Download as pdf or txt
You might also like
- DR Breath by Carl Stough PDFDocument128 pagesDR Breath by Carl Stough PDFJuan Vizán86% (7)
- Reading Test #32 (Thursday) - MergedDocument28 pagesReading Test #32 (Thursday) - MergedPiper Parker0% (1)
- Med Surg Notes 3Document6 pagesMed Surg Notes 3Ivy NguyenNo ratings yet
- Emphysema Case Study E3Document28 pagesEmphysema Case Study E3scarletsky1975% (8)
- Respiratory Diseases Chapter From Nelson Textbook of PediatricsDocument312 pagesRespiratory Diseases Chapter From Nelson Textbook of PediatricsMilan Andrejevic100% (1)
- Pneumothorax Part ADocument4 pagesPneumothorax Part ASoji0% (1)
- PPP Reading Test 11 Part A TextsDocument4 pagesPPP Reading Test 11 Part A TextsDaniah Marwan Dawood DAWOODNo ratings yet
- Medical Surgical Nursing Module 14Document31 pagesMedical Surgical Nursing Module 14weissNo ratings yet
- Assessment: Suctioning An Adult Patient With An Artificial AirwayDocument2 pagesAssessment: Suctioning An Adult Patient With An Artificial Airwayeunike FriciliaNo ratings yet
- Table of Comparison On Cardiopulmonary Resuscitation For Adul1Document1 pageTable of Comparison On Cardiopulmonary Resuscitation For Adul1Luigi GeduqueNo ratings yet
- AiepiDocument12 pagesAiepiRenzo Iván Marín DávalosNo ratings yet
- Non Invasive VentilationDocument58 pagesNon Invasive VentilationsachinNo ratings yet
- Lung Recruitment in General AnesthesiaDocument2 pagesLung Recruitment in General AnesthesiaIda SutawanNo ratings yet
- Medical Surgical Nursing Module 17Document31 pagesMedical Surgical Nursing Module 17weissNo ratings yet
- Uued Coivd 19mgmt Guide For Publication 9 - 15 - 2020Document29 pagesUued Coivd 19mgmt Guide For Publication 9 - 15 - 2020JorgeNo ratings yet
- Apa3 Cicv FinalDocument1 pageApa3 Cicv FinalRhany Ariesti IndryaniNo ratings yet
- Comprehensive Life Support Tutorial Case 1: Question/Action Information Note/Reference TipsDocument3 pagesComprehensive Life Support Tutorial Case 1: Question/Action Information Note/Reference Tipshyukkie minnieNo ratings yet
- Lung - PathophysiologyDocument66 pagesLung - PathophysiologyjmosserNo ratings yet
- Emergency Department Bronchiolitis Care Guideline: Inclusion CriteriaDocument3 pagesEmergency Department Bronchiolitis Care Guideline: Inclusion CriteriaPatricia KoikyNo ratings yet
- Spontaneous Pneumothorax - Management Feb15Document12 pagesSpontaneous Pneumothorax - Management Feb15samuelNo ratings yet
- PneumothoraxDocument45 pagesPneumothoraxLuknut Nuttamon NukaeowNo ratings yet
- Als2010 NewDocument185 pagesAls2010 NewMuhammad JazibNo ratings yet
- Mechanical VentilationDocument27 pagesMechanical VentilationAnne CamilleNo ratings yet
- Nursing Care Plan Thyroid CancerDocument2 pagesNursing Care Plan Thyroid CancerKathleen DimacaliNo ratings yet
- Spiro Me TryDocument13 pagesSpiro Me TryfatimaabedulkhalikturkeyNo ratings yet
- Application HFOV in NICU - Lily RundjanDocument43 pagesApplication HFOV in NICU - Lily Rundjandiah ayu pitalokaNo ratings yet
- ICU One Pager ARDS v1.1Document1 pageICU One Pager ARDS v1.1Michael LevitNo ratings yet
- Bronchiolitis: See AlsoDocument6 pagesBronchiolitis: See AlsoJuleides De LeonNo ratings yet
- Pulmo Case Simulation-TEAM Yellow-Blue - 01-04-21Document35 pagesPulmo Case Simulation-TEAM Yellow-Blue - 01-04-21Jolaine ValloNo ratings yet
- 5 Advanced Resu PDFDocument22 pages5 Advanced Resu PDFBeatrice Joy TombocNo ratings yet
- OxygenationDocument3 pagesOxygenationFritz MirandaNo ratings yet
- 10.5 Tracheostomies - Clinical Procedures For Safer Patient CareDocument31 pages10.5 Tracheostomies - Clinical Procedures For Safer Patient CareMeg AqNo ratings yet
- TSCUH Trachy Bed Head PDFDocument4 pagesTSCUH Trachy Bed Head PDFTudistef Analize SanatateNo ratings yet
- Respi Hema NotesDocument16 pagesRespi Hema NotesLucky GomezNo ratings yet
- Potential Conflicts of InterestDocument8 pagesPotential Conflicts of InterestLina GuerraNo ratings yet
- Excess or Deficit in Oxygenation And/or Carbon Dioxide Elimination at The Alveolar-Capillary MembraneDocument6 pagesExcess or Deficit in Oxygenation And/or Carbon Dioxide Elimination at The Alveolar-Capillary MembraneHazel MiraranNo ratings yet
- Non Invasive Positive Pressure Ventilation (NIPPV)Document39 pagesNon Invasive Positive Pressure Ventilation (NIPPV)api-3820606100% (1)
- Detresa Respiratorie NeonatalaDocument2 pagesDetresa Respiratorie NeonatalaAndrada CatrinoiuNo ratings yet
- Niv Vizag FinalDocument56 pagesNiv Vizag FinalPrakash PratimaNo ratings yet
- Anaesthetics NotesDocument15 pagesAnaesthetics NotesnaNo ratings yet
- RahpoDocument3 pagesRahpoassouma16052002No ratings yet
- PP Lung VolumesDocument30 pagesPP Lung VolumesAdam PrabowoNo ratings yet
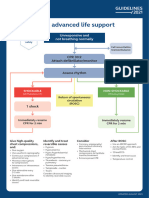
- Adult Advanced Life Support Algorithm 2021 Aug 2023Document1 pageAdult Advanced Life Support Algorithm 2021 Aug 2023cknihilnewNo ratings yet
- Presentasi Code Blue IGDDocument16 pagesPresentasi Code Blue IGDIgd Pondok TjandraNo ratings yet
- CPR Guideline 2022Document12 pagesCPR Guideline 2022Wyndham WooNo ratings yet
- PalsDocument1 pagePalslordroentgenNo ratings yet
- NCP CroupDocument3 pagesNCP Croupaurezea100% (3)
- S T A R T: Imple Riage ND Apid ReatmentDocument17 pagesS T A R T: Imple Riage ND Apid ReatmentNavine NavNo ratings yet
- BLS Healthcare Provider AlgorithmDocument7 pagesBLS Healthcare Provider AlgorithmyuniNo ratings yet
- Pneumothorax: Algorithm: Queen's Dect: KGH BleepDocument2 pagesPneumothorax: Algorithm: Queen's Dect: KGH BleepRachmi Merrina0% (1)
- Anesthesia For Laparoscopic SurgeryDocument14 pagesAnesthesia For Laparoscopic Surgeryhendrik taufikNo ratings yet
- Dean - Diagnostic 1 PDFDocument3 pagesDean - Diagnostic 1 PDFSophia GoNo ratings yet
- Poster 10 PALS 01 01 ENG V20100927 PDFDocument1 pagePoster 10 PALS 01 01 ENG V20100927 PDFAndy XiaoNo ratings yet
- NIV and HFNCDocument16 pagesNIV and HFNCMarceline GarciaNo ratings yet
- Respiratory Cram 6Document1 pageRespiratory Cram 6gwendolyn henryNo ratings yet
- Body CT - Chest HRCTDocument5 pagesBody CT - Chest HRCTKelum BuddhikaNo ratings yet
- Recovery Room Transfer Sheet44Document1 pageRecovery Room Transfer Sheet44Dr. Sumit Kumbhar0% (1)
- ABC AcuteCareDocument1 pageABC AcuteCareparkerNo ratings yet
- Triptico RCPDocument2 pagesTriptico RCPDenia Anguamea CalderónNo ratings yet
- 14.PNEUMOTHORAX + IC TubeDocument8 pages14.PNEUMOTHORAX + IC TubeLankeshwaraNo ratings yet
- 4-5 MV For COPD & AsthmaDocument45 pages4-5 MV For COPD & AsthmasalwafathiNo ratings yet
- RCP TripticoDocument2 pagesRCP Tripticoqg4r5srcnpNo ratings yet
- Hypertension: Hypertensive Emergency Hypertensive UrgencyDocument2 pagesHypertension: Hypertensive Emergency Hypertensive UrgencyAndrei MurariuNo ratings yet
- AsthmaDocument2 pagesAsthmaAndrei MurariuNo ratings yet
- Chest PainDocument5 pagesChest PainAndrei MurariuNo ratings yet
- Physiotherapeutic Management of Patients With Pregnancy-Related Pelvic Girdle PainDocument24 pagesPhysiotherapeutic Management of Patients With Pregnancy-Related Pelvic Girdle PainAndrei MurariuNo ratings yet
- Oxygen DeliveryDocument6 pagesOxygen Deliveryyourdirtysocks100% (1)
- 03 NCP 5 Pulmonary Tuberculosis LalitDocument17 pages03 NCP 5 Pulmonary Tuberculosis Lalitamit100% (2)
- Respiratory - Circulatory SystemDocument3 pagesRespiratory - Circulatory SystemClaude PeñaNo ratings yet
- Body PlathyDocument13 pagesBody PlathyWayanWahyuSemaraPutraNo ratings yet
- Negative Effects of SmokingDocument19 pagesNegative Effects of SmokingAnafemolyn NingascaNo ratings yet
- Worksheet ADocument3 pagesWorksheet AM Riel Cim AlbancesNo ratings yet
- GOLD Pocket 2017Document34 pagesGOLD Pocket 2017Giovanni MisseriNo ratings yet
- 1.chronic Illness Overview and COPDDocument12 pages1.chronic Illness Overview and COPDOmar IzzoNo ratings yet
- Covid - 19 NCPDocument4 pagesCovid - 19 NCPKrisianne Mae Lorenzo FranciscoNo ratings yet
- Question Bank X 202324 BiologyDocument9 pagesQuestion Bank X 202324 Biologyvaibhav4gameNo ratings yet
- 01 1 PDFDocument8 pages01 1 PDFpravikumar1989No ratings yet
- Critical Care Nursing A Holistic ApproachDocument84 pagesCritical Care Nursing A Holistic ApproachMildred GamboaNo ratings yet
- Respiratory Function TestDocument7 pagesRespiratory Function TestMarivic DianoNo ratings yet
- Predisposing Factors Disease Precipitating Factors: LegendDocument3 pagesPredisposing Factors Disease Precipitating Factors: LegendSOPHIA LOISE TEJANO FULACHENo ratings yet
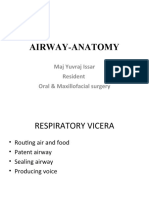
- Airway-Anatomy: Maj Yuvraj Issar Resident Oral & Maxillofacial SurgeryDocument83 pagesAirway-Anatomy: Maj Yuvraj Issar Resident Oral & Maxillofacial SurgeryBhanu PraseedhaNo ratings yet
- Exercise Science and The VocalistDocument10 pagesExercise Science and The VocalistVoz UGM100% (1)
- Worksheet - Week 6 - ANSWERSDocument6 pagesWorksheet - Week 6 - ANSWERSstudent4007No ratings yet
- NCP - Or-Rotation 2Document12 pagesNCP - Or-Rotation 2Vian RiveraNo ratings yet
- Thoracocentesis: Nadja E. SigristDocument4 pagesThoracocentesis: Nadja E. SigristDwi AnaNo ratings yet
- PSLE Science 2020 Booklet ADocument16 pagesPSLE Science 2020 Booklet Asgdogman1212No ratings yet
- Wheezing From PCODocument23 pagesWheezing From PCOShan KaiNo ratings yet
- EXAM 3 20210405 C11 NUR310G.C Health Assessment PDFDocument37 pagesEXAM 3 20210405 C11 NUR310G.C Health Assessment PDFCeciliaNo ratings yet
- Vocabulary Listening Speaking Reading WritingDocument9 pagesVocabulary Listening Speaking Reading Writingnimat rasyidNo ratings yet
- Respiratory SystemhjhuDocument23 pagesRespiratory SystemhjhuSara ANo ratings yet
- MTV1000 - PNEUMACARE (Eng) PDFDocument2 pagesMTV1000 - PNEUMACARE (Eng) PDFNhật LongNo ratings yet
- Breathing - Herbert M. SheltonDocument1 pageBreathing - Herbert M. Sheltonraweater75% (4)
- Avian and Exotic Animal AnesthesiaDocument46 pagesAvian and Exotic Animal AnesthesiaManecas TianeNo ratings yet