Download as docx, pdf, or txt
You might also like
- Soldering Risk Assessment 2018 PDFDocument5 pagesSoldering Risk Assessment 2018 PDFbubele pamlaNo ratings yet
- Tracheostomy: Presented By: Barte, Hannah Aida D. Balamurugan, RameebhaDocument21 pagesTracheostomy: Presented By: Barte, Hannah Aida D. Balamurugan, RameebhaThakoon Tts100% (1)
- Intercostal DrainDocument44 pagesIntercostal Drainvamshidh100% (1)
- Intubation: by Joan SinghDocument17 pagesIntubation: by Joan SinghJoan Singh100% (1)
- How To Do Holotropic BreathworkDocument2 pagesHow To Do Holotropic Breathworkcaiverzi1100% (7)
- Pharmacotherapy of CoughDocument51 pagesPharmacotherapy of CoughIqra Butt100% (3)
- Tracheostomy CareDocument22 pagesTracheostomy Carehakky gamyNo ratings yet
- Tracheostomy: ENT Department DMC & Hospital Ludhiana PunjabDocument46 pagesTracheostomy: ENT Department DMC & Hospital Ludhiana PunjabVikrant MittalNo ratings yet
- Tracheostomy Care (Done)Document53 pagesTracheostomy Care (Done)martinNo ratings yet
- Tracheostomy Care: Presented by Sital B. Sharma M SC Nursing Student College of Nursing. N.B.M.C.HDocument74 pagesTracheostomy Care: Presented by Sital B. Sharma M SC Nursing Student College of Nursing. N.B.M.C.HShetal Sharma100% (1)
- Tracheostomy SlidesDocument24 pagesTracheostomy SlidesMohammed AdamNo ratings yet
- Assignment ON Tracheostom Y Care: Submitted To: Submitted byDocument5 pagesAssignment ON Tracheostom Y Care: Submitted To: Submitted byAnanthibala100% (1)
- Care of Clients With Chest TubeDocument55 pagesCare of Clients With Chest TubeMarc Andreo MalalaNo ratings yet
- TRACHEOSTOMYDocument4 pagesTRACHEOSTOMYPrecious BlessingNo ratings yet
- ET TubeDocument4 pagesET TuberumasadraunaNo ratings yet
- Chap.30 Med SurgDocument4 pagesChap.30 Med SurgSheldon SloanNo ratings yet
- TRACHEOSTOMYDocument109 pagesTRACHEOSTOMYJayson RN92% (12)
- SuctioningDocument15 pagesSuctioningAngie MandeoyaNo ratings yet
- Final TracheostomyDocument6 pagesFinal TracheostomychandhomepcNo ratings yet
- Tracheostomy CareDocument37 pagesTracheostomy CareCharlene de CastroNo ratings yet
- TracheostomyDocument4 pagesTracheostomyNapieh Bulalaque PolisticoNo ratings yet
- Nasogastric Feeding TubeDocument7 pagesNasogastric Feeding Tubepatrayati90No ratings yet
- Tracheostomy SuctioningDocument59 pagesTracheostomy SuctioningMaan LapitanNo ratings yet
- TracheostomyDocument56 pagesTracheostomyRoshana MallawaarachchiNo ratings yet
- College of Nursing: (Dalubhasaan NG Narsing)Document10 pagesCollege of Nursing: (Dalubhasaan NG Narsing)Kimmy NgNo ratings yet
- Issaiah Nicolle L. Cecilia 3 BSN - ADocument6 pagesIssaiah Nicolle L. Cecilia 3 BSN - AIssaiah Nicolle CeciliaNo ratings yet
- AIRWAY-MANAGEMENT-SUCTIONING NotesDocument6 pagesAIRWAY-MANAGEMENT-SUCTIONING NotesYasser UlodNo ratings yet
- Extubation After Difficult IntubationDocument3 pagesExtubation After Difficult Intubationramanrajesh83No ratings yet
- Tracheostomy Care GuidelinesDocument15 pagesTracheostomy Care Guidelinesnurseuragon92% (25)
- Safe SuctioningDocument31 pagesSafe SuctioningKatrina Ponce100% (2)
- Endotracheal Intubation: By: AizaDocument29 pagesEndotracheal Intubation: By: AizaAiza Apelada-NievaNo ratings yet
- MedSurg NotesDocument57 pagesMedSurg NotesCHRISTOFER CORONADONo ratings yet
- Care of The Patient With A TracheostomyDocument25 pagesCare of The Patient With A TracheostomyBinu JoshvaNo ratings yet
- TracheostomyDocument32 pagesTracheostomydr Mohammed100% (1)
- Issaiah Nicolle L. Cecilia 3 BSN - ADocument14 pagesIssaiah Nicolle L. Cecilia 3 BSN - AIssaiah Nicolle CeciliaNo ratings yet
- TracheostomyDocument3 pagesTracheostomySarah Elizabeth WalkerNo ratings yet
- Tracheal Tubes and Prevention of VAPDocument23 pagesTracheal Tubes and Prevention of VAPعزالدين الزوقريNo ratings yet
- Tracheostomy Care: University of Babylon Faculty of NursingDocument24 pagesTracheostomy Care: University of Babylon Faculty of NursingmelaniaNo ratings yet
- Tracheostomy Care & WeanDocument33 pagesTracheostomy Care & WeanShiraz QamilNo ratings yet
- PRECAUTIONS FOR-WPS OfficeDocument5 pagesPRECAUTIONS FOR-WPS Officemkoboni23No ratings yet
- Tracheostomy CareDocument26 pagesTracheostomy CareMicaNo ratings yet
- Chest Drain ManagementDocument7 pagesChest Drain ManagementanuzNo ratings yet
- Tracheostomy: Done By: Sami FreijyDocument14 pagesTracheostomy: Done By: Sami FreijySami FreijyNo ratings yet
- Oxygen Administration SystemDocument45 pagesOxygen Administration SystemNamita Jadhao100% (1)
- SuctioningDocument24 pagesSuctioningzhaimeangirlNo ratings yet
- Suction Endotracheal V P StgeorgeDocument3 pagesSuction Endotracheal V P StgeorgeElaine Iris AbastaNo ratings yet
- Respiratory: Anatomy + PhysiologyDocument58 pagesRespiratory: Anatomy + Physiologydelrosariodenisejoy05No ratings yet
- Care During ECT Procedure: Submitted To: Priyanka Madam Submitted By: Ujjwal SadanshivDocument4 pagesCare During ECT Procedure: Submitted To: Priyanka Madam Submitted By: Ujjwal SadanshivUjjwal SadanshivNo ratings yet
- Tracheostomy CareDocument45 pagesTracheostomy Caredrnasir31No ratings yet
- CH 3 Maintenance and Care For Artificial AirwayDocument125 pagesCH 3 Maintenance and Care For Artificial AirwayMaherNo ratings yet
- Tracheostomy CareDocument44 pagesTracheostomy CareJharaNo ratings yet
- Assissting IntubationDocument17 pagesAssissting IntubationTriciaNo ratings yet
- Airway ManagementDocument16 pagesAirway ManagementSuganthi ParthibanNo ratings yet
- Et CareDocument15 pagesEt CarePaulo GarciaNo ratings yet
- Tracheostomy Tube CareDocument12 pagesTracheostomy Tube CareydtrgnNo ratings yet
- TRACHEOSTOMYDocument2 pagesTRACHEOSTOMY3C SAVELLA, Glaiza Marie RNo ratings yet
- Tracheostomy Care SkillsDocument8 pagesTracheostomy Care Skillshoangt2002No ratings yet
- Ramon Magsaysay Memorial Medical Center, Inc.: University of The EastDocument7 pagesRamon Magsaysay Memorial Medical Center, Inc.: University of The EastHANNAH MICOLE GAERLANNo ratings yet
- Primary Survey RealDocument21 pagesPrimary Survey RealLaraib KanwalNo ratings yet
- Central Line Removal ProtocolDocument1 pageCentral Line Removal Protocolmathurarun2000No ratings yet
- Different in the therapy of pressure negtotheeva single-useFrom EverandDifferent in the therapy of pressure negtotheeva single-useNo ratings yet
- Anesthesia in Thoracic Surgery: Changes of ParadigmsFrom EverandAnesthesia in Thoracic Surgery: Changes of ParadigmsManuel Granell GilNo ratings yet
- Drugs Used in Cardiac EmergenciesDocument18 pagesDrugs Used in Cardiac Emergencieshakky gamyNo ratings yet
- Bedside Presentation On CADDocument40 pagesBedside Presentation On CADhakky gamyNo ratings yet
- Pathogenesis of AtherosclerosisDocument21 pagesPathogenesis of Atherosclerosishakky gamyNo ratings yet
- ChemistryDocument51 pagesChemistryhakky gamyNo ratings yet
- Document 3Document2 pagesDocument 3hakky gamyNo ratings yet
- 198-GR - GRADE - 9-SB - biology-TP - notes-ANIMAL NUTRITION & Biological MoleculesDocument8 pages198-GR - GRADE - 9-SB - biology-TP - notes-ANIMAL NUTRITION & Biological Moleculeshakky gamyNo ratings yet
- Optical Neuritis: By: Antia Ayudika Supervisor M. Diana Rahim, MDDocument9 pagesOptical Neuritis: By: Antia Ayudika Supervisor M. Diana Rahim, MDdianarahimmNo ratings yet
- Intelli SyncDocument50 pagesIntelli SyncMadyline KatipanaNo ratings yet
- Acute Respiratory FailureDocument25 pagesAcute Respiratory FailurejohnleeeNo ratings yet
- Sulfuric Acid, 96% W/W: Safety Data SheetDocument8 pagesSulfuric Acid, 96% W/W: Safety Data SheetLindi PraditaNo ratings yet
- Sheetrock All Purpose Joint Compound Submittal J1969Document2 pagesSheetrock All Purpose Joint Compound Submittal J1969Eva MedinaNo ratings yet
- 4 - Batteries Material Safety Data SheetDocument6 pages4 - Batteries Material Safety Data Sheethafed baccoucheNo ratings yet
- Asthma Ineffective Airway ClearanceDocument2 pagesAsthma Ineffective Airway ClearanceEdmr SlzarNo ratings yet
- Seminar On Chronic Obstructive Pulmonary Disease (Copd)Document40 pagesSeminar On Chronic Obstructive Pulmonary Disease (Copd)Soniya Nakka100% (1)
- Indonesia Covid Cases - Google SearchDocument1 pageIndonesia Covid Cases - Google Searchche_c812125No ratings yet
- 118 A Chapter 2 - Responses To Altered Ventilatory Function (Edited) Handout #3 (Sir Marvin)Document14 pages118 A Chapter 2 - Responses To Altered Ventilatory Function (Edited) Handout #3 (Sir Marvin)Joanna TaylanNo ratings yet
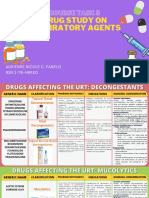
- Course Task 8 Drug Study On Respiratory AgentsDocument23 pagesCourse Task 8 Drug Study On Respiratory AgentsAdrienne Nicole PaneloNo ratings yet
- CPAPDocument5 pagesCPAPraul gutierrezNo ratings yet
- MXR Flowmeters Users Manual FM-286Document20 pagesMXR Flowmeters Users Manual FM-286Μαριτίνα ΑλεξίουNo ratings yet
- Basics Mechanical VentilationDocument51 pagesBasics Mechanical VentilationademNo ratings yet
- Taro 30 DP 40: Safety Data SheetDocument6 pagesTaro 30 DP 40: Safety Data SheetHassan KhalifeNo ratings yet
- Material Safety Data SheetDocument5 pagesMaterial Safety Data SheetMila SabriNo ratings yet
- PPT Skenario A - G6 - Blok 14Document66 pagesPPT Skenario A - G6 - Blok 14Ellysa CarolinnNo ratings yet
- Product and Company Identification: 1st Street Oven & Grill Cleaner Safety Data SheetDocument6 pagesProduct and Company Identification: 1st Street Oven & Grill Cleaner Safety Data Sheeteng4008No ratings yet
- Langmore 1988 Fiberoptic Endoscopic Examination of Swallowing SafetyDocument4 pagesLangmore 1988 Fiberoptic Endoscopic Examination of Swallowing SafetyDesiré MagalhãesNo ratings yet
- Circulatory and Respiratory ReviewDocument5 pagesCirculatory and Respiratory ReviewTristan PereyNo ratings yet
- Dyspnea Grading ScaleDocument5 pagesDyspnea Grading ScaleSartini Roma Dame NainggolanNo ratings yet
- Australasian Anaesthesia 2015Document107 pagesAustralasian Anaesthesia 2015Sean SmythNo ratings yet
- T2410222 - Activax CleanerDocument5 pagesT2410222 - Activax CleanerFreaknielllNo ratings yet
- PH Pco2 Pao2 Hco3 Spo2: Mode Description Pros Cons Major Settings / ExampleDocument1 pagePH Pco2 Pao2 Hco3 Spo2: Mode Description Pros Cons Major Settings / ExampleQasim AwanNo ratings yet
- Tracheostomy Care GuidelinesDocument15 pagesTracheostomy Care Guidelinesnurseuragon92% (25)
- Assessment and Initial Management Trauma PatientDocument69 pagesAssessment and Initial Management Trauma PatientdrpagrawNo ratings yet
- BLS Study Guide and PretestDocument47 pagesBLS Study Guide and PretestRicha AbcedeNo ratings yet