 2.1Alina CrissNo ratings yet
- Paclitaxel Albumin Abraxane Breast Cancer V1.1Document7 pagesPaclitaxel Albumin Abraxane Breast Cancer V1.1smokkerNo ratings yet
- Enoxaparin - Prescribing, Administration and MonitoringDocument6 pagesEnoxaparin - Prescribing, Administration and MonitoringFaheem AlsabriaNo ratings yet
- Enoxaparin - Safe Prescribing - Check It Out 1Document3 pagesEnoxaparin - Safe Prescribing - Check It Out 1Zaid DewachiNo ratings yet
- RLE - Oncology NotesDocument2 pagesRLE - Oncology NotesmareginaNo ratings yet
- SCLC Cisplatin-Etoposide IVplusor-RT Protocol V1.1Document3 pagesSCLC Cisplatin-Etoposide IVplusor-RT Protocol V1.1vera docNo ratings yet
- Tramadol Plus ParacetamolDocument2 pagesTramadol Plus ParacetamolKeir Mrls ForcadillaNo ratings yet
- ABVDDocument3 pagesABVDEsther WanguiNo ratings yet
- Brajac - ProtocolDocument13 pagesBrajac - Protocolthanh ngôNo ratings yet
- Supportive Care During Cancer TreatmentDocument18 pagesSupportive Care During Cancer TreatmentDebs AngupaNo ratings yet
- Anticoagulation Protocol For PostDocument8 pagesAnticoagulation Protocol For PostMohammed IbrahimNo ratings yet
- Mitomycin - UsmanDocument3 pagesMitomycin - UsmanSittie Nashieva A. UsmanNo ratings yet
- Oncology Supportive CareDocument57 pagesOncology Supportive CaredewiNo ratings yet
- Case Study ThrombocytopeniaDocument8 pagesCase Study ThrombocytopeniaAmina TariqNo ratings yet
- Pediatric Acute Sepsis: Physician'S OrdersDocument4 pagesPediatric Acute Sepsis: Physician'S OrdersSughosh MitraNo ratings yet
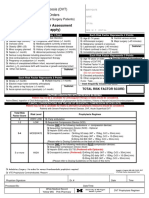
- Thrombosis Risk Factor Assessment (Choose All That Apply) : Deep Vein Thrombosis (DVT) Prophylaxis OrdersDocument2 pagesThrombosis Risk Factor Assessment (Choose All That Apply) : Deep Vein Thrombosis (DVT) Prophylaxis OrdersPutu Gizha Satrya GautamaNo ratings yet
- Leukemia Treatment Regimens 7937Document3 pagesLeukemia Treatment Regimens 7937Irfan FathurrahmanNo ratings yet
- L 51 R Hypercvad R MaDocument7 pagesL 51 R Hypercvad R MaMohamed MahmoudNo ratings yet
- Lomustine Ver 1Document6 pagesLomustine Ver 1soomro rehmanNo ratings yet
- Doxorubicin: Mechanism of ActionDocument3 pagesDoxorubicin: Mechanism of ActionGeorge FogNo ratings yet
- BRS62Document1 pageBRS62JaneNo ratings yet
- 596 Ifosfamide Etoposide Ie TherapyDocument6 pages596 Ifosfamide Etoposide Ie Therapyravindra0504090No ratings yet
- Secondary HLH Case Report: Highlighting Clinical ChallengesDocument11 pagesSecondary HLH Case Report: Highlighting Clinical ChallengesDr. Surya Abadi KristyoadiNo ratings yet
- Final Haad (DOH) ExamDocument9 pagesFinal Haad (DOH) ExamsenthamizhselvanNo ratings yet
- Drugs For Cancer Patients: Mona Shrestha MN (Adult Nursing)Document77 pagesDrugs For Cancer Patients: Mona Shrestha MN (Adult Nursing)sushma shresthaNo ratings yet
- NICU Drugs GuideDocument49 pagesNICU Drugs GuideArhanNo ratings yet
- PCV For High Grade Gliomas Protocol 09.12Document5 pagesPCV For High Grade Gliomas Protocol 09.12Bojan LukicNo ratings yet
- Oncology Cheat Sheets - 1Document5 pagesOncology Cheat Sheets - 1abdallahmaurice94No ratings yet
- Rancangan Bentuk Sediaan Farmasi Compatibility ModeDocument18 pagesRancangan Bentuk Sediaan Farmasi Compatibility ModeNully Andaretha SugiantoNo ratings yet
- VIDE v3Document3 pagesVIDE v3gonococo29No ratings yet
- Anticoagulation RegimensDocument1 pageAnticoagulation RegimensLame BossNo ratings yet
- Guideline: Antibiotic Drug Monitoring: Aminoglycosides and GlycopeptidesDocument8 pagesGuideline: Antibiotic Drug Monitoring: Aminoglycosides and GlycopeptidesKenRodulfReyesVillaruelNo ratings yet
- EPIRUBICIN Ferron PharmaceuticalsDocument7 pagesEPIRUBICIN Ferron PharmaceuticalsHep PutNo ratings yet
- Paclitaxel Trastuzumab Breast Cancer ProtocolDocument9 pagesPaclitaxel Trastuzumab Breast Cancer ProtocolsmokkerNo ratings yet
- Receiving Concurrent Moderate CYP3A4 Inhibitors (Erythromycin, Saquinavir, Verapamil, Fluconazole) - 25 MG Once Daily InitiallyDocument272 pagesReceiving Concurrent Moderate CYP3A4 Inhibitors (Erythromycin, Saquinavir, Verapamil, Fluconazole) - 25 MG Once Daily InitiallyFatima Doran PandaogNo ratings yet
- Perioperatif Antiemesis - Aiwi JapanesaDocument24 pagesPerioperatif Antiemesis - Aiwi JapanesafebrinasugiantoNo ratings yet
- Revision 1Document21 pagesRevision 1NaifmxNo ratings yet
- Concise Guide to Clinical Dentistry: Common Prescriptions In Clinical DentistryFrom EverandConcise Guide to Clinical Dentistry: Common Prescriptions In Clinical DentistryNo ratings yet
- Image Guided Radiotherapy Technique - IGRTDocument13 pagesImage Guided Radiotherapy Technique - IGRTbadusha vpNo ratings yet
- Online Appointment For Patients DSCI 31 July 2021Document9 pagesOnline Appointment For Patients DSCI 31 July 2021Prabhjot Kaur0% (1)
- Recent Advances in The Management of LiposarcomaDocument15 pagesRecent Advances in The Management of LiposarcomaBudhiNo ratings yet
- Genes Dev.-2010-Shen-1967-2000Document35 pagesGenes Dev.-2010-Shen-1967-2000Vanessa Anton MuñozNo ratings yet
- The New Version 9 American Joint Committee On CancDocument12 pagesThe New Version 9 American Joint Committee On CancardiNo ratings yet
- CA 19-9 Markers and Ca PancreasDocument13 pagesCA 19-9 Markers and Ca PancreasJose Tomás MooreNo ratings yet
- CV of BaifengZhang.2023Document3 pagesCV of BaifengZhang.2023Baifeng ZhangNo ratings yet
- PancreasDocument40 pagesPancreasMuthannah MarawanNo ratings yet
- Study of Cancer Investigatory ProjectDocument19 pagesStudy of Cancer Investigatory ProjectShivam Shankar AnandNo ratings yet
- Webinar Famiy Doctors 1 - 10 - 2020Document62 pagesWebinar Famiy Doctors 1 - 10 - 2020NoaEfratBen-BaruchNo ratings yet
- Brachytherapy To Treat CancerDocument2 pagesBrachytherapy To Treat CancerCrissel Kane CarpioNo ratings yet
- Mammography and Breast Localization For The InterventionalistDocument6 pagesMammography and Breast Localization For The InterventionalistrasminojNo ratings yet
- Neutrophil To Lymphocyte Ratio (NLR) As An Indicator of Poor Prognosis in Stage IV Non-Small Cell Lung CancerDocument6 pagesNeutrophil To Lymphocyte Ratio (NLR) As An Indicator of Poor Prognosis in Stage IV Non-Small Cell Lung CancerWilliamRayCassidyNo ratings yet
- Tumors of EyelidsDocument25 pagesTumors of Eyelidsabdulrehman akhtarNo ratings yet
- Tomita ScoreDocument11 pagesTomita ScoreMukharradhi NanzaNo ratings yet
- Odontogenic Tumors IIDocument24 pagesOdontogenic Tumors IIIbn HabibNo ratings yet
- Pap Smear Guidebook 2019Document73 pagesPap Smear Guidebook 2019Biorich ZilaNo ratings yet
- Monaco Hypofractionated Radiotherapy White PaperDocument10 pagesMonaco Hypofractionated Radiotherapy White Papersurenkumar100% (1)
- 65 - Approach To Patients With CancerDocument1 page65 - Approach To Patients With CancerRica Alyssa PepitoNo ratings yet
- Daftar Pustaka: Jurnal Pendidikan Khusus, 5 (2), 83-93Document3 pagesDaftar Pustaka: Jurnal Pendidikan Khusus, 5 (2), 83-93donatNo ratings yet
- Vulval CancerDocument9 pagesVulval CancerSana LodhiNo ratings yet
- AYUSHMAN BHAVA Launch OrderDocument9 pagesAYUSHMAN BHAVA Launch OrderChanmari West Sub-CentreNo ratings yet
- 22151a - RaySafe Pro Mam Accreditation Phantom - Flyer - enDocument2 pages22151a - RaySafe Pro Mam Accreditation Phantom - Flyer - enFernando RibicichNo ratings yet
- All Program 240423Document26 pagesAll Program 240423NoneNo ratings yet
- Hazardous Drugs - Pharmacy Services - LMPSDocument20 pagesHazardous Drugs - Pharmacy Services - LMPSphillip dunnNo ratings yet
- Social Event Cancare Day Campaign 2023 by IISE BINUS University Student Chapter #716Document6 pagesSocial Event Cancare Day Campaign 2023 by IISE BINUS University Student Chapter #716Octalianny HalimNo ratings yet
- Tugas Praktikum Kodefikasi PenyakitDocument6 pagesTugas Praktikum Kodefikasi Penyakitdewi candra agustinNo ratings yet
- Case Study 1Document6 pagesCase Study 1api-542345721No ratings yet
- What To Know About CancerDocument17 pagesWhat To Know About CancerKARL PASCUANo ratings yet
- The Origins of The NK Cell, or A Canadian in King Ivan's CourtDocument2 pagesThe Origins of The NK Cell, or A Canadian in King Ivan's Courthoangphuong08101992No ratings yet
























































































Download as pdf or txt
You might also like
- Etoposide Oral Sarcoma Protocol V1.0Document3 pagesEtoposide Oral Sarcoma Protocol V1.0أبو عبد الرحمن المحموديNo ratings yet
- Docetaxel Protocol V1.0Document6 pagesDocetaxel Protocol V1.0أبو عبد الرحمن المحموديNo ratings yet
- Protokol SarcomaDocument4 pagesProtokol SarcomaHep PutNo ratings yet
- Temozolomide Adjuvant NHSDocument5 pagesTemozolomide Adjuvant NHSSyed Touseef AhmedNo ratings yet
- Antimicrobial Dosage Adjustments in Renal Impairment For FormularyDocument20 pagesAntimicrobial Dosage Adjustments in Renal Impairment For Formularyangkatanjuli2019No ratings yet
- Carboplatin With Pemetrexed Pembrolizumab Non Squamous Non-Small Cell Lung Cancer Protocol V1.1Document8 pagesCarboplatin With Pemetrexed Pembrolizumab Non Squamous Non-Small Cell Lung Cancer Protocol V1.1Olaru DianaNo ratings yet
- 311 Topotecan Monotherapy 5 DayDocument4 pages311 Topotecan Monotherapy 5 DayRuxandra BănicăNo ratings yet
- Oncology Antiemetic PolicyDocument8 pagesOncology Antiemetic PolicyAnggy L, dr.No ratings yet
- Avelumab Merkel Cell Carcinoma Protocol V1.1Document6 pagesAvelumab Merkel Cell Carcinoma Protocol V1.1Vlad CroitoruNo ratings yet
- Aida Protocol For Apl: InductionDocument4 pagesAida Protocol For Apl: InductionGabrielNo ratings yet
- Heparin Dose Adjustment in The Prescence of Renal ImpairmentDocument5 pagesHeparin Dose Adjustment in The Prescence of Renal ImpairmentRPR KSVNo ratings yet
- SAAI Protocol KankerDocument4 pagesSAAI Protocol KankerSadha MahardhikaNo ratings yet
- Paclitaxel With Dose Dense EC Adjuvant or Neo-Adjuvant Protocol V1.0Document7 pagesPaclitaxel With Dose Dense EC Adjuvant or Neo-Adjuvant Protocol V1.0smokkerNo ratings yet
- CHLVPP (Hodgkin'S Lymphoma) : (Max: 10Mg) (Max: 10Mg)Document3 pagesCHLVPP (Hodgkin'S Lymphoma) : (Max: 10Mg) (Max: 10Mg)Sindu SankarNo ratings yet
- Imatinib For Philadelphia Chromosome Positive CML, First LineDocument4 pagesImatinib For Philadelphia Chromosome Positive CML, First LinehendranuraminNo ratings yet
- Neratinib Adjuvant Treatment Breast Cancer Protocol V1.1Document6 pagesNeratinib Adjuvant Treatment Breast Cancer Protocol V1.1smokkerNo ratings yet
- CVP Plus Rituximab (R-CVP) For Lymphoma: Page 1 of 2Document2 pagesCVP Plus Rituximab (R-CVP) For Lymphoma: Page 1 of 2Andreea NeculceaNo ratings yet
- EC-DH Epirubicin Cyclophosphamide Followed by Docetaxel With Trastuzumab Protocol V1.1Document11 pagesEC-DH Epirubicin Cyclophosphamide Followed by Docetaxel With Trastuzumab Protocol V1.1smokkerNo ratings yet
- Cyclophosphamide Doxorubicin Ver 1.1Document6 pagesCyclophosphamide Doxorubicin Ver 1.1Yudi ApriyantoNo ratings yet
- ASWCS10 HN001 Weekly Cisp and Radtx Final 110325 - AmendedJuly2012Document3 pagesASWCS10 HN001 Weekly Cisp and Radtx Final 110325 - AmendedJuly2012Kurnia AnharNo ratings yet
- Drug Study GentamicinDocument3 pagesDrug Study GentamicinEARL GERALD RICAFRANCANo ratings yet
- 1.13 Hyper-CVAD-MA Version 2.1Document5 pages1.13 Hyper-CVAD-MA Version 2.1Alina CrissNo ratings yet
- Paclitaxel Albumin Abraxane Breast Cancer V1.1Document7 pagesPaclitaxel Albumin Abraxane Breast Cancer V1.1smokkerNo ratings yet
- Enoxaparin - Prescribing, Administration and MonitoringDocument6 pagesEnoxaparin - Prescribing, Administration and MonitoringFaheem AlsabriaNo ratings yet
- Enoxaparin - Safe Prescribing - Check It Out 1Document3 pagesEnoxaparin - Safe Prescribing - Check It Out 1Zaid DewachiNo ratings yet
- RLE - Oncology NotesDocument2 pagesRLE - Oncology NotesmareginaNo ratings yet
- SCLC Cisplatin-Etoposide IVplusor-RT Protocol V1.1Document3 pagesSCLC Cisplatin-Etoposide IVplusor-RT Protocol V1.1vera docNo ratings yet
- Tramadol Plus ParacetamolDocument2 pagesTramadol Plus ParacetamolKeir Mrls ForcadillaNo ratings yet
- ABVDDocument3 pagesABVDEsther WanguiNo ratings yet
- Brajac - ProtocolDocument13 pagesBrajac - Protocolthanh ngôNo ratings yet
- Supportive Care During Cancer TreatmentDocument18 pagesSupportive Care During Cancer TreatmentDebs AngupaNo ratings yet
- Anticoagulation Protocol For PostDocument8 pagesAnticoagulation Protocol For PostMohammed IbrahimNo ratings yet
- Mitomycin - UsmanDocument3 pagesMitomycin - UsmanSittie Nashieva A. UsmanNo ratings yet
- Oncology Supportive CareDocument57 pagesOncology Supportive CaredewiNo ratings yet
- Case Study ThrombocytopeniaDocument8 pagesCase Study ThrombocytopeniaAmina TariqNo ratings yet
- Pediatric Acute Sepsis: Physician'S OrdersDocument4 pagesPediatric Acute Sepsis: Physician'S OrdersSughosh MitraNo ratings yet
- Thrombosis Risk Factor Assessment (Choose All That Apply) : Deep Vein Thrombosis (DVT) Prophylaxis OrdersDocument2 pagesThrombosis Risk Factor Assessment (Choose All That Apply) : Deep Vein Thrombosis (DVT) Prophylaxis OrdersPutu Gizha Satrya GautamaNo ratings yet
- Leukemia Treatment Regimens 7937Document3 pagesLeukemia Treatment Regimens 7937Irfan FathurrahmanNo ratings yet
- L 51 R Hypercvad R MaDocument7 pagesL 51 R Hypercvad R MaMohamed MahmoudNo ratings yet
- Lomustine Ver 1Document6 pagesLomustine Ver 1soomro rehmanNo ratings yet
- Doxorubicin: Mechanism of ActionDocument3 pagesDoxorubicin: Mechanism of ActionGeorge FogNo ratings yet
- BRS62Document1 pageBRS62JaneNo ratings yet
- 596 Ifosfamide Etoposide Ie TherapyDocument6 pages596 Ifosfamide Etoposide Ie Therapyravindra0504090No ratings yet
- Secondary HLH Case Report: Highlighting Clinical ChallengesDocument11 pagesSecondary HLH Case Report: Highlighting Clinical ChallengesDr. Surya Abadi KristyoadiNo ratings yet
- Final Haad (DOH) ExamDocument9 pagesFinal Haad (DOH) ExamsenthamizhselvanNo ratings yet
- Drugs For Cancer Patients: Mona Shrestha MN (Adult Nursing)Document77 pagesDrugs For Cancer Patients: Mona Shrestha MN (Adult Nursing)sushma shresthaNo ratings yet
- NICU Drugs GuideDocument49 pagesNICU Drugs GuideArhanNo ratings yet
- PCV For High Grade Gliomas Protocol 09.12Document5 pagesPCV For High Grade Gliomas Protocol 09.12Bojan LukicNo ratings yet
- Oncology Cheat Sheets - 1Document5 pagesOncology Cheat Sheets - 1abdallahmaurice94No ratings yet
- Rancangan Bentuk Sediaan Farmasi Compatibility ModeDocument18 pagesRancangan Bentuk Sediaan Farmasi Compatibility ModeNully Andaretha SugiantoNo ratings yet
- VIDE v3Document3 pagesVIDE v3gonococo29No ratings yet
- Anticoagulation RegimensDocument1 pageAnticoagulation RegimensLame BossNo ratings yet
- Guideline: Antibiotic Drug Monitoring: Aminoglycosides and GlycopeptidesDocument8 pagesGuideline: Antibiotic Drug Monitoring: Aminoglycosides and GlycopeptidesKenRodulfReyesVillaruelNo ratings yet
- EPIRUBICIN Ferron PharmaceuticalsDocument7 pagesEPIRUBICIN Ferron PharmaceuticalsHep PutNo ratings yet
- Paclitaxel Trastuzumab Breast Cancer ProtocolDocument9 pagesPaclitaxel Trastuzumab Breast Cancer ProtocolsmokkerNo ratings yet
- Receiving Concurrent Moderate CYP3A4 Inhibitors (Erythromycin, Saquinavir, Verapamil, Fluconazole) - 25 MG Once Daily InitiallyDocument272 pagesReceiving Concurrent Moderate CYP3A4 Inhibitors (Erythromycin, Saquinavir, Verapamil, Fluconazole) - 25 MG Once Daily InitiallyFatima Doran PandaogNo ratings yet
- Perioperatif Antiemesis - Aiwi JapanesaDocument24 pagesPerioperatif Antiemesis - Aiwi JapanesafebrinasugiantoNo ratings yet
- Revision 1Document21 pagesRevision 1NaifmxNo ratings yet
- Concise Guide to Clinical Dentistry: Common Prescriptions In Clinical DentistryFrom EverandConcise Guide to Clinical Dentistry: Common Prescriptions In Clinical DentistryNo ratings yet
- Image Guided Radiotherapy Technique - IGRTDocument13 pagesImage Guided Radiotherapy Technique - IGRTbadusha vpNo ratings yet
- Online Appointment For Patients DSCI 31 July 2021Document9 pagesOnline Appointment For Patients DSCI 31 July 2021Prabhjot Kaur0% (1)
- Recent Advances in The Management of LiposarcomaDocument15 pagesRecent Advances in The Management of LiposarcomaBudhiNo ratings yet
- Genes Dev.-2010-Shen-1967-2000Document35 pagesGenes Dev.-2010-Shen-1967-2000Vanessa Anton MuñozNo ratings yet
- The New Version 9 American Joint Committee On CancDocument12 pagesThe New Version 9 American Joint Committee On CancardiNo ratings yet
- CA 19-9 Markers and Ca PancreasDocument13 pagesCA 19-9 Markers and Ca PancreasJose Tomás MooreNo ratings yet
- CV of BaifengZhang.2023Document3 pagesCV of BaifengZhang.2023Baifeng ZhangNo ratings yet
- PancreasDocument40 pagesPancreasMuthannah MarawanNo ratings yet
- Study of Cancer Investigatory ProjectDocument19 pagesStudy of Cancer Investigatory ProjectShivam Shankar AnandNo ratings yet
- Webinar Famiy Doctors 1 - 10 - 2020Document62 pagesWebinar Famiy Doctors 1 - 10 - 2020NoaEfratBen-BaruchNo ratings yet
- Brachytherapy To Treat CancerDocument2 pagesBrachytherapy To Treat CancerCrissel Kane CarpioNo ratings yet
- Mammography and Breast Localization For The InterventionalistDocument6 pagesMammography and Breast Localization For The InterventionalistrasminojNo ratings yet
- Neutrophil To Lymphocyte Ratio (NLR) As An Indicator of Poor Prognosis in Stage IV Non-Small Cell Lung CancerDocument6 pagesNeutrophil To Lymphocyte Ratio (NLR) As An Indicator of Poor Prognosis in Stage IV Non-Small Cell Lung CancerWilliamRayCassidyNo ratings yet
- Tumors of EyelidsDocument25 pagesTumors of Eyelidsabdulrehman akhtarNo ratings yet
- Tomita ScoreDocument11 pagesTomita ScoreMukharradhi NanzaNo ratings yet
- Odontogenic Tumors IIDocument24 pagesOdontogenic Tumors IIIbn HabibNo ratings yet
- Pap Smear Guidebook 2019Document73 pagesPap Smear Guidebook 2019Biorich ZilaNo ratings yet
- Monaco Hypofractionated Radiotherapy White PaperDocument10 pagesMonaco Hypofractionated Radiotherapy White Papersurenkumar100% (1)
- 65 - Approach To Patients With CancerDocument1 page65 - Approach To Patients With CancerRica Alyssa PepitoNo ratings yet
- Daftar Pustaka: Jurnal Pendidikan Khusus, 5 (2), 83-93Document3 pagesDaftar Pustaka: Jurnal Pendidikan Khusus, 5 (2), 83-93donatNo ratings yet
- Vulval CancerDocument9 pagesVulval CancerSana LodhiNo ratings yet
- AYUSHMAN BHAVA Launch OrderDocument9 pagesAYUSHMAN BHAVA Launch OrderChanmari West Sub-CentreNo ratings yet
- 22151a - RaySafe Pro Mam Accreditation Phantom - Flyer - enDocument2 pages22151a - RaySafe Pro Mam Accreditation Phantom - Flyer - enFernando RibicichNo ratings yet
- All Program 240423Document26 pagesAll Program 240423NoneNo ratings yet
- Hazardous Drugs - Pharmacy Services - LMPSDocument20 pagesHazardous Drugs - Pharmacy Services - LMPSphillip dunnNo ratings yet
- Social Event Cancare Day Campaign 2023 by IISE BINUS University Student Chapter #716Document6 pagesSocial Event Cancare Day Campaign 2023 by IISE BINUS University Student Chapter #716Octalianny HalimNo ratings yet
- Tugas Praktikum Kodefikasi PenyakitDocument6 pagesTugas Praktikum Kodefikasi Penyakitdewi candra agustinNo ratings yet
- Case Study 1Document6 pagesCase Study 1api-542345721No ratings yet
- What To Know About CancerDocument17 pagesWhat To Know About CancerKARL PASCUANo ratings yet
- The Origins of The NK Cell, or A Canadian in King Ivan's CourtDocument2 pagesThe Origins of The NK Cell, or A Canadian in King Ivan's Courthoangphuong08101992No ratings yet