Download as pdf or txt
You might also like
- Provincial Finals Intermediate: Pack #4Document9 pagesProvincial Finals Intermediate: Pack #4lin xu100% (1)
- Er63419 Rev101 140628Document329 pagesEr63419 Rev101 140628Roman BeránekNo ratings yet
- Hofmaenner - Association Between Hypocholesterolemia and Mortality in Critically Ill Patients With Sepsis - A Systematic Review and Meta-AnalysisDocument10 pagesHofmaenner - Association Between Hypocholesterolemia and Mortality in Critically Ill Patients With Sepsis - A Systematic Review and Meta-AnalysisgiadungdanamallNo ratings yet
- Comparison of Inflammatory Markers in HTNDocument6 pagesComparison of Inflammatory Markers in HTNDan JohnstonNo ratings yet
- 1nnnnn ... A Qbqn2i29191s D..... Snsjwnwbs SSWQJQKQ 1111111 60-167Document8 pages1nnnnn ... A Qbqn2i29191s D..... Snsjwnwbs SSWQJQKQ 1111111 60-167Red DiggerNo ratings yet
- Lipid Profile in CKDDocument4 pagesLipid Profile in CKDAmiyanshu BeheraNo ratings yet
- Kidney Research and Clinical PracticeDocument8 pagesKidney Research and Clinical PracticepangaribuansantaNo ratings yet
- 25rakshitha EtalDocument8 pages25rakshitha EtaleditorijmrhsNo ratings yet
- MGvol81.2011 25Document8 pagesMGvol81.2011 25eminacengic5851No ratings yet
- Popa2009 PDFDocument6 pagesPopa2009 PDFHeinz FischerNo ratings yet
- Serum Uric Acid and Chronic Kidney Disease The Role of HypertensionDocument8 pagesSerum Uric Acid and Chronic Kidney Disease The Role of HypertensionAdam Adachi SanNo ratings yet
- Tugas Jurnal KardioDocument5 pagesTugas Jurnal KardioKiki AmandaNo ratings yet
- PB, Afect, Cardiovasc, Biomark, LDL, CholestDocument6 pagesPB, Afect, Cardiovasc, Biomark, LDL, CholestAna IsaNo ratings yet
- Cholesterol MS RADocument6 pagesCholesterol MS RATsamara YumnaNo ratings yet
- ILN Biomarker 2016Document6 pagesILN Biomarker 2016AlienNo ratings yet
- LIFE StudyDocument9 pagesLIFE StudySukma EffendyNo ratings yet
- Research Article Baseline Serum Uric Acid Levels Are Associated With All-Cause Mortality in Acute Coronary Syndrome Patients After Percutaneous Coronary InterventionDocument9 pagesResearch Article Baseline Serum Uric Acid Levels Are Associated With All-Cause Mortality in Acute Coronary Syndrome Patients After Percutaneous Coronary InterventionmikeNo ratings yet
- 1471 2369 14 191 PDFDocument9 pages1471 2369 14 191 PDFhanifahrafaNo ratings yet
- Significance of Serum Uric Acid Level in Patients of Stroke With Diabetes MellitusDocument4 pagesSignificance of Serum Uric Acid Level in Patients of Stroke With Diabetes MellitusIOSR Journal of PharmacyNo ratings yet
- METAANALYSIS Steroisds For ARDSDocument10 pagesMETAANALYSIS Steroisds For ARDSfretzie enguitoNo ratings yet
- 4 - 2015serum Lipoprotein (A) Concentrations Are Inversely Associated With T2D, Prediabetes, and Insulin ResDocument10 pages4 - 2015serum Lipoprotein (A) Concentrations Are Inversely Associated With T2D, Prediabetes, and Insulin Resjef5525No ratings yet
- The Efficacy and Safety of Triple Vs Dual Combination of ARB, CCB, and DiureticsDocument9 pagesThe Efficacy and Safety of Triple Vs Dual Combination of ARB, CCB, and DiureticsLucky PratamaNo ratings yet
- Metabolic Cardiovascular Disease Risk Factors and Their Clustering in Subclinical HypothyroidismDocument7 pagesMetabolic Cardiovascular Disease Risk Factors and Their Clustering in Subclinical HypothyroidismMaria Alice BourneufNo ratings yet
- 2014 Albumin ARDSDocument8 pages2014 Albumin ARDSJeltsin Chávarry AratíaNo ratings yet
- Kunutsor - 2016 - Serum Zinc Concentrations and Incident HypertensionDocument7 pagesKunutsor - 2016 - Serum Zinc Concentrations and Incident Hypertensionzi coNo ratings yet
- Impact of Community-Based Cardiac Rehabilitation On Clinical Parameters of Patients With Cardiovascular DiseasesDocument7 pagesImpact of Community-Based Cardiac Rehabilitation On Clinical Parameters of Patients With Cardiovascular DiseasesAfrizal FauziansyahNo ratings yet
- 8931 26614 2 PB PDFDocument7 pages8931 26614 2 PB PDFMaferNo ratings yet
- PrintDocument8 pagesPrintannarchyNo ratings yet
- Transfusiones Septic ShockDocument12 pagesTransfusiones Septic ShockKelvin George Huayllazo MerelNo ratings yet
- Investigations On Serum Lipid Profile in Patients With Urinary Tract InfectionsDocument3 pagesInvestigations On Serum Lipid Profile in Patients With Urinary Tract InfectionsJOHNKENNEDY NNODIMNo ratings yet
- JCH 12758Document6 pagesJCH 12758HanafieHeluthNo ratings yet
- Efeito Tratamento Hormonal No HDL Nos Trans (Exemplo de Resultados Esperados e Materiais e MétodosDocument10 pagesEfeito Tratamento Hormonal No HDL Nos Trans (Exemplo de Resultados Esperados e Materiais e MétodosHigor FerreiraNo ratings yet
- Study of Serum Electrolytes in Acute Exacerbation of Chronic Obstructive Pulmonary Disease PatientsDocument4 pagesStudy of Serum Electrolytes in Acute Exacerbation of Chronic Obstructive Pulmonary Disease PatientsTri UtomoNo ratings yet
- Medip, IJAM-2391 ODocument4 pagesMedip, IJAM-2391 OalitrnfbNo ratings yet
- Comparison of Fasting and Postprandial Levels of CDocument6 pagesComparison of Fasting and Postprandial Levels of CDaniel Reyes MNo ratings yet
- Vegetarian Diet, Seventh Day Adventists and Risk of CardiovascularDocument7 pagesVegetarian Diet, Seventh Day Adventists and Risk of CardiovascularJohn SammutNo ratings yet
- Correlation of Serum Osteocalcin Level With The Indices of Obesity and Lipid Profile in Type Ii Diabetic Sudanese PatientsDocument10 pagesCorrelation of Serum Osteocalcin Level With The Indices of Obesity and Lipid Profile in Type Ii Diabetic Sudanese PatientsIJAR JOURNALNo ratings yet
- ,content, 31,2,361 FullDocument2 pages,content, 31,2,361 FullMilka MimingNo ratings yet
- Jurnal Bu Sulis 1Document6 pagesJurnal Bu Sulis 1PitoAdhiNo ratings yet
- Efficacy and Safety of High-Density Lipoprotein Cholesterol-Increasing CompoundsDocument13 pagesEfficacy and Safety of High-Density Lipoprotein Cholesterol-Increasing CompoundsAdityasekar WangiNo ratings yet
- Case Study 2. Lipid AbnormalitiesDocument3 pagesCase Study 2. Lipid AbnormalitiesBryan Christian MadeloNo ratings yet
- Jurnal 6Document8 pagesJurnal 6OziNo ratings yet
- Research ArticleDocument9 pagesResearch ArticlemikeNo ratings yet
- Song 2014Document11 pagesSong 2014Ayssa WitjaksonoNo ratings yet
- 14perederii CorinaDocument6 pages14perederii CorinaCami ElenaNo ratings yet
- Pharmacology & Therapeutics: Anette Varbo, Marianne Benn, Børge G. NordestgaardDocument10 pagesPharmacology & Therapeutics: Anette Varbo, Marianne Benn, Børge G. NordestgaardIonuț CozmaNo ratings yet
- Nutrition Parameters As Hemodialysis Adequacy Markers: Original ArticleDocument5 pagesNutrition Parameters As Hemodialysis Adequacy Markers: Original ArticleMariska Widya WNo ratings yet
- 302 Cardiovascular Risk: AssessmentDocument1 page302 Cardiovascular Risk: AssessmentLêHữuHoàiNo ratings yet
- Applied-A Correlative Study of Hypertension-Raksha GoyalDocument8 pagesApplied-A Correlative Study of Hypertension-Raksha GoyalImpact JournalsNo ratings yet
- 9 - Efficacy, Safety, Tolerate, ApheresisDocument9 pages9 - Efficacy, Safety, Tolerate, Apheresisjef5525No ratings yet
- CD005425 AbstractDocument3 pagesCD005425 AbstractokisutartoNo ratings yet
- Stroke and LipidDocument4 pagesStroke and LipidvenniariskiaNo ratings yet
- Significance of Total Protein Albumin Globulin SerDocument5 pagesSignificance of Total Protein Albumin Globulin SerGabriella Berta SitompulNo ratings yet
- Oxidative Stress and Lipid Profile Among Hypertensive Patients at A Tertiary Centre in Kano, Northwest, NigeriaDocument9 pagesOxidative Stress and Lipid Profile Among Hypertensive Patients at A Tertiary Centre in Kano, Northwest, NigeriaidiNo ratings yet
- Green Tea Intake Lowers Fasting Serum Total and LDL Cholesterol in Adults: A Meta-Analysis of 14 Randomized Controlled TrialsDocument10 pagesGreen Tea Intake Lowers Fasting Serum Total and LDL Cholesterol in Adults: A Meta-Analysis of 14 Randomized Controlled TrialswheiinhyNo ratings yet
- Limited Salt Consumption Reduces The Incidence of Chronic Kidney Disease: A Modeling StudyDocument8 pagesLimited Salt Consumption Reduces The Incidence of Chronic Kidney Disease: A Modeling StudyanuNo ratings yet
- Serum Albumin Level Adjusted With C-Reactive Protein Predicts Hemodialysis Patient SurvivalDocument9 pagesSerum Albumin Level Adjusted With C-Reactive Protein Predicts Hemodialysis Patient Survivalmelda lestari haidirNo ratings yet
- (Kadar LDL Dan HDL Dalam Darah Model Tikus Periodontitis (Blood Level of LDL and HDL in Periodontitis Rat Model)Document5 pages(Kadar LDL Dan HDL Dalam Darah Model Tikus Periodontitis (Blood Level of LDL and HDL in Periodontitis Rat Model)Suma_DewiNo ratings yet
- Serum Concentrations of Adiponectin and Risk of Type 2 Diabetes Mellitus and Coronary Heart Disease in Apparently Healthy Middle-Aged MenDocument15 pagesSerum Concentrations of Adiponectin and Risk of Type 2 Diabetes Mellitus and Coronary Heart Disease in Apparently Healthy Middle-Aged MenEcha MagungNo ratings yet
- Int J Clinical Practice - 2010 - Sinan Deveci - The Association Between Serum Uric Acid Level and Coronary Artery DiseaseDocument8 pagesInt J Clinical Practice - 2010 - Sinan Deveci - The Association Between Serum Uric Acid Level and Coronary Artery DiseasealitrnfbNo ratings yet
- Complementary and Alternative Medical Lab Testing Part 8: UrologyFrom EverandComplementary and Alternative Medical Lab Testing Part 8: UrologyRating: 3 out of 5 stars3/5 (1)
- Complementary and Alternative Medical Lab Testing Part 4: VascularFrom EverandComplementary and Alternative Medical Lab Testing Part 4: VascularNo ratings yet
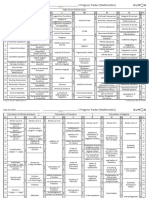
- Kumon Mathematics Progress Tracker Levels C To O PDFDocument2 pagesKumon Mathematics Progress Tracker Levels C To O PDFcharmradeekNo ratings yet
- Paraxylene Safety Data Sheet CPChemDocument14 pagesParaxylene Safety Data Sheet CPChemscribd405No ratings yet
- Hartalega Annual Report 2019 - Part 1Document57 pagesHartalega Annual Report 2019 - Part 1tanushara0No ratings yet
- TO Bus Rapid Transit (BRT) System: Hemant TiwariDocument48 pagesTO Bus Rapid Transit (BRT) System: Hemant TiwariHemant Tiwari100% (2)
- Hemhem Crown - WikipediaDocument2 pagesHemhem Crown - WikipediamanandpatelNo ratings yet
- Conduction Convection Radiation PowerpointDocument27 pagesConduction Convection Radiation PowerpointApet Satusembilansembilan JieNo ratings yet
- EFX By-Pass Level Transmitter - NewDocument32 pagesEFX By-Pass Level Transmitter - Newsaka dewaNo ratings yet
- TubosDocument12 pagesTubosASHIK TNo ratings yet
- BlueridgemountnsDocument37 pagesBlueridgemountnsကဗ်ာရည္းစားNo ratings yet
- DC SimpDocument3 pagesDC SimpNikhil HiremathNo ratings yet
- Final Project Flood ManagementDocument11 pagesFinal Project Flood ManagementJagat SinghNo ratings yet
- Mono - Probiotics - English MONOGRAFIA HEALTH CANADA - 0Document25 pagesMono - Probiotics - English MONOGRAFIA HEALTH CANADA - 0Farhan aliNo ratings yet
- Mucopolysaccharidoses EditedDocument6 pagesMucopolysaccharidoses EditedSamuel NjengaNo ratings yet
- Madame DoubtfireDocument110 pagesMadame Doubtfire快乐无忧的阿俊yxNo ratings yet
- ConsolidatedDocument46 pagesConsolidatedJ. Karthick Myilvahanan CSBSNo ratings yet
- HMI Design Process ENDocument2 pagesHMI Design Process ENSHNo ratings yet
- FAO - Climate Smart Agriculture SourcebookDocument570 pagesFAO - Climate Smart Agriculture Sourcebookeeeek100% (1)
- 04 MSDS Catalyst (Vandium Penta Oxide)Document6 pages04 MSDS Catalyst (Vandium Penta Oxide)Furqan SiddiquiNo ratings yet
- ChirdsDocument5 pagesChirdsWise FidelityNo ratings yet
- Yield of Cucumber Varieties To Be ContinuedDocument24 pagesYield of Cucumber Varieties To Be ContinuedMaideluz V. SandagNo ratings yet
- Pediatric Medication AdministrationDocument62 pagesPediatric Medication AdministrationJaezee RamosNo ratings yet
- Berube Et Al 2003 - Laboratory and Field Investigations of The Influence of Sodium Chloride On ASRDocument8 pagesBerube Et Al 2003 - Laboratory and Field Investigations of The Influence of Sodium Chloride On ASRrodrigo.vilela.gorgaNo ratings yet
- ECO #10 - 6th Dec, 2012Document2 pagesECO #10 - 6th Dec, 2012adoptnegotiatorNo ratings yet
- Radiology DVTDocument90 pagesRadiology DVTDhruv KushwahaNo ratings yet
- FMP Series: High Pressure Fi LtersDocument14 pagesFMP Series: High Pressure Fi LtersДаниіл ЩигельськийNo ratings yet
- Chap016.ppt Materials Requirements PlanningDocument25 pagesChap016.ppt Materials Requirements PlanningSaad Khadur EilyesNo ratings yet
- 6.VLSI Architecture Design For Analysis of Fast Locking ADPLL Via Feed Forward Compensation Algorithm (33-38)Document6 pages6.VLSI Architecture Design For Analysis of Fast Locking ADPLL Via Feed Forward Compensation Algorithm (33-38)ijcctsNo ratings yet
- BMEDocument11 pagesBMEtemesgen adugnaNo ratings yet