
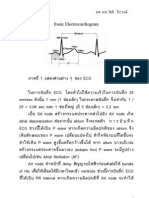
Basic EKG การอ่านคลื่นไฟฟ้าหัวใจเบื้องต้น: interpretation
Basic EKG การอ่านคลื่นไฟฟ้าหัวใจเบื้องต้น: interpretation
You might also like
- SI 115 Survival Guide Complete EditionDocument628 pagesSI 115 Survival Guide Complete Editionตามา รถไฟมา ตามารถไฟ100% (10)
- เฉลยข้อสอบ 4Document40 pagesเฉลยข้อสอบ 4Note Sornkerd100% (9)
- CVPDocument31 pagesCVPKorakot Plongthong100% (1)
- Arrhythmia GADocument6 pagesArrhythmia GANuengburut TiamtanomNo ratings yet
- Basic EKGDocument149 pagesBasic EKGFriska Kirani Nakhwa FirdausiNo ratings yet
- Basic EKGDocument149 pagesBasic EKGFieta Dewi SeptRg100% (3)
- EkgDocument67 pagesEkgkannikaNo ratings yet
- BasicECG by DR ChareanlapDocument29 pagesBasicECG by DR ChareanlapPrukeJIttrathornNo ratings yet
- Basic ECGDocument12 pagesBasic ECGSunudtha SuksamaiNo ratings yet
- Lab Gross of Heart 64, DTDocument30 pagesLab Gross of Heart 64, DTnakarid sinsirinawangNo ratings yet
- Ekg PDFDocument5 pagesEkg PDFKiddyRx LoukkadeNo ratings yet
- Oufoudoydlufouditso 6 W 57 Dipt 85 ADocument5 pagesOufoudoydlufouditso 6 W 57 Dipt 85 AAltiwaNo ratings yet
- Short Notes in CardiologyDocument1,007 pagesShort Notes in CardiologySuchada SangpetchNo ratings yet
- Emailing N Srikanchanawat Internal Medicine 2nd Edition RevisedDocument403 pagesEmailing N Srikanchanawat Internal Medicine 2nd Edition Revisedparames03041512No ratings yet
- cardiac arrhythmia 2020 คลินิกแพทย์ครรชิค-แพทย์สุวิโชติ เชี่ยวชาญDocument161 pagescardiac arrhythmia 2020 คลินิกแพทย์ครรชิค-แพทย์สุวิโชติ เชี่ยวชาญI BNo ratings yet
- เรื่องElectrocardiography ผู้สอน ผศ.พญ. ปณคพร วรรณานนท์Document25 pagesเรื่องElectrocardiography ผู้สอน ผศ.พญ. ปณคพร วรรณานนท์034377101No ratings yet
- แนวทางเวชปฏิบัติในการดูแลผู้ป่วย โรคหัวใจขาดเลือด รพDocument19 pagesแนวทางเวชปฏิบัติในการดูแลผู้ป่วย โรคหัวใจขาดเลือด รพTheerawat NaksanguanNo ratings yet
- Tutor ExternDocument109 pagesTutor ExternVeerapong Vattanavanit75% (8)
- แกะเทป Heart as a Pump & Heart SoundDocument7 pagesแกะเทป Heart as a Pump & Heart SoundHaM_CheesE100% (11)
- 4745-Article Text-6075-1-10-20180912Document7 pages4745-Article Text-6075-1-10-20180912สุภัสสร ภาตุบุตรNo ratings yet
- Internal Medicine TOP SIDocument224 pagesInternal Medicine TOP SIKasidit IntaNo ratings yet
- CE2015 NU Ans PDFDocument303 pagesCE2015 NU Ans PDFIcekung KasamepongtongdeeNo ratings yet
- แกะเทป EKGDocument15 pagesแกะเทป EKGHaM_CheesE100% (10)
- PiPUBM - Surgery&TraumaDocument111 pagesPiPUBM - Surgery&TraumaStaporn KasemsripitakNo ratings yet
- 3 RectifierDocument103 pages3 Rectifierbananabank603No ratings yet
- แกะเทป Electrical Activity of HeartDocument12 pagesแกะเทป Electrical Activity of HeartHaM_CheesE100% (4)
- ระบบหมุนเวียนเลือด circulatory systemDocument21 pagesระบบหมุนเวียนเลือด circulatory systemTeerapat MananitNo ratings yet
- Lect4-4 Monitoring Equipment PDFDocument11 pagesLect4-4 Monitoring Equipment PDFJidapa SEELADEENo ratings yet
- เฉลยข้อสอบ 1-2Document92 pagesเฉลยข้อสอบ 1-2Note Sornkerd89% (9)
- รายงาน การทดลองวิชา ENE 103 Electro technology (Electronics)Document7 pagesรายงาน การทดลองวิชา ENE 103 Electro technology (Electronics)Rinn SinthunavaratNo ratings yet
- EKG For DX ACSDocument57 pagesEKG For DX ACSI BNo ratings yet
- Thai Journal of Nursing Council Vol. 28 No.4 October-December 2013Document12 pagesThai Journal of Nursing Council Vol. 28 No.4 October-December 2013Buneeya BingdolohNo ratings yet
- Anesthetic Consideration in Patients With Cardiac Implantable Electronic Devices (CIED) PDFDocument9 pagesAnesthetic Consideration in Patients With Cardiac Implantable Electronic Devices (CIED) PDFtnim.dsNo ratings yet
- BloodDocument25 pagesBloodknuttorn8179No ratings yet
- แกะเทป Arterial & Venous SystemDocument12 pagesแกะเทป Arterial & Venous SystemHaM_CheesE100% (2)
- Fundamental Chap2 Diode Part2 OkDocument42 pagesFundamental Chap2 Diode Part2 OkThichanon Romsaiyud100% (1)
- Circulation24 6 3Document29 pagesCirculation24 6 3Natcha100% (1)
- Human Body PhysioDocument3 pagesHuman Body PhysioKittiphat AkasriwornNo ratings yet
- โอห์มมิเตอร์กระแสตรงDocument53 pagesโอห์มมิเตอร์กระแสตรงเนติ สุภาพรเหมินทร์No ratings yet
- PCP 452-2565-Ipd-Gr1-Ppt-08022023Document91 pagesPCP 452-2565-Ipd-Gr1-Ppt-08022023Nattapat InhomNo ratings yet
- STEMI.ppt แก้ไข 14 11 53Document117 pagesSTEMI.ppt แก้ไข 14 11 53ชนิชา ธาดาวรภัทร์No ratings yet
- Lab Power ElectronicDocument9 pagesLab Power ElectronicRonnakorn SarikaburtNo ratings yet
- Short Time Fourier Transform (STFT) of ECG SignalDocument16 pagesShort Time Fourier Transform (STFT) of ECG SignalRatchaneekorn Mo-onNo ratings yet
- 46Document58 pages46sujareechansriNo ratings yet
- Ped501 Hyponat NewDocument98 pagesPed501 Hyponat NewMisoo KimNo ratings yet
- Circulatory 2023Document112 pagesCirculatory 2023Lily PimladaNo ratings yet
- AC-DC Converter กลุ่มที่ 2Document17 pagesAC-DC Converter กลุ่มที่ 2Sawatsakorn SirisoNo ratings yet
- Transdusor 01Document10 pagesTransdusor 01nontronicNo ratings yet
- 391 Transformer in ClassDocument39 pages391 Transformer in ClassSmurf 01No ratings yet
- Course Project Elec II Group5Document26 pagesCourse Project Elec II Group5Kittiyaporn GonthongNo ratings yet
- Unit XV Blood Circulatory and Lymphatic m2-1Document53 pagesUnit XV Blood Circulatory and Lymphatic m2-116- Thadchai SaetangNo ratings yet
- ATLSDocument68 pagesATLSPattanop Ngaodulyawat50% (2)
- EM2 Week 1Document2 pagesEM2 Week 1khanitsorn thongchuearNo ratings yet














































Download as pdf or txt
You might also like
- SI 115 Survival Guide Complete EditionDocument628 pagesSI 115 Survival Guide Complete Editionตามา รถไฟมา ตามารถไฟ100% (10)
- เฉลยข้อสอบ 4Document40 pagesเฉลยข้อสอบ 4Note Sornkerd100% (9)
- CVPDocument31 pagesCVPKorakot Plongthong100% (1)
- Arrhythmia GADocument6 pagesArrhythmia GANuengburut TiamtanomNo ratings yet
- Basic EKGDocument149 pagesBasic EKGFriska Kirani Nakhwa FirdausiNo ratings yet
- Basic EKGDocument149 pagesBasic EKGFieta Dewi SeptRg100% (3)
- EkgDocument67 pagesEkgkannikaNo ratings yet
- BasicECG by DR ChareanlapDocument29 pagesBasicECG by DR ChareanlapPrukeJIttrathornNo ratings yet
- Basic ECGDocument12 pagesBasic ECGSunudtha SuksamaiNo ratings yet
- Lab Gross of Heart 64, DTDocument30 pagesLab Gross of Heart 64, DTnakarid sinsirinawangNo ratings yet
- Ekg PDFDocument5 pagesEkg PDFKiddyRx LoukkadeNo ratings yet
- Oufoudoydlufouditso 6 W 57 Dipt 85 ADocument5 pagesOufoudoydlufouditso 6 W 57 Dipt 85 AAltiwaNo ratings yet
- Short Notes in CardiologyDocument1,007 pagesShort Notes in CardiologySuchada SangpetchNo ratings yet
- Emailing N Srikanchanawat Internal Medicine 2nd Edition RevisedDocument403 pagesEmailing N Srikanchanawat Internal Medicine 2nd Edition Revisedparames03041512No ratings yet
- cardiac arrhythmia 2020 คลินิกแพทย์ครรชิค-แพทย์สุวิโชติ เชี่ยวชาญDocument161 pagescardiac arrhythmia 2020 คลินิกแพทย์ครรชิค-แพทย์สุวิโชติ เชี่ยวชาญI BNo ratings yet
- เรื่องElectrocardiography ผู้สอน ผศ.พญ. ปณคพร วรรณานนท์Document25 pagesเรื่องElectrocardiography ผู้สอน ผศ.พญ. ปณคพร วรรณานนท์034377101No ratings yet
- แนวทางเวชปฏิบัติในการดูแลผู้ป่วย โรคหัวใจขาดเลือด รพDocument19 pagesแนวทางเวชปฏิบัติในการดูแลผู้ป่วย โรคหัวใจขาดเลือด รพTheerawat NaksanguanNo ratings yet
- Tutor ExternDocument109 pagesTutor ExternVeerapong Vattanavanit75% (8)
- แกะเทป Heart as a Pump & Heart SoundDocument7 pagesแกะเทป Heart as a Pump & Heart SoundHaM_CheesE100% (11)
- 4745-Article Text-6075-1-10-20180912Document7 pages4745-Article Text-6075-1-10-20180912สุภัสสร ภาตุบุตรNo ratings yet
- Internal Medicine TOP SIDocument224 pagesInternal Medicine TOP SIKasidit IntaNo ratings yet
- CE2015 NU Ans PDFDocument303 pagesCE2015 NU Ans PDFIcekung KasamepongtongdeeNo ratings yet
- แกะเทป EKGDocument15 pagesแกะเทป EKGHaM_CheesE100% (10)
- PiPUBM - Surgery&TraumaDocument111 pagesPiPUBM - Surgery&TraumaStaporn KasemsripitakNo ratings yet
- 3 RectifierDocument103 pages3 Rectifierbananabank603No ratings yet
- แกะเทป Electrical Activity of HeartDocument12 pagesแกะเทป Electrical Activity of HeartHaM_CheesE100% (4)
- ระบบหมุนเวียนเลือด circulatory systemDocument21 pagesระบบหมุนเวียนเลือด circulatory systemTeerapat MananitNo ratings yet
- Lect4-4 Monitoring Equipment PDFDocument11 pagesLect4-4 Monitoring Equipment PDFJidapa SEELADEENo ratings yet
- เฉลยข้อสอบ 1-2Document92 pagesเฉลยข้อสอบ 1-2Note Sornkerd89% (9)
- รายงาน การทดลองวิชา ENE 103 Electro technology (Electronics)Document7 pagesรายงาน การทดลองวิชา ENE 103 Electro technology (Electronics)Rinn SinthunavaratNo ratings yet
- EKG For DX ACSDocument57 pagesEKG For DX ACSI BNo ratings yet
- Thai Journal of Nursing Council Vol. 28 No.4 October-December 2013Document12 pagesThai Journal of Nursing Council Vol. 28 No.4 October-December 2013Buneeya BingdolohNo ratings yet
- Anesthetic Consideration in Patients With Cardiac Implantable Electronic Devices (CIED) PDFDocument9 pagesAnesthetic Consideration in Patients With Cardiac Implantable Electronic Devices (CIED) PDFtnim.dsNo ratings yet
- BloodDocument25 pagesBloodknuttorn8179No ratings yet
- แกะเทป Arterial & Venous SystemDocument12 pagesแกะเทป Arterial & Venous SystemHaM_CheesE100% (2)
- Fundamental Chap2 Diode Part2 OkDocument42 pagesFundamental Chap2 Diode Part2 OkThichanon Romsaiyud100% (1)
- Circulation24 6 3Document29 pagesCirculation24 6 3Natcha100% (1)
- Human Body PhysioDocument3 pagesHuman Body PhysioKittiphat AkasriwornNo ratings yet
- โอห์มมิเตอร์กระแสตรงDocument53 pagesโอห์มมิเตอร์กระแสตรงเนติ สุภาพรเหมินทร์No ratings yet
- PCP 452-2565-Ipd-Gr1-Ppt-08022023Document91 pagesPCP 452-2565-Ipd-Gr1-Ppt-08022023Nattapat InhomNo ratings yet
- STEMI.ppt แก้ไข 14 11 53Document117 pagesSTEMI.ppt แก้ไข 14 11 53ชนิชา ธาดาวรภัทร์No ratings yet
- Lab Power ElectronicDocument9 pagesLab Power ElectronicRonnakorn SarikaburtNo ratings yet
- Short Time Fourier Transform (STFT) of ECG SignalDocument16 pagesShort Time Fourier Transform (STFT) of ECG SignalRatchaneekorn Mo-onNo ratings yet
- 46Document58 pages46sujareechansriNo ratings yet
- Ped501 Hyponat NewDocument98 pagesPed501 Hyponat NewMisoo KimNo ratings yet
- Circulatory 2023Document112 pagesCirculatory 2023Lily PimladaNo ratings yet
- AC-DC Converter กลุ่มที่ 2Document17 pagesAC-DC Converter กลุ่มที่ 2Sawatsakorn SirisoNo ratings yet
- Transdusor 01Document10 pagesTransdusor 01nontronicNo ratings yet
- 391 Transformer in ClassDocument39 pages391 Transformer in ClassSmurf 01No ratings yet
- Course Project Elec II Group5Document26 pagesCourse Project Elec II Group5Kittiyaporn GonthongNo ratings yet
- Unit XV Blood Circulatory and Lymphatic m2-1Document53 pagesUnit XV Blood Circulatory and Lymphatic m2-116- Thadchai SaetangNo ratings yet
- ATLSDocument68 pagesATLSPattanop Ngaodulyawat50% (2)
- EM2 Week 1Document2 pagesEM2 Week 1khanitsorn thongchuearNo ratings yet