Download as pdf or txt
You might also like
- SSRI (Selective Serotonin Reuptake Inhibitor)Document1 pageSSRI (Selective Serotonin Reuptake Inhibitor)Mike EveretteNo ratings yet
- Kidney Disease Community Health PresentationDocument17 pagesKidney Disease Community Health PresentationVanessa FloresNo ratings yet
- Psychoanalytical Impact On O Neill S Long Day S Journey Into NightDocument2 pagesPsychoanalytical Impact On O Neill S Long Day S Journey Into NightKinaz Gul100% (1)
- Anxiolytics (289-290) SharlyDocument2 pagesAnxiolytics (289-290) SharlySharly Mae PanchoNo ratings yet
- Analgesics Non-Narcotic Analgesics Non-Narcotic Analgesics Common Uses What I Need To Know As A Brand New NurseDocument2 pagesAnalgesics Non-Narcotic Analgesics Non-Narcotic Analgesics Common Uses What I Need To Know As A Brand New NurseDilausan B MolukNo ratings yet
- PAiN SYnDrOmEs (Reviewer)Document19 pagesPAiN SYnDrOmEs (Reviewer)Agum, Philip James P.No ratings yet
- AmantadineDocument3 pagesAmantadineLina Marcela Portilla PrietoNo ratings yet
- Mental HealthDocument6 pagesMental HealtholadapoNo ratings yet
- Drug Study GabapentinDocument3 pagesDrug Study Gabapentinbridget.badiang001No ratings yet
- 0903CP Article1Document7 pages0903CP Article1Patricia Cavalcanti RibeiroNo ratings yet
- الانسومنيا المحاضره+ وزاريDocument6 pagesالانسومنيا المحاضره+ وزاريبراء طاهر حاتمNo ratings yet
- Drug Study (Tofranil J Zoloft)Document2 pagesDrug Study (Tofranil J Zoloft)alteahmichaella.mintuNo ratings yet
- Headache Management Guideline For Adults Version 10Document6 pagesHeadache Management Guideline For Adults Version 10TomiNo ratings yet
- Injections: 2.5mg/ml in CNS: Drowsiness,: DroperidolDocument3 pagesInjections: 2.5mg/ml in CNS: Drowsiness,: DroperidolthesarayoNo ratings yet
- Er-Drug StudyDocument41 pagesEr-Drug Studyrc_lacampuinganyahooNo ratings yet
- Tramadol and Related ProductsDocument63 pagesTramadol and Related ProductsWrhaeyna MarieNo ratings yet
- Benylin 4 Flu Susp.Document3 pagesBenylin 4 Flu Susp.Young MaxxNo ratings yet
- LosartanDocument1 pageLosartanBiya MacunteNo ratings yet
- PhenobarbitalDocument1 pagePhenobarbitalSherwin LauronNo ratings yet
- Exam 1 Drug ResumeDocument8 pagesExam 1 Drug Resumecpmv0410No ratings yet
- Anxiolytic DrugDocument3 pagesAnxiolytic DrugAnna Mendiola-BasbasNo ratings yet
- Beri151216 w1Document1 pageBeri151216 w1Lunatiku TraderNo ratings yet
- Tramadol NestDocument9 pagesTramadol NestAbegail PolicarpioNo ratings yet
- Drug StudyDocument3 pagesDrug StudyAlyssa Marie PepitoNo ratings yet
- Adult: IV/IM 5-10 MG, Drowsiness, Fatigue, Ataxia,: Injectable Form: ShockDocument1 pageAdult: IV/IM 5-10 MG, Drowsiness, Fatigue, Ataxia,: Injectable Form: ShockinfectionmanNo ratings yet
- Negatil Tablet: What Is in This LeafletDocument2 pagesNegatil Tablet: What Is in This LeafletEe JoNo ratings yet
- Algoritmo BenzoDocument2 pagesAlgoritmo BenzoGabriela BarreiraNo ratings yet
- FluoxetineDocument2 pagesFluoxetineSherena NicolasNo ratings yet
- ValiumDocument1 pageValiumJess MatiasNo ratings yet
- Imipramine Tofranil Melipamine Phenelzine Nardil Drug StudyDocument5 pagesImipramine Tofranil Melipamine Phenelzine Nardil Drug StudyHamimah Bint Ali100% (1)
- BuspironeDocument2 pagesBuspironeFatima Diane S. MondejarNo ratings yet
- Generic Name: Trade Name: Dosage: 15mgDocument3 pagesGeneric Name: Trade Name: Dosage: 15mgWILMARIE SAPANTANo ratings yet
- Drug StudyDocument2 pagesDrug StudyAlyssa Marie PepitoNo ratings yet
- Commonly Used Medication For Older AdultsDocument3 pagesCommonly Used Medication For Older AdultsRaze AlemaniaNo ratings yet
- DRUGSDocument5 pagesDRUGSDanica EspejoNo ratings yet
- BIPERIDENDocument3 pagesBIPERIDENDenise GabatoNo ratings yet
- Drug Study NCP FormatDocument6 pagesDrug Study NCP FormatPrincess Javier TorcelinoNo ratings yet
- Drug Study AlzheimersDocument12 pagesDrug Study Alzheimersella retizaNo ratings yet
- Unit 4 - Emergency Drugs - Table FormDocument5 pagesUnit 4 - Emergency Drugs - Table FormTESORO Zeus DavidNo ratings yet
- Pain Agitation and Delirium (PAD) UHL Critical Care GuidelineDocument35 pagesPain Agitation and Delirium (PAD) UHL Critical Care GuidelineLollapallooza 23No ratings yet
- Top 5 Drugs For Perianesthetic AnalgesiaDocument17 pagesTop 5 Drugs For Perianesthetic AnalgesiaPrakash KhangalNo ratings yet
- Tramadol, Paracetamol, Calmoseptine, B12Document5 pagesTramadol, Paracetamol, Calmoseptine, B12Denise EspinosaNo ratings yet
- Diazepam Tablets BP 10mg - PIL PDFDocument2 pagesDiazepam Tablets BP 10mg - PIL PDFOdunlamiNo ratings yet
- Linagliptin, Norgesic ForteDocument4 pagesLinagliptin, Norgesic FortehahahaNo ratings yet
- DS GadDocument2 pagesDS Gadbianca musicNo ratings yet
- Drug Study by Ivy DecenaDocument6 pagesDrug Study by Ivy DecenaIvy Mae DecenaNo ratings yet
- Drug Study (Tramadol)Document1 pageDrug Study (Tramadol)Baji ۦۦNo ratings yet
- Module 5: Chemotherapies Unit 2: Anti-Anxiety Drugs (Anxiolytics)Document8 pagesModule 5: Chemotherapies Unit 2: Anti-Anxiety Drugs (Anxiolytics)Luz TanNo ratings yet
- T Wycross 1984Document6 pagesT Wycross 1984Ha HaNo ratings yet
- Drug Study (Geria)Document7 pagesDrug Study (Geria)nicoleNo ratings yet
- SAFETY ALERT: Clients Taking An Anti-Anxiety Drug Should NotDocument4 pagesSAFETY ALERT: Clients Taking An Anti-Anxiety Drug Should NotMelissa HarndenNo ratings yet
- Forcadilla - Drug Study orDocument31 pagesForcadilla - Drug Study orKeir Mrls ForcadillaNo ratings yet
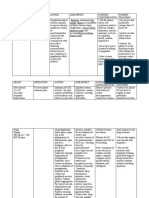
- Drug Name Classification Dosage/ Indication Mechanism of Action Contraindication Side Effect/ Adverse Effect Nursing ResponsibilitiesDocument2 pagesDrug Name Classification Dosage/ Indication Mechanism of Action Contraindication Side Effect/ Adverse Effect Nursing ResponsibilitiesEula Angelica OcoNo ratings yet
- IX. Drug StudyDocument4 pagesIX. Drug StudykingpinNo ratings yet
- !KULIAH Adjuvant AnalgesiaDocument31 pages!KULIAH Adjuvant AnalgesiaHilmi HidayatNo ratings yet
- AnxiolyticsDocument16 pagesAnxiolyticsChengDNo ratings yet
- Drug Study (Chlordiazepoxide, Lorazepam)Document4 pagesDrug Study (Chlordiazepoxide, Lorazepam)Kuro Hanabusa100% (2)
- Drugstudy Liver CirrhosisDocument5 pagesDrugstudy Liver CirrhosisBunnie AlphaNo ratings yet
- Difflam Drug StudyDocument1 pageDifflam Drug StudyDanlee EstandaNo ratings yet
- Depression & Anxiety: What You Need To Know About Treatment with Medications, Herbs & SupplementsFrom EverandDepression & Anxiety: What You Need To Know About Treatment with Medications, Herbs & SupplementsNo ratings yet
- Trigeminal Neuralgia, A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsFrom EverandTrigeminal Neuralgia, A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsNo ratings yet
- A Simple Guide to Neuralgia and Related Nerve DisordersFrom EverandA Simple Guide to Neuralgia and Related Nerve DisordersRating: 5 out of 5 stars5/5 (5)
- 1555-Article Text-5883-3-10-20200229Document11 pages1555-Article Text-5883-3-10-20200229Siti lestarinurhamidahNo ratings yet
- Interview QuestionsDocument1 pageInterview QuestionsRichieDaisyNo ratings yet
- STOPP5Document1 pageSTOPP5David BatesNo ratings yet
- 10 Z - Menik 2019 PDFDocument8 pages10 Z - Menik 2019 PDFAriF mauLNo ratings yet
- List of Licensed Free Standing Dialysis Clinics As of December 31, 2017Document23 pagesList of Licensed Free Standing Dialysis Clinics As of December 31, 2017jefferson velonzaNo ratings yet
- REBTDocument18 pagesREBTGayathree ChandranNo ratings yet
- Thyroid Disease in PregnancyDocument36 pagesThyroid Disease in Pregnancypeni_dwiNo ratings yet
- Diagnosis and Management of Cystic Fibrosis: Rosalind L SmythDocument6 pagesDiagnosis and Management of Cystic Fibrosis: Rosalind L SmythMuhammadShahzadNo ratings yet
- Short Scar Rhytidectomy Tech 2014 Atlas of The Oral and Maxillofacial SurgerDocument16 pagesShort Scar Rhytidectomy Tech 2014 Atlas of The Oral and Maxillofacial Surgerlaljadeff12No ratings yet
- Simmond's Disease MSDocument22 pagesSimmond's Disease MSRocel Devilles100% (1)
- Superficial Heating ModalitiesDocument19 pagesSuperficial Heating ModalitiesLoganathan Chandrasekar100% (1)
- Methane (CH) : Material Safety Data Sheet ForDocument7 pagesMethane (CH) : Material Safety Data Sheet Forسجاد الحلاويNo ratings yet
- Social Work Counseling Content Lesson 3Document10 pagesSocial Work Counseling Content Lesson 3joel lacayNo ratings yet
- MSDS Dulux Weathershield Powerflexx Inggris - ENGDocument11 pagesMSDS Dulux Weathershield Powerflexx Inggris - ENGtintucinbNo ratings yet
- Sneha KalpanaDocument7 pagesSneha KalpanachaithraM KulalNo ratings yet
- Presentation 1Document21 pagesPresentation 1Sharice CoscolluelaNo ratings yet
- MMM MachineDocument27 pagesMMM Machinej100% (1)
- Business ProposalDocument5 pagesBusiness Proposalapi-299665237No ratings yet
- Kidney Biopsy: A Guide For PatientsDocument12 pagesKidney Biopsy: A Guide For PatientsfirdausNo ratings yet
- MBG4234234 PDFDocument531 pagesMBG4234234 PDFVishwamedhi Kadavilla100% (1)
- 08 - Privileges - Orthopaedics SurgeryDocument3 pages08 - Privileges - Orthopaedics SurgeryAccreditation ConsultantNo ratings yet
- Starch Industry in IndiaDocument3 pagesStarch Industry in Indiabanapte59No ratings yet
- Storage Prevention of MedicinesDocument13 pagesStorage Prevention of MedicinestanishaNo ratings yet
- Generic NameDocument6 pagesGeneric NameKimsha ConcepcionNo ratings yet
- Leisure Awareness ActivitiesDocument9 pagesLeisure Awareness Activitiesapi-301398957No ratings yet
- Crohn Vs ColitisDocument5 pagesCrohn Vs Colitiswbarnes7No ratings yet
- What I Know? What I Want To Know? What I Learn?: John Andrei D. Dela Cruz Understanding Calories Grade 11-STEMDocument1 pageWhat I Know? What I Want To Know? What I Learn?: John Andrei D. Dela Cruz Understanding Calories Grade 11-STEMAnonymous Bryju9No ratings yet
- Foundation Concepts 1. Foundation ConceptsDocument30 pagesFoundation Concepts 1. Foundation ConceptsGlenna Joy SolsonaNo ratings yet