
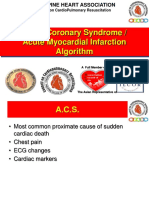
Chest Pain
Chest Pain
You might also like
- Algorithm-ACLS ACS 200806 1Document1 pageAlgorithm-ACLS ACS 200806 1Kavya Shree100% (1)
- High Yield Cardiology Internal Medicine Shelf PDFDocument44 pagesHigh Yield Cardiology Internal Medicine Shelf PDFsaja fuadNo ratings yet
- Algorithm 1: Initial Evaluation and Management: Symptoms of Possible ACSDocument6 pagesAlgorithm 1: Initial Evaluation and Management: Symptoms of Possible ACSNenyNo ratings yet
- CVS1 - K25 - Cardiac EmergencyDocument34 pagesCVS1 - K25 - Cardiac EmergencyAdmin neuro-usu.idNo ratings yet
- Acute Coronary Syndrome: An Essential & Practical ApproachDocument35 pagesAcute Coronary Syndrome: An Essential & Practical ApproachGinawidiyastutiNo ratings yet
- ACLS ACS Algorithm NewDocument3 pagesACLS ACS Algorithm Newsambo100% (1)
- Acute Coronary SyndromeDocument5 pagesAcute Coronary Syndromem3d1k100% (1)
- Acute Coronary Syndrome: Patsadee Nachom MDDocument58 pagesAcute Coronary Syndrome: Patsadee Nachom MDRachapon OngwibunwongNo ratings yet
- Acute Coronary Syndrome / Acute Myocardial Infarction AlgorithmDocument37 pagesAcute Coronary Syndrome / Acute Myocardial Infarction Algorithmjitendra magarNo ratings yet
- Acs CCS 2021 KLDocument52 pagesAcs CCS 2021 KLPitchya WangmeesriNo ratings yet
- ST-Elevation Myocardial Infarction (Stemi) : Present byDocument29 pagesST-Elevation Myocardial Infarction (Stemi) : Present byReema AlamriNo ratings yet
- Prescribing in Chest PainDocument4 pagesPrescribing in Chest PainYY_1992No ratings yet
- Emd1-K22-Cardiac EmergencyDocument49 pagesEmd1-K22-Cardiac EmergencyAnanta GintingNo ratings yet
- Nstemi 3MBDocument69 pagesNstemi 3MBDNo ratings yet
- ACS Final DraftDocument33 pagesACS Final Draftomcm17006No ratings yet
- Acute Coronary Syndrome EditedDocument38 pagesAcute Coronary Syndrome EditedSurgicalgownNo ratings yet
- Acute Coronary SyndromeDocument5 pagesAcute Coronary Syndromecotten joeNo ratings yet
- ACS BikoDocument18 pagesACS BikoDanissa Fidia PuteriNo ratings yet
- Management of ArrhythmiasDocument4 pagesManagement of ArrhythmiasAray Al-AfiqahNo ratings yet
- ParulDocument7 pagesParulПарул КатіярNo ratings yet
- Acute Coronary SyndromeDocument52 pagesAcute Coronary Syndromeindra muhammadNo ratings yet
- Kegawatan Jantung - MeDocument41 pagesKegawatan Jantung - MeNam Min BinNo ratings yet
- IM CASE RTR - Myocardial InfarctionDocument47 pagesIM CASE RTR - Myocardial InfarctionTrisNo ratings yet
- ACS - Dr. BennyDocument45 pagesACS - Dr. Bennyutari rahmaNo ratings yet
- Acute Coronary Syndrome / Acute Myocardial Infarction AlgorithmDocument37 pagesAcute Coronary Syndrome / Acute Myocardial Infarction AlgorithmHan OWNo ratings yet
- Clinical Pathway StrokeDocument8 pagesClinical Pathway StrokedjizhieeNo ratings yet
- Menu Dieet MayooDocument50 pagesMenu Dieet MayooariefsuwarniNo ratings yet
- 5 ACS Pathway NT IltonDocument48 pages5 ACS Pathway NT IltonAlief AkbarNo ratings yet
- Acute Coronary Syndrome: Hasbiyetil HusniDocument40 pagesAcute Coronary Syndrome: Hasbiyetil HusnipraktekdrfadelNo ratings yet
- Myocardial InfarctionDocument1 pageMyocardial InfarctionjljoioiuNo ratings yet
- Acute Coronay Syndrome - BACCDocument72 pagesAcute Coronay Syndrome - BACCYeyen Devyanti HandokoNo ratings yet
- Sindroma Koroner Akut: World Heart Day 29 SEPTEMBER 2021Document68 pagesSindroma Koroner Akut: World Heart Day 29 SEPTEMBER 2021Dafhina Store100% (1)
- 6 - Fahad Class 6 Cardiac AnesthesiaDocument18 pages6 - Fahad Class 6 Cardiac AnesthesiaOne ClickNo ratings yet
- Troponin PathwayDocument1 pageTroponin PathwayAllana AngelesNo ratings yet
- Acute Coronary Syndrome - YMDocument64 pagesAcute Coronary Syndrome - YMNirwanaNo ratings yet
- Cardiopulmonary Resuscitation & Emergency Cardiovascular CareDocument32 pagesCardiopulmonary Resuscitation & Emergency Cardiovascular CareMohamad FikrieNo ratings yet
- Cardiology BookletDocument30 pagesCardiology Bookletali.khanfariplsNo ratings yet
- Medicine: Management of Patients With UA/NSTEMIDocument2 pagesMedicine: Management of Patients With UA/NSTEMIapi-3829364No ratings yet
- LYSISDocument3 pagesLYSISjenitNo ratings yet
- MTB Cardiology NotesDocument7 pagesMTB Cardiology Noteskabal321No ratings yet
- ACS (Dr. Thamrin 2015)Document43 pagesACS (Dr. Thamrin 2015)Budianto Aj Ganteng DeweNo ratings yet
- MTB Cardiology NotesDocument11 pagesMTB Cardiology Noteskabal321No ratings yet
- Acute Coronary Syndrome: by Ho NisaDocument58 pagesAcute Coronary Syndrome: by Ho NisaShre RanjithamNo ratings yet
- Pemicu 6 KGD DeniseDocument95 pagesPemicu 6 KGD DeniseVincent VandestyoNo ratings yet
- Acute Choronary SyndromeDocument7 pagesAcute Choronary SyndromeSafana NazeerNo ratings yet
- Cerebrovascular Accidents: Stroke Versus TIADocument19 pagesCerebrovascular Accidents: Stroke Versus TIASagar ShahNo ratings yet
- ACS Management in Pandemic EraDocument56 pagesACS Management in Pandemic EraFatmawati nersNo ratings yet
- CHC-PC-0033: Procedure Number Version NosDocument7 pagesCHC-PC-0033: Procedure Number Version NosQari Ramadhan AminNo ratings yet
- ACS (Dr. Thamrin 2015)Document43 pagesACS (Dr. Thamrin 2015)ok sogatenNo ratings yet
- Peri Arrest ArrhythmiasDocument40 pagesPeri Arrest ArrhythmiasDestiAriyaniNo ratings yet
- StrokeDocument7 pagesStrokeAhmed AdelNo ratings yet
- Ventura County Medical Center: Mi Thrombolysis, Management ofDocument3 pagesVentura County Medical Center: Mi Thrombolysis, Management ofblackcat657No ratings yet
- St-Segment Elevation Myocardial Infarction: PGI Barrantes, Lloyd DanielDocument28 pagesSt-Segment Elevation Myocardial Infarction: PGI Barrantes, Lloyd DanielLloyd Daniel BarrantesNo ratings yet
- Acs With New Stemi GuidelineDocument35 pagesAcs With New Stemi Guidelinematmin07No ratings yet
- NSTEMIDocument29 pagesNSTEMIGeanina Creanga100% (1)
- Stroke Inclusion Exclusion StrokeDocument1 pageStroke Inclusion Exclusion Strokecdeepak71No ratings yet
- Pearls of MRCP Part 2 PastestDocument111 pagesPearls of MRCP Part 2 PastestS TNo ratings yet
- EKG StripsDocument10 pagesEKG StripsSaidel ElizondoNo ratings yet
- NCP Seizure FinalDocument4 pagesNCP Seizure FinalLyrechel de GuzmanNo ratings yet
- Clodinafop - Msds PDFDocument6 pagesClodinafop - Msds PDFMishra KewalNo ratings yet
- Contemporary Orthodontics, 5th Ed: Book ReviewDocument1 pageContemporary Orthodontics, 5th Ed: Book ReviewPaula Diaz100% (1)
- Sample Essay For High School StudentsDocument4 pagesSample Essay For High School StudentshtzmxoaegNo ratings yet
- The Analysis of Pharmaceutical MarketDocument10 pagesThe Analysis of Pharmaceutical MarketAnamaria BejenariuNo ratings yet
- iRECIST: Guidelines For Response Criteria For Use in Trials Testing Immunotherapeutics AuthorsDocument30 pagesiRECIST: Guidelines For Response Criteria For Use in Trials Testing Immunotherapeutics AuthorsNguyenthanh DuongNo ratings yet
- Disaster Drill JournalDocument3 pagesDisaster Drill Journalapi-508765756No ratings yet
- CXC Social Studies Sba 2023Document27 pagesCXC Social Studies Sba 2023David DillonNo ratings yet
- Acute Management of Pulmonary Embolism - American College of CardiologyDocument22 pagesAcute Management of Pulmonary Embolism - American College of CardiologyRaja GopalNo ratings yet
- NCPDocument10 pagesNCPRobin HaliliNo ratings yet
- Boost Your PA ProtectionDocument22 pagesBoost Your PA ProtectionLogen TiranNo ratings yet
- Acne Blackheads Pimple Zits MedlinePlusgrzkjxirmtDocument2 pagesAcne Blackheads Pimple Zits MedlinePlusgrzkjxirmtdollarcanvas0No ratings yet
- "Take Off Patient/ Operan Jaga": Tugas Bahasa InggrisDocument3 pages"Take Off Patient/ Operan Jaga": Tugas Bahasa InggrisKurnia anggrainiNo ratings yet
- Clinical Goals For Placement Louisa Oduro Animapauh Hsns 206 220183967Document3 pagesClinical Goals For Placement Louisa Oduro Animapauh Hsns 206 220183967api-426629371No ratings yet
- SHE List DocumentDocument1 pageSHE List DocumentMunajamNo ratings yet
- Peripheral NeuropathyDocument30 pagesPeripheral NeuropathyLyn LynNo ratings yet
- W9 Teori Akuntansi RS ASPDocument4 pagesW9 Teori Akuntansi RS ASPJessicaNo ratings yet
- BDRRM Polo Action PlanDocument3 pagesBDRRM Polo Action Planmicah bitantosNo ratings yet
- INTUSSUSCEPTIONDocument1 pageINTUSSUSCEPTIONAezyreal Anne MirallesNo ratings yet
- IJP Mhca SupplementDocument7 pagesIJP Mhca Supplementgion.nandNo ratings yet
- Vitamin D SupplementsDocument11 pagesVitamin D SupplementsPetra JobovaNo ratings yet
- Job Stress Work Performance With CommentssssDocument37 pagesJob Stress Work Performance With CommentssssAmen MartzNo ratings yet
- DR ScrapbookDocument8 pagesDR Scrapbookcrenz23_shaniyha15No ratings yet
- 89 391 Eec PDFDocument8 pages89 391 Eec PDFBasara MladenNo ratings yet
- We Are What We EatDocument2 pagesWe Are What We EatAlex MgebrishviliNo ratings yet
- Effects of Alcoholism To The BehaviourDocument4 pagesEffects of Alcoholism To The BehaviourJoylyn PerezNo ratings yet
- TractionDocument11 pagesTractionDenalyn Ann TormoNo ratings yet
- Alzheimer Lengkappppp PDFDocument8 pagesAlzheimer Lengkappppp PDFyulan sulemanNo ratings yet
- Hse Induction: KYK Analysis of Potentially Hazardous Area (JSA)Document1 pageHse Induction: KYK Analysis of Potentially Hazardous Area (JSA)teman k3No ratings yet
- Islamic Integrated Cognitive Behavior Therapy: A Shari'ah-Compliant Intervention For Muslims With DepressionDocument10 pagesIslamic Integrated Cognitive Behavior Therapy: A Shari'ah-Compliant Intervention For Muslims With DepressionHANISAH BINTI ABDUL RAHMAN MIC173019No ratings yet
























































































Download as pdf or txt
You might also like
- Algorithm-ACLS ACS 200806 1Document1 pageAlgorithm-ACLS ACS 200806 1Kavya Shree100% (1)
- High Yield Cardiology Internal Medicine Shelf PDFDocument44 pagesHigh Yield Cardiology Internal Medicine Shelf PDFsaja fuadNo ratings yet
- Algorithm 1: Initial Evaluation and Management: Symptoms of Possible ACSDocument6 pagesAlgorithm 1: Initial Evaluation and Management: Symptoms of Possible ACSNenyNo ratings yet
- CVS1 - K25 - Cardiac EmergencyDocument34 pagesCVS1 - K25 - Cardiac EmergencyAdmin neuro-usu.idNo ratings yet
- Acute Coronary Syndrome: An Essential & Practical ApproachDocument35 pagesAcute Coronary Syndrome: An Essential & Practical ApproachGinawidiyastutiNo ratings yet
- ACLS ACS Algorithm NewDocument3 pagesACLS ACS Algorithm Newsambo100% (1)
- Acute Coronary SyndromeDocument5 pagesAcute Coronary Syndromem3d1k100% (1)
- Acute Coronary Syndrome: Patsadee Nachom MDDocument58 pagesAcute Coronary Syndrome: Patsadee Nachom MDRachapon OngwibunwongNo ratings yet
- Acute Coronary Syndrome / Acute Myocardial Infarction AlgorithmDocument37 pagesAcute Coronary Syndrome / Acute Myocardial Infarction Algorithmjitendra magarNo ratings yet
- Acs CCS 2021 KLDocument52 pagesAcs CCS 2021 KLPitchya WangmeesriNo ratings yet
- ST-Elevation Myocardial Infarction (Stemi) : Present byDocument29 pagesST-Elevation Myocardial Infarction (Stemi) : Present byReema AlamriNo ratings yet
- Prescribing in Chest PainDocument4 pagesPrescribing in Chest PainYY_1992No ratings yet
- Emd1-K22-Cardiac EmergencyDocument49 pagesEmd1-K22-Cardiac EmergencyAnanta GintingNo ratings yet
- Nstemi 3MBDocument69 pagesNstemi 3MBDNo ratings yet
- ACS Final DraftDocument33 pagesACS Final Draftomcm17006No ratings yet
- Acute Coronary Syndrome EditedDocument38 pagesAcute Coronary Syndrome EditedSurgicalgownNo ratings yet
- Acute Coronary SyndromeDocument5 pagesAcute Coronary Syndromecotten joeNo ratings yet
- ACS BikoDocument18 pagesACS BikoDanissa Fidia PuteriNo ratings yet
- Management of ArrhythmiasDocument4 pagesManagement of ArrhythmiasAray Al-AfiqahNo ratings yet
- ParulDocument7 pagesParulПарул КатіярNo ratings yet
- Acute Coronary SyndromeDocument52 pagesAcute Coronary Syndromeindra muhammadNo ratings yet
- Kegawatan Jantung - MeDocument41 pagesKegawatan Jantung - MeNam Min BinNo ratings yet
- IM CASE RTR - Myocardial InfarctionDocument47 pagesIM CASE RTR - Myocardial InfarctionTrisNo ratings yet
- ACS - Dr. BennyDocument45 pagesACS - Dr. Bennyutari rahmaNo ratings yet
- Acute Coronary Syndrome / Acute Myocardial Infarction AlgorithmDocument37 pagesAcute Coronary Syndrome / Acute Myocardial Infarction AlgorithmHan OWNo ratings yet
- Clinical Pathway StrokeDocument8 pagesClinical Pathway StrokedjizhieeNo ratings yet
- Menu Dieet MayooDocument50 pagesMenu Dieet MayooariefsuwarniNo ratings yet
- 5 ACS Pathway NT IltonDocument48 pages5 ACS Pathway NT IltonAlief AkbarNo ratings yet
- Acute Coronary Syndrome: Hasbiyetil HusniDocument40 pagesAcute Coronary Syndrome: Hasbiyetil HusnipraktekdrfadelNo ratings yet
- Myocardial InfarctionDocument1 pageMyocardial InfarctionjljoioiuNo ratings yet
- Acute Coronay Syndrome - BACCDocument72 pagesAcute Coronay Syndrome - BACCYeyen Devyanti HandokoNo ratings yet
- Sindroma Koroner Akut: World Heart Day 29 SEPTEMBER 2021Document68 pagesSindroma Koroner Akut: World Heart Day 29 SEPTEMBER 2021Dafhina Store100% (1)
- 6 - Fahad Class 6 Cardiac AnesthesiaDocument18 pages6 - Fahad Class 6 Cardiac AnesthesiaOne ClickNo ratings yet
- Troponin PathwayDocument1 pageTroponin PathwayAllana AngelesNo ratings yet
- Acute Coronary Syndrome - YMDocument64 pagesAcute Coronary Syndrome - YMNirwanaNo ratings yet
- Cardiopulmonary Resuscitation & Emergency Cardiovascular CareDocument32 pagesCardiopulmonary Resuscitation & Emergency Cardiovascular CareMohamad FikrieNo ratings yet
- Cardiology BookletDocument30 pagesCardiology Bookletali.khanfariplsNo ratings yet
- Medicine: Management of Patients With UA/NSTEMIDocument2 pagesMedicine: Management of Patients With UA/NSTEMIapi-3829364No ratings yet
- LYSISDocument3 pagesLYSISjenitNo ratings yet
- MTB Cardiology NotesDocument7 pagesMTB Cardiology Noteskabal321No ratings yet
- ACS (Dr. Thamrin 2015)Document43 pagesACS (Dr. Thamrin 2015)Budianto Aj Ganteng DeweNo ratings yet
- MTB Cardiology NotesDocument11 pagesMTB Cardiology Noteskabal321No ratings yet
- Acute Coronary Syndrome: by Ho NisaDocument58 pagesAcute Coronary Syndrome: by Ho NisaShre RanjithamNo ratings yet
- Pemicu 6 KGD DeniseDocument95 pagesPemicu 6 KGD DeniseVincent VandestyoNo ratings yet
- Acute Choronary SyndromeDocument7 pagesAcute Choronary SyndromeSafana NazeerNo ratings yet
- Cerebrovascular Accidents: Stroke Versus TIADocument19 pagesCerebrovascular Accidents: Stroke Versus TIASagar ShahNo ratings yet
- ACS Management in Pandemic EraDocument56 pagesACS Management in Pandemic EraFatmawati nersNo ratings yet
- CHC-PC-0033: Procedure Number Version NosDocument7 pagesCHC-PC-0033: Procedure Number Version NosQari Ramadhan AminNo ratings yet
- ACS (Dr. Thamrin 2015)Document43 pagesACS (Dr. Thamrin 2015)ok sogatenNo ratings yet
- Peri Arrest ArrhythmiasDocument40 pagesPeri Arrest ArrhythmiasDestiAriyaniNo ratings yet
- StrokeDocument7 pagesStrokeAhmed AdelNo ratings yet
- Ventura County Medical Center: Mi Thrombolysis, Management ofDocument3 pagesVentura County Medical Center: Mi Thrombolysis, Management ofblackcat657No ratings yet
- St-Segment Elevation Myocardial Infarction: PGI Barrantes, Lloyd DanielDocument28 pagesSt-Segment Elevation Myocardial Infarction: PGI Barrantes, Lloyd DanielLloyd Daniel BarrantesNo ratings yet
- Acs With New Stemi GuidelineDocument35 pagesAcs With New Stemi Guidelinematmin07No ratings yet
- NSTEMIDocument29 pagesNSTEMIGeanina Creanga100% (1)
- Stroke Inclusion Exclusion StrokeDocument1 pageStroke Inclusion Exclusion Strokecdeepak71No ratings yet
- Pearls of MRCP Part 2 PastestDocument111 pagesPearls of MRCP Part 2 PastestS TNo ratings yet
- EKG StripsDocument10 pagesEKG StripsSaidel ElizondoNo ratings yet
- NCP Seizure FinalDocument4 pagesNCP Seizure FinalLyrechel de GuzmanNo ratings yet
- Clodinafop - Msds PDFDocument6 pagesClodinafop - Msds PDFMishra KewalNo ratings yet
- Contemporary Orthodontics, 5th Ed: Book ReviewDocument1 pageContemporary Orthodontics, 5th Ed: Book ReviewPaula Diaz100% (1)
- Sample Essay For High School StudentsDocument4 pagesSample Essay For High School StudentshtzmxoaegNo ratings yet
- The Analysis of Pharmaceutical MarketDocument10 pagesThe Analysis of Pharmaceutical MarketAnamaria BejenariuNo ratings yet
- iRECIST: Guidelines For Response Criteria For Use in Trials Testing Immunotherapeutics AuthorsDocument30 pagesiRECIST: Guidelines For Response Criteria For Use in Trials Testing Immunotherapeutics AuthorsNguyenthanh DuongNo ratings yet
- Disaster Drill JournalDocument3 pagesDisaster Drill Journalapi-508765756No ratings yet
- CXC Social Studies Sba 2023Document27 pagesCXC Social Studies Sba 2023David DillonNo ratings yet
- Acute Management of Pulmonary Embolism - American College of CardiologyDocument22 pagesAcute Management of Pulmonary Embolism - American College of CardiologyRaja GopalNo ratings yet
- NCPDocument10 pagesNCPRobin HaliliNo ratings yet
- Boost Your PA ProtectionDocument22 pagesBoost Your PA ProtectionLogen TiranNo ratings yet
- Acne Blackheads Pimple Zits MedlinePlusgrzkjxirmtDocument2 pagesAcne Blackheads Pimple Zits MedlinePlusgrzkjxirmtdollarcanvas0No ratings yet
- "Take Off Patient/ Operan Jaga": Tugas Bahasa InggrisDocument3 pages"Take Off Patient/ Operan Jaga": Tugas Bahasa InggrisKurnia anggrainiNo ratings yet
- Clinical Goals For Placement Louisa Oduro Animapauh Hsns 206 220183967Document3 pagesClinical Goals For Placement Louisa Oduro Animapauh Hsns 206 220183967api-426629371No ratings yet
- SHE List DocumentDocument1 pageSHE List DocumentMunajamNo ratings yet
- Peripheral NeuropathyDocument30 pagesPeripheral NeuropathyLyn LynNo ratings yet
- W9 Teori Akuntansi RS ASPDocument4 pagesW9 Teori Akuntansi RS ASPJessicaNo ratings yet
- BDRRM Polo Action PlanDocument3 pagesBDRRM Polo Action Planmicah bitantosNo ratings yet
- INTUSSUSCEPTIONDocument1 pageINTUSSUSCEPTIONAezyreal Anne MirallesNo ratings yet
- IJP Mhca SupplementDocument7 pagesIJP Mhca Supplementgion.nandNo ratings yet
- Vitamin D SupplementsDocument11 pagesVitamin D SupplementsPetra JobovaNo ratings yet
- Job Stress Work Performance With CommentssssDocument37 pagesJob Stress Work Performance With CommentssssAmen MartzNo ratings yet
- DR ScrapbookDocument8 pagesDR Scrapbookcrenz23_shaniyha15No ratings yet
- 89 391 Eec PDFDocument8 pages89 391 Eec PDFBasara MladenNo ratings yet
- We Are What We EatDocument2 pagesWe Are What We EatAlex MgebrishviliNo ratings yet
- Effects of Alcoholism To The BehaviourDocument4 pagesEffects of Alcoholism To The BehaviourJoylyn PerezNo ratings yet
- TractionDocument11 pagesTractionDenalyn Ann TormoNo ratings yet
- Alzheimer Lengkappppp PDFDocument8 pagesAlzheimer Lengkappppp PDFyulan sulemanNo ratings yet
- Hse Induction: KYK Analysis of Potentially Hazardous Area (JSA)Document1 pageHse Induction: KYK Analysis of Potentially Hazardous Area (JSA)teman k3No ratings yet
- Islamic Integrated Cognitive Behavior Therapy: A Shari'ah-Compliant Intervention For Muslims With DepressionDocument10 pagesIslamic Integrated Cognitive Behavior Therapy: A Shari'ah-Compliant Intervention For Muslims With DepressionHANISAH BINTI ABDUL RAHMAN MIC173019No ratings yet