
Article Appraisal 1
Article Appraisal 1
You might also like
- HEALTH ASSESSMENT Syllabus 2023 2Document16 pagesHEALTH ASSESSMENT Syllabus 2023 2Raibert Rosales100% (1)
- Yousaf Ali (Auth.) - Self Assessment Questions in Rheumatology-Humana Press (2009)Document147 pagesYousaf Ali (Auth.) - Self Assessment Questions in Rheumatology-Humana Press (2009)Amr AmalNo ratings yet
- Pedia QuizesDocument19 pagesPedia QuizesPraneeth PaletiNo ratings yet
- Clinical Evaluation Tools Ver 2 First PageDocument3 pagesClinical Evaluation Tools Ver 2 First Pageapi-3697326No ratings yet
- Case Analysis RLE MODULE TEMPLATE Nursery 1 (One)Document7 pagesCase Analysis RLE MODULE TEMPLATE Nursery 1 (One)PanJan BalNo ratings yet
- Imposition Studio User GuideDocument45 pagesImposition Studio User Guidemrclprnt100% (1)
- LGDocument12 pagesLGFaisal Khan JaisiNo ratings yet
- 2008 Civil ProcedureDocument142 pages2008 Civil ProcedureDi CanNo ratings yet
- Civil ProcedureDocument20 pagesCivil ProcedureRitch LibonNo ratings yet
- Clinical Performance Evaluation Tool: Name: Year/Section/Group: Inclusive Dates: Area and ShiftDocument3 pagesClinical Performance Evaluation Tool: Name: Year/Section/Group: Inclusive Dates: Area and ShiftJONATHAN JAY MALITNo ratings yet
- Disturbances in Digestion and AbsorptionDocument115 pagesDisturbances in Digestion and AbsorptionGabrielle PamaNo ratings yet
- Physical AssessmentDocument51 pagesPhysical AssessmentJasmin Jacob100% (2)
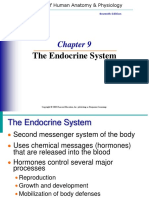
- The Endocrine System: Seventh EditionDocument40 pagesThe Endocrine System: Seventh EditionAngelaNo ratings yet
- Community Health Nursing Diagnostic IIDocument9 pagesCommunity Health Nursing Diagnostic IIPaul EspinosaNo ratings yet
- H.E CHAPTER 2 Historical Development and Concepts of Health 1Document35 pagesH.E CHAPTER 2 Historical Development and Concepts of Health 1Gumama AmeiyrhaNo ratings yet
- Activity 2 Answer The Following Questions: 10 Points EachDocument4 pagesActivity 2 Answer The Following Questions: 10 Points EachArmySapphireNo ratings yet
- Test Bank For Health Assessment in Nursing 3 Har CDR Edition Janet R WeberDocument6 pagesTest Bank For Health Assessment in Nursing 3 Har CDR Edition Janet R Weberirisadele7s3x8No ratings yet
- Chapter 1. History and Physical Examination - Art and ScienceDocument3 pagesChapter 1. History and Physical Examination - Art and SciencecarolineNo ratings yet
- BLOOD SPECIMEN CollectionDocument12 pagesBLOOD SPECIMEN CollectionJohn Henry G. Gabriel IV100% (11)
- 10 Community Oriented Primary CareDocument3 pages10 Community Oriented Primary CareIrene Veron Bernardo ChicoNo ratings yet
- Digestive-System QADocument6 pagesDigestive-System QASageNo ratings yet
- Health Education LM Week 1 and 2Document8 pagesHealth Education LM Week 1 and 2Joice LenteriaNo ratings yet
- Bioethics Lec 6, 7, 8, 9 11 12 13Document20 pagesBioethics Lec 6, 7, 8, 9 11 12 13Lynette Roldan RNNo ratings yet
- Guthrie Test Is One of Screening Test For Amino Acid Especially To DetectDocument6 pagesGuthrie Test Is One of Screening Test For Amino Acid Especially To DetectAyioKunNo ratings yet
- Nursing Jurisprudence Ethics and Legalit PDFDocument342 pagesNursing Jurisprudence Ethics and Legalit PDFElizabella Henrietta TanaquilNo ratings yet
- Biliran Province State University: ISO 9001:2015 CERTIFIED School of Nursing and Health SciencesDocument9 pagesBiliran Province State University: ISO 9001:2015 CERTIFIED School of Nursing and Health SciencesMaia Saivi OmegaNo ratings yet
- Teaching and LearningDocument11 pagesTeaching and LearningNovee Jane Arangote Ceriño100% (1)
- Guidelines For The Conduct of The Oral Revalida For Clinical Clerks (Batch 2020)Document2 pagesGuidelines For The Conduct of The Oral Revalida For Clinical Clerks (Batch 2020)mhegan07No ratings yet
- Quiz 1Document3 pagesQuiz 1Wiljohn de la CruzNo ratings yet
- R.A. No. 11509 Doktor para Sa Bayan ActDocument14 pagesR.A. No. 11509 Doktor para Sa Bayan ActAngel BacaniNo ratings yet
- Withholding and Withdrawing Life SupportDocument3 pagesWithholding and Withdrawing Life SupportNURSETOPNOTCHERNo ratings yet
- Clinical Chemistry QuestionsDocument5 pagesClinical Chemistry QuestionsEric C. CentenoNo ratings yet
- The 4 Box Method - Practical ApproachDocument39 pagesThe 4 Box Method - Practical ApproachramwshNo ratings yet
- CD PD 2.1 NECK 2017 Bates Outline PDFDocument3 pagesCD PD 2.1 NECK 2017 Bates Outline PDFGiaFelicianoNo ratings yet
- Synopsis 8TH AAAAaaDocument19 pagesSynopsis 8TH AAAAaaعثمان علیNo ratings yet
- Trans 1 - BioethicsDocument2 pagesTrans 1 - BioethicsRencel Hope BañezNo ratings yet
- Health Economics: Teacher: Teresita Balgos Reporter: Group 4 MLS-II FDocument19 pagesHealth Economics: Teacher: Teresita Balgos Reporter: Group 4 MLS-II FThyrealle Frances Sorongon100% (1)
- Although Some Vision As Been Lost and Cannot Be Restored, Further Loss May Be Prevented by Adhering To The Treatment Plan.Document8 pagesAlthough Some Vision As Been Lost and Cannot Be Restored, Further Loss May Be Prevented by Adhering To The Treatment Plan.Juma Sammy100% (1)
- CA 1 Resource UnitDocument8 pagesCA 1 Resource UnitPerlie Loren Arreo Cabatingan100% (1)
- Peritonitis: Email AddressDocument65 pagesPeritonitis: Email AddressJhon JefriNo ratings yet
- AAU Senate Legislation of 2019Document178 pagesAAU Senate Legislation of 2019carelessmanNo ratings yet
- NCM 102Document23 pagesNCM 102Aileen A. MonaresNo ratings yet
- Nursing Process Approach-Identification of Health Illness, Health Behaviour, Sign and Symptoms of CleintDocument27 pagesNursing Process Approach-Identification of Health Illness, Health Behaviour, Sign and Symptoms of CleintPinki BarmanNo ratings yet
- Palm Sas 1 13 CompilationDocument39 pagesPalm Sas 1 13 CompilationShyn MargarethNo ratings yet
- Endo GI Extra QuestionsDocument3 pagesEndo GI Extra QuestionsToni Marie Buenconsejo PunzalanNo ratings yet
- Dummy TablesDocument5 pagesDummy TablesAldrece CastroverdeNo ratings yet
- NCM 102 Chapter 5 Principles of Good Teaching PracticeDocument34 pagesNCM 102 Chapter 5 Principles of Good Teaching Practiceyzzabelle villaflorNo ratings yet
- 419 MidtermDocument28 pages419 MidtermANDREW DEL ROSARIONo ratings yet
- Med Tech Laws Reviewer 1-1Document15 pagesMed Tech Laws Reviewer 1-1lachicajustinnicoleNo ratings yet
- Examination of The Newborn InfantDocument15 pagesExamination of The Newborn InfantWilda AwliaNo ratings yet
- Ra PD Eo AoDocument3 pagesRa PD Eo AoAndy FrigillanaNo ratings yet
- NUTRITIONALASSESSMENT27102018PSMDocument48 pagesNUTRITIONALASSESSMENT27102018PSMRomani Pal100% (1)
- Urinary CalculiDocument2 pagesUrinary CalculiJayceeniPatricia CoronelNo ratings yet
- Nur 4242 Practicum Log 1Document2 pagesNur 4242 Practicum Log 1api-447860598No ratings yet
- Gordons 11 Functional Health PatternDocument18 pagesGordons 11 Functional Health PatternMae Antonette OrlinaNo ratings yet
- The Health History and Interviewing Process 2Document25 pagesThe Health History and Interviewing Process 2Mitul PeterNo ratings yet
- DR Checklist Intrapartal CompetenciesDocument3 pagesDR Checklist Intrapartal CompetenciesRussel PamaNo ratings yet
- Demo Teaching Physical Health AssessmentDocument5 pagesDemo Teaching Physical Health AssessmentJulie May SuganobNo ratings yet
- Assessment of The Heart and Neck VesselsDocument7 pagesAssessment of The Heart and Neck Vesselsclyde i amNo ratings yet
- Test BlueprintDocument2 pagesTest BlueprintAde AlcarazNo ratings yet
- Assessing The Musculoskeletal SystemDocument4 pagesAssessing The Musculoskeletal SystemtmdoreenNo ratings yet
- Article 1 AppraisalDocument4 pagesArticle 1 Appraisalapi-621026204No ratings yet
- Community Service HoursDocument2 pagesCommunity Service Hoursapi-670980669No ratings yet
- Allos Brink Schneider Manuscript FinalDocument39 pagesAllos Brink Schneider Manuscript Finalapi-670980669No ratings yet
- Professional Behaviors AssignmentDocument2 pagesProfessional Behaviors Assignmentapi-670980669No ratings yet
- Handout 2Document3 pagesHandout 2api-670980669No ratings yet
- Final PosterDocument1 pageFinal Posterapi-670980669No ratings yet
- Mechanical Method For Soil CompactionDocument63 pagesMechanical Method For Soil Compactionhawk_shahin100% (2)
- Listening Test: Directions: For Each Question in This Part, You Will Hear Four Statements About A Picture in YourDocument40 pagesListening Test: Directions: For Each Question in This Part, You Will Hear Four Statements About A Picture in YourTrương Hữu LộcNo ratings yet
- Entrepreneurship Development (BM-302) : Assignment 1Document7 pagesEntrepreneurship Development (BM-302) : Assignment 1AbhishekNo ratings yet
- UNIT-1: Linear Wave ShapingDocument24 pagesUNIT-1: Linear Wave Shapingmahender1987No ratings yet
- Aditya Solanki Expriment No.2Document5 pagesAditya Solanki Expriment No.2Kertik SinghNo ratings yet
- Alfa Laval SanitaryDocument10 pagesAlfa Laval SanitaryShrinivas TamaskarNo ratings yet
- Research Paper About Asian CuisineDocument8 pagesResearch Paper About Asian Cuisineikofdvbnd100% (1)
- 24 Wlic Index PlusDocument12 pages24 Wlic Index PlusSrinivasan KannanNo ratings yet
- Department of Defense Climate Adaptation PlanDocument32 pagesDepartment of Defense Climate Adaptation PlanCFHeatherNo ratings yet
- Heidenhain TNC 620 CatalogueDocument96 pagesHeidenhain TNC 620 CatalogueDörky LefieuwNo ratings yet
- STANAG 3101eed15Document30 pagesSTANAG 3101eed15Anselmo Alvarez GonzalezNo ratings yet
- 02 Laboratory Exercise 1 TemplateDocument11 pages02 Laboratory Exercise 1 TemplateMarie OsorioNo ratings yet
- Unit 9: Joint Products, Cost Allocation and by Products ContentDocument20 pagesUnit 9: Joint Products, Cost Allocation and by Products Contentዝምታ ተሻለNo ratings yet
- CIBSE Pipe Sizing V2Document13 pagesCIBSE Pipe Sizing V2Sameer UddinNo ratings yet
- Generic Attribute Profile (GATT) Specification - Bluetooth Technology Website PDFDocument3 pagesGeneric Attribute Profile (GATT) Specification - Bluetooth Technology Website PDFAshok Siva Kumar PoojalaNo ratings yet
- Legal Hurdle in Gaming PaymentDocument9 pagesLegal Hurdle in Gaming Paymentanurag kumarNo ratings yet
- Sales IncentiveDocument77 pagesSales Incentivebidiec100% (1)
- Full Ebook of Atkins Physical Chemistry Peter Atkins Online PDF All ChapterDocument69 pagesFull Ebook of Atkins Physical Chemistry Peter Atkins Online PDF All Chapterjessaeynmaei100% (5)
- The Rise and Fall of Levi StraussDocument6 pagesThe Rise and Fall of Levi StraussMark ElbenNo ratings yet
- School Forms Checking ReportDocument10 pagesSchool Forms Checking ReportRODNIE GUBATONNo ratings yet
- Final MKTDocument34 pagesFinal MKTHong Anh VuNo ratings yet
- TranscriptsDocument474 pagesTranscriptsToàn Huỳnh ThanhNo ratings yet
- D-5 Track Maintenance Activities - Part 4Document35 pagesD-5 Track Maintenance Activities - Part 4rajeshengasst89No ratings yet
- Family Case Study On The Billones Family 1Document63 pagesFamily Case Study On The Billones Family 1Ivy Mae DecenaNo ratings yet
- Anti Microbial DrugsDocument18 pagesAnti Microbial Drugseyadballas35No ratings yet
- Lecture 1 General Properties of Viruses 2021Document70 pagesLecture 1 General Properties of Viruses 2021Suresh Krishnani0% (1)
- NTPC Sabbatical SchemeDocument10 pagesNTPC Sabbatical Schemedhanu sreeNo ratings yet
- User - S - Manual Thermometer PDFDocument22 pagesUser - S - Manual Thermometer PDFjuanNo ratings yet




























































































Download as docx, pdf, or txt
You might also like
- HEALTH ASSESSMENT Syllabus 2023 2Document16 pagesHEALTH ASSESSMENT Syllabus 2023 2Raibert Rosales100% (1)
- Yousaf Ali (Auth.) - Self Assessment Questions in Rheumatology-Humana Press (2009)Document147 pagesYousaf Ali (Auth.) - Self Assessment Questions in Rheumatology-Humana Press (2009)Amr AmalNo ratings yet
- Pedia QuizesDocument19 pagesPedia QuizesPraneeth PaletiNo ratings yet
- Clinical Evaluation Tools Ver 2 First PageDocument3 pagesClinical Evaluation Tools Ver 2 First Pageapi-3697326No ratings yet
- Case Analysis RLE MODULE TEMPLATE Nursery 1 (One)Document7 pagesCase Analysis RLE MODULE TEMPLATE Nursery 1 (One)PanJan BalNo ratings yet
- Imposition Studio User GuideDocument45 pagesImposition Studio User Guidemrclprnt100% (1)
- LGDocument12 pagesLGFaisal Khan JaisiNo ratings yet
- 2008 Civil ProcedureDocument142 pages2008 Civil ProcedureDi CanNo ratings yet
- Civil ProcedureDocument20 pagesCivil ProcedureRitch LibonNo ratings yet
- Clinical Performance Evaluation Tool: Name: Year/Section/Group: Inclusive Dates: Area and ShiftDocument3 pagesClinical Performance Evaluation Tool: Name: Year/Section/Group: Inclusive Dates: Area and ShiftJONATHAN JAY MALITNo ratings yet
- Disturbances in Digestion and AbsorptionDocument115 pagesDisturbances in Digestion and AbsorptionGabrielle PamaNo ratings yet
- Physical AssessmentDocument51 pagesPhysical AssessmentJasmin Jacob100% (2)
- The Endocrine System: Seventh EditionDocument40 pagesThe Endocrine System: Seventh EditionAngelaNo ratings yet
- Community Health Nursing Diagnostic IIDocument9 pagesCommunity Health Nursing Diagnostic IIPaul EspinosaNo ratings yet
- H.E CHAPTER 2 Historical Development and Concepts of Health 1Document35 pagesH.E CHAPTER 2 Historical Development and Concepts of Health 1Gumama AmeiyrhaNo ratings yet
- Activity 2 Answer The Following Questions: 10 Points EachDocument4 pagesActivity 2 Answer The Following Questions: 10 Points EachArmySapphireNo ratings yet
- Test Bank For Health Assessment in Nursing 3 Har CDR Edition Janet R WeberDocument6 pagesTest Bank For Health Assessment in Nursing 3 Har CDR Edition Janet R Weberirisadele7s3x8No ratings yet
- Chapter 1. History and Physical Examination - Art and ScienceDocument3 pagesChapter 1. History and Physical Examination - Art and SciencecarolineNo ratings yet
- BLOOD SPECIMEN CollectionDocument12 pagesBLOOD SPECIMEN CollectionJohn Henry G. Gabriel IV100% (11)
- 10 Community Oriented Primary CareDocument3 pages10 Community Oriented Primary CareIrene Veron Bernardo ChicoNo ratings yet
- Digestive-System QADocument6 pagesDigestive-System QASageNo ratings yet
- Health Education LM Week 1 and 2Document8 pagesHealth Education LM Week 1 and 2Joice LenteriaNo ratings yet
- Bioethics Lec 6, 7, 8, 9 11 12 13Document20 pagesBioethics Lec 6, 7, 8, 9 11 12 13Lynette Roldan RNNo ratings yet
- Guthrie Test Is One of Screening Test For Amino Acid Especially To DetectDocument6 pagesGuthrie Test Is One of Screening Test For Amino Acid Especially To DetectAyioKunNo ratings yet
- Nursing Jurisprudence Ethics and Legalit PDFDocument342 pagesNursing Jurisprudence Ethics and Legalit PDFElizabella Henrietta TanaquilNo ratings yet
- Biliran Province State University: ISO 9001:2015 CERTIFIED School of Nursing and Health SciencesDocument9 pagesBiliran Province State University: ISO 9001:2015 CERTIFIED School of Nursing and Health SciencesMaia Saivi OmegaNo ratings yet
- Teaching and LearningDocument11 pagesTeaching and LearningNovee Jane Arangote Ceriño100% (1)
- Guidelines For The Conduct of The Oral Revalida For Clinical Clerks (Batch 2020)Document2 pagesGuidelines For The Conduct of The Oral Revalida For Clinical Clerks (Batch 2020)mhegan07No ratings yet
- Quiz 1Document3 pagesQuiz 1Wiljohn de la CruzNo ratings yet
- R.A. No. 11509 Doktor para Sa Bayan ActDocument14 pagesR.A. No. 11509 Doktor para Sa Bayan ActAngel BacaniNo ratings yet
- Withholding and Withdrawing Life SupportDocument3 pagesWithholding and Withdrawing Life SupportNURSETOPNOTCHERNo ratings yet
- Clinical Chemistry QuestionsDocument5 pagesClinical Chemistry QuestionsEric C. CentenoNo ratings yet
- The 4 Box Method - Practical ApproachDocument39 pagesThe 4 Box Method - Practical ApproachramwshNo ratings yet
- CD PD 2.1 NECK 2017 Bates Outline PDFDocument3 pagesCD PD 2.1 NECK 2017 Bates Outline PDFGiaFelicianoNo ratings yet
- Synopsis 8TH AAAAaaDocument19 pagesSynopsis 8TH AAAAaaعثمان علیNo ratings yet
- Trans 1 - BioethicsDocument2 pagesTrans 1 - BioethicsRencel Hope BañezNo ratings yet
- Health Economics: Teacher: Teresita Balgos Reporter: Group 4 MLS-II FDocument19 pagesHealth Economics: Teacher: Teresita Balgos Reporter: Group 4 MLS-II FThyrealle Frances Sorongon100% (1)
- Although Some Vision As Been Lost and Cannot Be Restored, Further Loss May Be Prevented by Adhering To The Treatment Plan.Document8 pagesAlthough Some Vision As Been Lost and Cannot Be Restored, Further Loss May Be Prevented by Adhering To The Treatment Plan.Juma Sammy100% (1)
- CA 1 Resource UnitDocument8 pagesCA 1 Resource UnitPerlie Loren Arreo Cabatingan100% (1)
- Peritonitis: Email AddressDocument65 pagesPeritonitis: Email AddressJhon JefriNo ratings yet
- AAU Senate Legislation of 2019Document178 pagesAAU Senate Legislation of 2019carelessmanNo ratings yet
- NCM 102Document23 pagesNCM 102Aileen A. MonaresNo ratings yet
- Nursing Process Approach-Identification of Health Illness, Health Behaviour, Sign and Symptoms of CleintDocument27 pagesNursing Process Approach-Identification of Health Illness, Health Behaviour, Sign and Symptoms of CleintPinki BarmanNo ratings yet
- Palm Sas 1 13 CompilationDocument39 pagesPalm Sas 1 13 CompilationShyn MargarethNo ratings yet
- Endo GI Extra QuestionsDocument3 pagesEndo GI Extra QuestionsToni Marie Buenconsejo PunzalanNo ratings yet
- Dummy TablesDocument5 pagesDummy TablesAldrece CastroverdeNo ratings yet
- NCM 102 Chapter 5 Principles of Good Teaching PracticeDocument34 pagesNCM 102 Chapter 5 Principles of Good Teaching Practiceyzzabelle villaflorNo ratings yet
- 419 MidtermDocument28 pages419 MidtermANDREW DEL ROSARIONo ratings yet
- Med Tech Laws Reviewer 1-1Document15 pagesMed Tech Laws Reviewer 1-1lachicajustinnicoleNo ratings yet
- Examination of The Newborn InfantDocument15 pagesExamination of The Newborn InfantWilda AwliaNo ratings yet
- Ra PD Eo AoDocument3 pagesRa PD Eo AoAndy FrigillanaNo ratings yet
- NUTRITIONALASSESSMENT27102018PSMDocument48 pagesNUTRITIONALASSESSMENT27102018PSMRomani Pal100% (1)
- Urinary CalculiDocument2 pagesUrinary CalculiJayceeniPatricia CoronelNo ratings yet
- Nur 4242 Practicum Log 1Document2 pagesNur 4242 Practicum Log 1api-447860598No ratings yet
- Gordons 11 Functional Health PatternDocument18 pagesGordons 11 Functional Health PatternMae Antonette OrlinaNo ratings yet
- The Health History and Interviewing Process 2Document25 pagesThe Health History and Interviewing Process 2Mitul PeterNo ratings yet
- DR Checklist Intrapartal CompetenciesDocument3 pagesDR Checklist Intrapartal CompetenciesRussel PamaNo ratings yet
- Demo Teaching Physical Health AssessmentDocument5 pagesDemo Teaching Physical Health AssessmentJulie May SuganobNo ratings yet
- Assessment of The Heart and Neck VesselsDocument7 pagesAssessment of The Heart and Neck Vesselsclyde i amNo ratings yet
- Test BlueprintDocument2 pagesTest BlueprintAde AlcarazNo ratings yet
- Assessing The Musculoskeletal SystemDocument4 pagesAssessing The Musculoskeletal SystemtmdoreenNo ratings yet
- Article 1 AppraisalDocument4 pagesArticle 1 Appraisalapi-621026204No ratings yet
- Community Service HoursDocument2 pagesCommunity Service Hoursapi-670980669No ratings yet
- Allos Brink Schneider Manuscript FinalDocument39 pagesAllos Brink Schneider Manuscript Finalapi-670980669No ratings yet
- Professional Behaviors AssignmentDocument2 pagesProfessional Behaviors Assignmentapi-670980669No ratings yet
- Handout 2Document3 pagesHandout 2api-670980669No ratings yet
- Final PosterDocument1 pageFinal Posterapi-670980669No ratings yet
- Mechanical Method For Soil CompactionDocument63 pagesMechanical Method For Soil Compactionhawk_shahin100% (2)
- Listening Test: Directions: For Each Question in This Part, You Will Hear Four Statements About A Picture in YourDocument40 pagesListening Test: Directions: For Each Question in This Part, You Will Hear Four Statements About A Picture in YourTrương Hữu LộcNo ratings yet
- Entrepreneurship Development (BM-302) : Assignment 1Document7 pagesEntrepreneurship Development (BM-302) : Assignment 1AbhishekNo ratings yet
- UNIT-1: Linear Wave ShapingDocument24 pagesUNIT-1: Linear Wave Shapingmahender1987No ratings yet
- Aditya Solanki Expriment No.2Document5 pagesAditya Solanki Expriment No.2Kertik SinghNo ratings yet
- Alfa Laval SanitaryDocument10 pagesAlfa Laval SanitaryShrinivas TamaskarNo ratings yet
- Research Paper About Asian CuisineDocument8 pagesResearch Paper About Asian Cuisineikofdvbnd100% (1)
- 24 Wlic Index PlusDocument12 pages24 Wlic Index PlusSrinivasan KannanNo ratings yet
- Department of Defense Climate Adaptation PlanDocument32 pagesDepartment of Defense Climate Adaptation PlanCFHeatherNo ratings yet
- Heidenhain TNC 620 CatalogueDocument96 pagesHeidenhain TNC 620 CatalogueDörky LefieuwNo ratings yet
- STANAG 3101eed15Document30 pagesSTANAG 3101eed15Anselmo Alvarez GonzalezNo ratings yet
- 02 Laboratory Exercise 1 TemplateDocument11 pages02 Laboratory Exercise 1 TemplateMarie OsorioNo ratings yet
- Unit 9: Joint Products, Cost Allocation and by Products ContentDocument20 pagesUnit 9: Joint Products, Cost Allocation and by Products Contentዝምታ ተሻለNo ratings yet
- CIBSE Pipe Sizing V2Document13 pagesCIBSE Pipe Sizing V2Sameer UddinNo ratings yet
- Generic Attribute Profile (GATT) Specification - Bluetooth Technology Website PDFDocument3 pagesGeneric Attribute Profile (GATT) Specification - Bluetooth Technology Website PDFAshok Siva Kumar PoojalaNo ratings yet
- Legal Hurdle in Gaming PaymentDocument9 pagesLegal Hurdle in Gaming Paymentanurag kumarNo ratings yet
- Sales IncentiveDocument77 pagesSales Incentivebidiec100% (1)
- Full Ebook of Atkins Physical Chemistry Peter Atkins Online PDF All ChapterDocument69 pagesFull Ebook of Atkins Physical Chemistry Peter Atkins Online PDF All Chapterjessaeynmaei100% (5)
- The Rise and Fall of Levi StraussDocument6 pagesThe Rise and Fall of Levi StraussMark ElbenNo ratings yet
- School Forms Checking ReportDocument10 pagesSchool Forms Checking ReportRODNIE GUBATONNo ratings yet
- Final MKTDocument34 pagesFinal MKTHong Anh VuNo ratings yet
- TranscriptsDocument474 pagesTranscriptsToàn Huỳnh ThanhNo ratings yet
- D-5 Track Maintenance Activities - Part 4Document35 pagesD-5 Track Maintenance Activities - Part 4rajeshengasst89No ratings yet
- Family Case Study On The Billones Family 1Document63 pagesFamily Case Study On The Billones Family 1Ivy Mae DecenaNo ratings yet
- Anti Microbial DrugsDocument18 pagesAnti Microbial Drugseyadballas35No ratings yet
- Lecture 1 General Properties of Viruses 2021Document70 pagesLecture 1 General Properties of Viruses 2021Suresh Krishnani0% (1)
- NTPC Sabbatical SchemeDocument10 pagesNTPC Sabbatical Schemedhanu sreeNo ratings yet
- User - S - Manual Thermometer PDFDocument22 pagesUser - S - Manual Thermometer PDFjuanNo ratings yet