
Chapter 3 - Resp
Chapter 3 - Resp
You might also like
- A compilation of anabolic and nutritionnal supplementsFrom EverandA compilation of anabolic and nutritionnal supplementsRating: 4.5 out of 5 stars4.5/5 (2)
- FLCCC Alliance I RECOVER Management Protocol For Long Haul COVID 19 SyndromeDocument3 pagesFLCCC Alliance I RECOVER Management Protocol For Long Haul COVID 19 SyndromeAizaz ul HaqNo ratings yet
- FLCCC Alliance's I RECOVER Management Protocol For Long Haul COVID 19 SyndromeDocument3 pagesFLCCC Alliance's I RECOVER Management Protocol For Long Haul COVID 19 SyndromeAlan N100% (1)
- GINA Assessment of Asthma ControlDocument12 pagesGINA Assessment of Asthma ControlaranspeterNo ratings yet
- Stages of LaborDocument5 pagesStages of LaborGeraldine Marie Salvo100% (4)
- Principles of Management of MDR-TBDocument22 pagesPrinciples of Management of MDR-TBGeorge VergheseNo ratings yet
- Pharmacotherapy of Asthma: Asniar Pascayantri, S.Si., M.Si., AptDocument27 pagesPharmacotherapy of Asthma: Asniar Pascayantri, S.Si., M.Si., AptLeni Fitriani HamduNo ratings yet
- Bronchial Asthma: Marshell Tendean, MD Departemen of Internal Medicine UKRIDA - JakartaDocument39 pagesBronchial Asthma: Marshell Tendean, MD Departemen of Internal Medicine UKRIDA - JakartamiazaraNo ratings yet
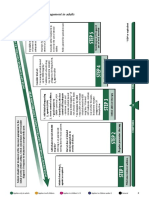
- Summary of Stepwise Management in AdultsDocument3 pagesSummary of Stepwise Management in AdultsHenrypat Uche OgbuduNo ratings yet
- Asthma+Clinicians+at A Glance+508 02-03-21Document6 pagesAsthma+Clinicians+at A Glance+508 02-03-21Noe SandovalNo ratings yet
- GINA Guidelines2019-DikonversiDocument36 pagesGINA Guidelines2019-Dikonversifelly iswaNo ratings yet
- Treatment GuidelinesDocument9 pagesTreatment GuidelinesEmmaNo ratings yet
- Hosp Ops II Week 2 Questions 1Document3 pagesHosp Ops II Week 2 Questions 1api-650133203No ratings yet
- Adult ( 18 Years) Asthma Quick Reference Guide (Update Nov 2017)Document2 pagesAdult ( 18 Years) Asthma Quick Reference Guide (Update Nov 2017)Nerissa Neri NatataNo ratings yet
- MALARIA DR - PAULDocument67 pagesMALARIA DR - PAULNodi Rahma DiniNo ratings yet
- CHBC and GPAC Provincial Asthma Guideline SummaryDocument1 pageCHBC and GPAC Provincial Asthma Guideline SummaryfisesaNo ratings yet
- Tuberculosis: Sudchaya Prasoetpan (R1 Silpakorn University Residency Program)Document56 pagesTuberculosis: Sudchaya Prasoetpan (R1 Silpakorn University Residency Program)moraceaebmNo ratings yet
- Penggunaan Kortikosteroid BaruDocument2 pagesPenggunaan Kortikosteroid Barudian prawitaNo ratings yet
- Asthma in Children: April 2014Document35 pagesAsthma in Children: April 2014abdisalaan hassanNo ratings yet
- Management of AsthmaDocument20 pagesManagement of Asthmazaidiarisha52No ratings yet
- Procacci Handouts1Document11 pagesProcacci Handouts1api-246046306100% (1)
- Rotherham CCG Asthma Guidelines FINAL MMC Version V6.1Document6 pagesRotherham CCG Asthma Guidelines FINAL MMC Version V6.1Verónica Rojas NavaNo ratings yet
- Management of Suspected Paediatric ThyrotoxicosisDocument5 pagesManagement of Suspected Paediatric ThyrotoxicosisCaity YoungNo ratings yet
- Summarised Clinchers Created For The Exam - Credits - Audi Maglalang-ReedDocument9 pagesSummarised Clinchers Created For The Exam - Credits - Audi Maglalang-ReedflashjetNo ratings yet
- 2021 Final - COVID 19 IN CHILDREN PROTOCOLDocument12 pages2021 Final - COVID 19 IN CHILDREN PROTOCOLSutirtha RoyNo ratings yet
- GINA 2022 Severe Asthma Slide Set 2Document22 pagesGINA 2022 Severe Asthma Slide Set 2Fitri RahmarianiNo ratings yet
- Anti-Tuberculosis Treatment: DR Wong VF Sibu GH 27/7/2013Document27 pagesAnti-Tuberculosis Treatment: DR Wong VF Sibu GH 27/7/2013Widy StefannyNo ratings yet
- Paediatricshouseofficerguidehospitalkulim 151026150042 Lva1 App6891Document14 pagesPaediatricshouseofficerguidehospitalkulim 151026150042 Lva1 App6891Nadia SalwaniNo ratings yet
- Medicine RotatationbookletDocument20 pagesMedicine RotatationbookletJanelle JosephsNo ratings yet
- Journal Reading AsthmaDocument12 pagesJournal Reading AsthmaMuhammad Ihsan AuliaNo ratings yet
- Asthma: Kaps PrepDocument21 pagesAsthma: Kaps PrepImee TingzonNo ratings yet
- SalbutamolDocument5 pagesSalbutamolFildehl Janice Bomediano CatipayNo ratings yet
- Asthma Guidelines 2011Document5 pagesAsthma Guidelines 2011oss-20502745No ratings yet
- Lin 2018Document13 pagesLin 2018Pamela JumpNo ratings yet
- New Drugs and Regimens For TB: 2015 Update: Scott K. Heysell MD, MPH (No Disclosures)Document21 pagesNew Drugs and Regimens For TB: 2015 Update: Scott K. Heysell MD, MPH (No Disclosures)Nop PiromNo ratings yet
- Recent TB Treatment GuidelinesDocument28 pagesRecent TB Treatment GuidelinesDr venkatesh jalluNo ratings yet
- Immediate Release - (Methylphenidate)Document4 pagesImmediate Release - (Methylphenidate)MaryNguyenNo ratings yet
- Clinical Toxicology Part 3Document13 pagesClinical Toxicology Part 3Muhammad Shahedul IslamNo ratings yet
- Key Drug Information: AlbuterolDocument1 pageKey Drug Information: Albuterolamaliea234No ratings yet
- RespiratorydrugsDocument1 pageRespiratorydrugshevere6273No ratings yet
- Benefits of SMART Therapy For Asthma ManagementDocument4 pagesBenefits of SMART Therapy For Asthma ManagementREDANo ratings yet
- Final Haad (DOH) ExamDocument9 pagesFinal Haad (DOH) ExamsenthamizhselvanNo ratings yet
- Management of DR-TB: PMDT GuidelineDocument41 pagesManagement of DR-TB: PMDT GuidelineSomnath Das GuptaNo ratings yet
- Guideline For Management Protocol of Children With Fever and Respiratory SymptomsDocument44 pagesGuideline For Management Protocol of Children With Fever and Respiratory SymptomsKushagr GautamNo ratings yet
- L Bronchial Asthma Management 2024Document54 pagesL Bronchial Asthma Management 2024wdsmhNo ratings yet
- Child With Fits in ED - Srl.Document2 pagesChild With Fits in ED - Srl.azeemNo ratings yet
- DrugsDocument5 pagesDrugsdeepika kushwahNo ratings yet
- DrugsDocument5 pagesDrugsdeepika kushwah100% (1)
- Management of Acute Asthma Exacerbation in Primary CareDocument2 pagesManagement of Acute Asthma Exacerbation in Primary CareValerie Anne BebitaNo ratings yet
- Cme Bronchial AsthmaDocument28 pagesCme Bronchial AsthmaameerabestNo ratings yet
- Drug StudyDocument7 pagesDrug StudyGladys NacionNo ratings yet
- AntipsychoticsDocument76 pagesAntipsychoticslysf908No ratings yet
- Common Tropical Disease in ThailandDocument84 pagesCommon Tropical Disease in ThailandDr.Sathaporn KunnathumNo ratings yet
- PulmoDocument18 pagesPulmoAllum KaribasappaNo ratings yet
- Final Anti TB in SP - SituationDocument50 pagesFinal Anti TB in SP - SituationAbdul JalilNo ratings yet
- PRN Asthma TXDocument29 pagesPRN Asthma TXisauraNo ratings yet
- Asthma:: Cortisone, Hydrocortisone (SoluDocument7 pagesAsthma:: Cortisone, Hydrocortisone (SoluWil LesterNo ratings yet
- 6 Palliative CareDocument4 pages6 Palliative CareDiana VillanuevaNo ratings yet
- Whats New in GINA 2016Document34 pagesWhats New in GINA 2016Jimmy Wea ChittiwanNo ratings yet
- Status Epilepticus GuidelineDocument2 pagesStatus Epilepticus GuidelineBalrajSinghNo ratings yet
- Respirology SectionDocument4 pagesRespirology SectionAmna KhanNo ratings yet
- Patogenesis Malaria - Dr. A. Visi Kartika, SP - PADocument26 pagesPatogenesis Malaria - Dr. A. Visi Kartika, SP - PAahmadyawidyatmaNo ratings yet
- Health, Stress, and CopingDocument49 pagesHealth, Stress, and CopingMarissa BrionesNo ratings yet
- This Presentation Deals With Ten Important Mudras That Can Result in Amazing Health BenefitsDocument12 pagesThis Presentation Deals With Ten Important Mudras That Can Result in Amazing Health BenefitsnitinshyamNo ratings yet
- University of Cebu College of Nursing Banilad, Cebu CityDocument3 pagesUniversity of Cebu College of Nursing Banilad, Cebu Cityjapheth01No ratings yet
- AnalogiesDocument12 pagesAnalogiesharpriyaminhasNo ratings yet
- The Impact of The Flexible Partial Denture Base On The Alveolar Mucosa in Comparison To Metallic Denture RCT and Histological StudyDocument7 pagesThe Impact of The Flexible Partial Denture Base On The Alveolar Mucosa in Comparison To Metallic Denture RCT and Histological StudyZachary DuongNo ratings yet
- Historical AntecedentsDocument17 pagesHistorical AntecedentsBench Adrian AvilaNo ratings yet
- Icha 1Document5 pagesIcha 1kadek ayu ichaNo ratings yet
- Employees Compensation and State Insurance Fund HandoutDocument19 pagesEmployees Compensation and State Insurance Fund HandoutDanice Go GanNo ratings yet
- Literature Review On Packed Cell VolumeDocument4 pagesLiterature Review On Packed Cell Volumeaflsqrbnq100% (1)
- Central Nervous System Involvement in Adults With Acute Leukemia: Diagnosis, Prevention, and ManagementDocument10 pagesCentral Nervous System Involvement in Adults With Acute Leukemia: Diagnosis, Prevention, and ManagementYo MeNo ratings yet
- Question Bank in Biology Class XIIDocument64 pagesQuestion Bank in Biology Class XIIaleena'No ratings yet
- Analysis of Aspirin in Commercial Apc Tablet Using Ftir SpectrosDocument5 pagesAnalysis of Aspirin in Commercial Apc Tablet Using Ftir SpectrosMay Lee100% (1)
- Triangular Fibrocartilage Complex Injury in Professional CricketersDocument5 pagesTriangular Fibrocartilage Complex Injury in Professional Cricketersrima rizky nourliaNo ratings yet
- How To Lose Belly Fats in 20 Days Guaranteed (Action Required)Document3 pagesHow To Lose Belly Fats in 20 Days Guaranteed (Action Required)Idongesit KoffiNo ratings yet
- General Dermatology NotesDocument6 pagesGeneral Dermatology NotesPenny_Teoh_3451No ratings yet
- Nursing Practice: Betty Neuman'S-Neuman'S System ModelDocument5 pagesNursing Practice: Betty Neuman'S-Neuman'S System ModelKate DabucolNo ratings yet
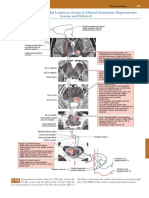
- Posterior Column-Medial Lemniscus System in Clinical Orientation: Representative Lesions and DeficitsDocument1 pagePosterior Column-Medial Lemniscus System in Clinical Orientation: Representative Lesions and DeficitsEduardo RodriguezNo ratings yet
- Gandhi - Collected Works Vol 12Document487 pagesGandhi - Collected Works Vol 12Nrusimha ( नृसिंह )No ratings yet
- Mechanical Ventilation in NeonatesDocument60 pagesMechanical Ventilation in NeonatesZuhair Aldajani زهير عمر الدجاني100% (3)
- PANRE and PANCE Review NeurologyDocument15 pagesPANRE and PANCE Review NeurologyThe Physician Assistant Life60% (5)
- Pituitary Adenoma FinalDocument44 pagesPituitary Adenoma FinalTuhinaRaj100% (1)
- Expanded SkeletonsDocument25 pagesExpanded SkeletonsKristopher Garrett100% (3)
- Sase Reviewer (Science)Document9 pagesSase Reviewer (Science)Ashley Jean CosmianoNo ratings yet
- Mapeh Grade 6 Active Body: Quarter 1 Week 5 Module 1Document34 pagesMapeh Grade 6 Active Body: Quarter 1 Week 5 Module 1reena joyceNo ratings yet
- Research Article: Cyanoacrylate For Intraoral Wound Closure: A Possibility?Document7 pagesResearch Article: Cyanoacrylate For Intraoral Wound Closure: A Possibility?Kikilis AčiuvisNo ratings yet
- AESGP Conference Report Brussels 2017Document27 pagesAESGP Conference Report Brussels 2017aesgpNo ratings yet
- Science 10 Quarter 3 Week 5 1Document5 pagesScience 10 Quarter 3 Week 5 1Celeste PalogmeNo ratings yet
- Chromosomal AberrationsDocument17 pagesChromosomal AberrationsHajiRab NawazNo ratings yet
























































































Download as pdf or txt
You might also like
- A compilation of anabolic and nutritionnal supplementsFrom EverandA compilation of anabolic and nutritionnal supplementsRating: 4.5 out of 5 stars4.5/5 (2)
- FLCCC Alliance I RECOVER Management Protocol For Long Haul COVID 19 SyndromeDocument3 pagesFLCCC Alliance I RECOVER Management Protocol For Long Haul COVID 19 SyndromeAizaz ul HaqNo ratings yet
- FLCCC Alliance's I RECOVER Management Protocol For Long Haul COVID 19 SyndromeDocument3 pagesFLCCC Alliance's I RECOVER Management Protocol For Long Haul COVID 19 SyndromeAlan N100% (1)
- GINA Assessment of Asthma ControlDocument12 pagesGINA Assessment of Asthma ControlaranspeterNo ratings yet
- Stages of LaborDocument5 pagesStages of LaborGeraldine Marie Salvo100% (4)
- Principles of Management of MDR-TBDocument22 pagesPrinciples of Management of MDR-TBGeorge VergheseNo ratings yet
- Pharmacotherapy of Asthma: Asniar Pascayantri, S.Si., M.Si., AptDocument27 pagesPharmacotherapy of Asthma: Asniar Pascayantri, S.Si., M.Si., AptLeni Fitriani HamduNo ratings yet
- Bronchial Asthma: Marshell Tendean, MD Departemen of Internal Medicine UKRIDA - JakartaDocument39 pagesBronchial Asthma: Marshell Tendean, MD Departemen of Internal Medicine UKRIDA - JakartamiazaraNo ratings yet
- Summary of Stepwise Management in AdultsDocument3 pagesSummary of Stepwise Management in AdultsHenrypat Uche OgbuduNo ratings yet
- Asthma+Clinicians+at A Glance+508 02-03-21Document6 pagesAsthma+Clinicians+at A Glance+508 02-03-21Noe SandovalNo ratings yet
- GINA Guidelines2019-DikonversiDocument36 pagesGINA Guidelines2019-Dikonversifelly iswaNo ratings yet
- Treatment GuidelinesDocument9 pagesTreatment GuidelinesEmmaNo ratings yet
- Hosp Ops II Week 2 Questions 1Document3 pagesHosp Ops II Week 2 Questions 1api-650133203No ratings yet
- Adult ( 18 Years) Asthma Quick Reference Guide (Update Nov 2017)Document2 pagesAdult ( 18 Years) Asthma Quick Reference Guide (Update Nov 2017)Nerissa Neri NatataNo ratings yet
- MALARIA DR - PAULDocument67 pagesMALARIA DR - PAULNodi Rahma DiniNo ratings yet
- CHBC and GPAC Provincial Asthma Guideline SummaryDocument1 pageCHBC and GPAC Provincial Asthma Guideline SummaryfisesaNo ratings yet
- Tuberculosis: Sudchaya Prasoetpan (R1 Silpakorn University Residency Program)Document56 pagesTuberculosis: Sudchaya Prasoetpan (R1 Silpakorn University Residency Program)moraceaebmNo ratings yet
- Penggunaan Kortikosteroid BaruDocument2 pagesPenggunaan Kortikosteroid Barudian prawitaNo ratings yet
- Asthma in Children: April 2014Document35 pagesAsthma in Children: April 2014abdisalaan hassanNo ratings yet
- Management of AsthmaDocument20 pagesManagement of Asthmazaidiarisha52No ratings yet
- Procacci Handouts1Document11 pagesProcacci Handouts1api-246046306100% (1)
- Rotherham CCG Asthma Guidelines FINAL MMC Version V6.1Document6 pagesRotherham CCG Asthma Guidelines FINAL MMC Version V6.1Verónica Rojas NavaNo ratings yet
- Management of Suspected Paediatric ThyrotoxicosisDocument5 pagesManagement of Suspected Paediatric ThyrotoxicosisCaity YoungNo ratings yet
- Summarised Clinchers Created For The Exam - Credits - Audi Maglalang-ReedDocument9 pagesSummarised Clinchers Created For The Exam - Credits - Audi Maglalang-ReedflashjetNo ratings yet
- 2021 Final - COVID 19 IN CHILDREN PROTOCOLDocument12 pages2021 Final - COVID 19 IN CHILDREN PROTOCOLSutirtha RoyNo ratings yet
- GINA 2022 Severe Asthma Slide Set 2Document22 pagesGINA 2022 Severe Asthma Slide Set 2Fitri RahmarianiNo ratings yet
- Anti-Tuberculosis Treatment: DR Wong VF Sibu GH 27/7/2013Document27 pagesAnti-Tuberculosis Treatment: DR Wong VF Sibu GH 27/7/2013Widy StefannyNo ratings yet
- Paediatricshouseofficerguidehospitalkulim 151026150042 Lva1 App6891Document14 pagesPaediatricshouseofficerguidehospitalkulim 151026150042 Lva1 App6891Nadia SalwaniNo ratings yet
- Medicine RotatationbookletDocument20 pagesMedicine RotatationbookletJanelle JosephsNo ratings yet
- Journal Reading AsthmaDocument12 pagesJournal Reading AsthmaMuhammad Ihsan AuliaNo ratings yet
- Asthma: Kaps PrepDocument21 pagesAsthma: Kaps PrepImee TingzonNo ratings yet
- SalbutamolDocument5 pagesSalbutamolFildehl Janice Bomediano CatipayNo ratings yet
- Asthma Guidelines 2011Document5 pagesAsthma Guidelines 2011oss-20502745No ratings yet
- Lin 2018Document13 pagesLin 2018Pamela JumpNo ratings yet
- New Drugs and Regimens For TB: 2015 Update: Scott K. Heysell MD, MPH (No Disclosures)Document21 pagesNew Drugs and Regimens For TB: 2015 Update: Scott K. Heysell MD, MPH (No Disclosures)Nop PiromNo ratings yet
- Recent TB Treatment GuidelinesDocument28 pagesRecent TB Treatment GuidelinesDr venkatesh jalluNo ratings yet
- Immediate Release - (Methylphenidate)Document4 pagesImmediate Release - (Methylphenidate)MaryNguyenNo ratings yet
- Clinical Toxicology Part 3Document13 pagesClinical Toxicology Part 3Muhammad Shahedul IslamNo ratings yet
- Key Drug Information: AlbuterolDocument1 pageKey Drug Information: Albuterolamaliea234No ratings yet
- RespiratorydrugsDocument1 pageRespiratorydrugshevere6273No ratings yet
- Benefits of SMART Therapy For Asthma ManagementDocument4 pagesBenefits of SMART Therapy For Asthma ManagementREDANo ratings yet
- Final Haad (DOH) ExamDocument9 pagesFinal Haad (DOH) ExamsenthamizhselvanNo ratings yet
- Management of DR-TB: PMDT GuidelineDocument41 pagesManagement of DR-TB: PMDT GuidelineSomnath Das GuptaNo ratings yet
- Guideline For Management Protocol of Children With Fever and Respiratory SymptomsDocument44 pagesGuideline For Management Protocol of Children With Fever and Respiratory SymptomsKushagr GautamNo ratings yet
- L Bronchial Asthma Management 2024Document54 pagesL Bronchial Asthma Management 2024wdsmhNo ratings yet
- Child With Fits in ED - Srl.Document2 pagesChild With Fits in ED - Srl.azeemNo ratings yet
- DrugsDocument5 pagesDrugsdeepika kushwahNo ratings yet
- DrugsDocument5 pagesDrugsdeepika kushwah100% (1)
- Management of Acute Asthma Exacerbation in Primary CareDocument2 pagesManagement of Acute Asthma Exacerbation in Primary CareValerie Anne BebitaNo ratings yet
- Cme Bronchial AsthmaDocument28 pagesCme Bronchial AsthmaameerabestNo ratings yet
- Drug StudyDocument7 pagesDrug StudyGladys NacionNo ratings yet
- AntipsychoticsDocument76 pagesAntipsychoticslysf908No ratings yet
- Common Tropical Disease in ThailandDocument84 pagesCommon Tropical Disease in ThailandDr.Sathaporn KunnathumNo ratings yet
- PulmoDocument18 pagesPulmoAllum KaribasappaNo ratings yet
- Final Anti TB in SP - SituationDocument50 pagesFinal Anti TB in SP - SituationAbdul JalilNo ratings yet
- PRN Asthma TXDocument29 pagesPRN Asthma TXisauraNo ratings yet
- Asthma:: Cortisone, Hydrocortisone (SoluDocument7 pagesAsthma:: Cortisone, Hydrocortisone (SoluWil LesterNo ratings yet
- 6 Palliative CareDocument4 pages6 Palliative CareDiana VillanuevaNo ratings yet
- Whats New in GINA 2016Document34 pagesWhats New in GINA 2016Jimmy Wea ChittiwanNo ratings yet
- Status Epilepticus GuidelineDocument2 pagesStatus Epilepticus GuidelineBalrajSinghNo ratings yet
- Respirology SectionDocument4 pagesRespirology SectionAmna KhanNo ratings yet
- Patogenesis Malaria - Dr. A. Visi Kartika, SP - PADocument26 pagesPatogenesis Malaria - Dr. A. Visi Kartika, SP - PAahmadyawidyatmaNo ratings yet
- Health, Stress, and CopingDocument49 pagesHealth, Stress, and CopingMarissa BrionesNo ratings yet
- This Presentation Deals With Ten Important Mudras That Can Result in Amazing Health BenefitsDocument12 pagesThis Presentation Deals With Ten Important Mudras That Can Result in Amazing Health BenefitsnitinshyamNo ratings yet
- University of Cebu College of Nursing Banilad, Cebu CityDocument3 pagesUniversity of Cebu College of Nursing Banilad, Cebu Cityjapheth01No ratings yet
- AnalogiesDocument12 pagesAnalogiesharpriyaminhasNo ratings yet
- The Impact of The Flexible Partial Denture Base On The Alveolar Mucosa in Comparison To Metallic Denture RCT and Histological StudyDocument7 pagesThe Impact of The Flexible Partial Denture Base On The Alveolar Mucosa in Comparison To Metallic Denture RCT and Histological StudyZachary DuongNo ratings yet
- Historical AntecedentsDocument17 pagesHistorical AntecedentsBench Adrian AvilaNo ratings yet
- Icha 1Document5 pagesIcha 1kadek ayu ichaNo ratings yet
- Employees Compensation and State Insurance Fund HandoutDocument19 pagesEmployees Compensation and State Insurance Fund HandoutDanice Go GanNo ratings yet
- Literature Review On Packed Cell VolumeDocument4 pagesLiterature Review On Packed Cell Volumeaflsqrbnq100% (1)
- Central Nervous System Involvement in Adults With Acute Leukemia: Diagnosis, Prevention, and ManagementDocument10 pagesCentral Nervous System Involvement in Adults With Acute Leukemia: Diagnosis, Prevention, and ManagementYo MeNo ratings yet
- Question Bank in Biology Class XIIDocument64 pagesQuestion Bank in Biology Class XIIaleena'No ratings yet
- Analysis of Aspirin in Commercial Apc Tablet Using Ftir SpectrosDocument5 pagesAnalysis of Aspirin in Commercial Apc Tablet Using Ftir SpectrosMay Lee100% (1)
- Triangular Fibrocartilage Complex Injury in Professional CricketersDocument5 pagesTriangular Fibrocartilage Complex Injury in Professional Cricketersrima rizky nourliaNo ratings yet
- How To Lose Belly Fats in 20 Days Guaranteed (Action Required)Document3 pagesHow To Lose Belly Fats in 20 Days Guaranteed (Action Required)Idongesit KoffiNo ratings yet
- General Dermatology NotesDocument6 pagesGeneral Dermatology NotesPenny_Teoh_3451No ratings yet
- Nursing Practice: Betty Neuman'S-Neuman'S System ModelDocument5 pagesNursing Practice: Betty Neuman'S-Neuman'S System ModelKate DabucolNo ratings yet
- Posterior Column-Medial Lemniscus System in Clinical Orientation: Representative Lesions and DeficitsDocument1 pagePosterior Column-Medial Lemniscus System in Clinical Orientation: Representative Lesions and DeficitsEduardo RodriguezNo ratings yet
- Gandhi - Collected Works Vol 12Document487 pagesGandhi - Collected Works Vol 12Nrusimha ( नृसिंह )No ratings yet
- Mechanical Ventilation in NeonatesDocument60 pagesMechanical Ventilation in NeonatesZuhair Aldajani زهير عمر الدجاني100% (3)
- PANRE and PANCE Review NeurologyDocument15 pagesPANRE and PANCE Review NeurologyThe Physician Assistant Life60% (5)
- Pituitary Adenoma FinalDocument44 pagesPituitary Adenoma FinalTuhinaRaj100% (1)
- Expanded SkeletonsDocument25 pagesExpanded SkeletonsKristopher Garrett100% (3)
- Sase Reviewer (Science)Document9 pagesSase Reviewer (Science)Ashley Jean CosmianoNo ratings yet
- Mapeh Grade 6 Active Body: Quarter 1 Week 5 Module 1Document34 pagesMapeh Grade 6 Active Body: Quarter 1 Week 5 Module 1reena joyceNo ratings yet
- Research Article: Cyanoacrylate For Intraoral Wound Closure: A Possibility?Document7 pagesResearch Article: Cyanoacrylate For Intraoral Wound Closure: A Possibility?Kikilis AčiuvisNo ratings yet
- AESGP Conference Report Brussels 2017Document27 pagesAESGP Conference Report Brussels 2017aesgpNo ratings yet
- Science 10 Quarter 3 Week 5 1Document5 pagesScience 10 Quarter 3 Week 5 1Celeste PalogmeNo ratings yet
- Chromosomal AberrationsDocument17 pagesChromosomal AberrationsHajiRab NawazNo ratings yet