Download as pdf or txt
You might also like
- Current Procedural Terminology (CPT CODING)Document5 pagesCurrent Procedural Terminology (CPT CODING)Rabindra P.Singh50% (2)
- Patient Report: Tests Result Flag Units Reference Interval LabDocument1 pagePatient Report: Tests Result Flag Units Reference Interval LabMillennialz MarketingNo ratings yet
- James Tin Yau So - Treatment of Disease With AcupunctureDocument397 pagesJames Tin Yau So - Treatment of Disease With Acupuncturearyaa202096% (26)
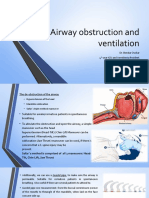
- Airway Obstruction and VentilationDocument8 pagesAirway Obstruction and VentilationJeremias KwapiszNo ratings yet
- Cuerp Extra en Orl-Econa-Feb 2019Document10 pagesCuerp Extra en Orl-Econa-Feb 2019surgeonyNo ratings yet
- ENT Emergency PresentationDocument135 pagesENT Emergency PresentationshahiruddinNo ratings yet
- What Is NeuropathyDocument4 pagesWhat Is NeuropathyLord Pozak MillerNo ratings yet
- Inhalation or Aerosols Therapy1Document21 pagesInhalation or Aerosols Therapy1drnasir31No ratings yet
- Tracheostomy: Dr. Amar KumarDocument18 pagesTracheostomy: Dr. Amar KumarSudhanshu ShekharNo ratings yet
- MSN Question Bank-Unit 1 - Ent: Long Essay 5MDocument31 pagesMSN Question Bank-Unit 1 - Ent: Long Essay 5Mkiran kumarNo ratings yet
- Lecture NPPCD DeafnessDocument35 pagesLecture NPPCD DeafnessAkshay50% (2)
- Anatomy EarDocument44 pagesAnatomy Earrinaldy agungNo ratings yet
- External Ear DisordersDocument48 pagesExternal Ear DisordershemaanandhyNo ratings yet
- Cortical Mastoid SurgeryDocument22 pagesCortical Mastoid Surgerymanu100% (1)
- Ototoxicity LatestDocument37 pagesOtotoxicity LatestSucdi CabdiNo ratings yet
- Ear Irrigation: Nurs 516 Emergency Nursing Care 1 PracticalDocument28 pagesEar Irrigation: Nurs 516 Emergency Nursing Care 1 PracticalMarianne Laylo100% (1)
- Ear, Nose, and Throat EmergenciesDocument23 pagesEar, Nose, and Throat EmergenciesRajesh SharmaNo ratings yet
- NOVEMBER 10, 2021 DAY 2 Intensive Care Unit: Critical Care TeamDocument7 pagesNOVEMBER 10, 2021 DAY 2 Intensive Care Unit: Critical Care TeamLeslie PaguioNo ratings yet
- Tonsillitis & TonsillectomyDocument18 pagesTonsillitis & TonsillectomyLuqman HakimNo ratings yet
- Nasal Fractures: Trauma To NoseDocument38 pagesNasal Fractures: Trauma To NoseSindhura ManjunathNo ratings yet
- Auditory DisordersDocument19 pagesAuditory DisordersJobelle AcenaNo ratings yet
- Hydrocephalus: Mr. Fadi J. Zaben RN MSN IMET2000, Ramallah February, 2013Document30 pagesHydrocephalus: Mr. Fadi J. Zaben RN MSN IMET2000, Ramallah February, 2013WisnuBaskoro100% (1)
- Epistaxis: Presenter: Elesia Powell-WilliamsDocument46 pagesEpistaxis: Presenter: Elesia Powell-Williamselesia powellNo ratings yet
- Cancer LaryncDocument35 pagesCancer LaryncSaya MenangNo ratings yet
- Stages of AnesthesiaDocument8 pagesStages of Anesthesiajanikka100% (1)
- CPR 1Document12 pagesCPR 1Renju JoseNo ratings yet
- OxygenationDocument50 pagesOxygenationLulu MushiNo ratings yet
- Otalgia (Ear Pain)Document43 pagesOtalgia (Ear Pain)Suzzane MNo ratings yet
- Intracranial SurgeryDocument12 pagesIntracranial SurgerysetanpikulanNo ratings yet
- CCLS IRC ISA CPR Guidelines PPT Rakesh GargDocument67 pagesCCLS IRC ISA CPR Guidelines PPT Rakesh GargPiyush JoshiNo ratings yet
- Prognosis MGDocument7 pagesPrognosis MGPutri Cindy Claudia PandoyoNo ratings yet
- Myringotomy & MyringoplastyDocument35 pagesMyringotomy & MyringoplastypriyaNo ratings yet
- Acute Pancreatitis: A Case Study Report ONDocument43 pagesAcute Pancreatitis: A Case Study Report ONArchana MaharjanNo ratings yet
- Acute Suppurative Otitis MediaDocument41 pagesAcute Suppurative Otitis Mediarani suwadjiNo ratings yet
- Endotracheal IntubationDocument1 pageEndotracheal IntubationAnusha VergheseNo ratings yet
- Ultrasound - SummaryDocument19 pagesUltrasound - SummaryHeidar ZaarourNo ratings yet
- CP Head InjuryDocument9 pagesCP Head InjurySindhu S NairNo ratings yet
- BASIC LIFE SUPPORT Basics IntroductionDocument27 pagesBASIC LIFE SUPPORT Basics IntroductionMUKESH SUNDARARAJANNo ratings yet
- Spinal AnesthesiaDocument7 pagesSpinal AnesthesiaAlaa OmarNo ratings yet
- Anatomy of Nose andDocument29 pagesAnatomy of Nose andMuhammad Waqar UlfatNo ratings yet
- A Comparative Study of Phenylephrine, Ephedrine and Mephentermine For Maintainance of Arterial Pressure During Spinal Anaesthesia in Caesarean SectionDocument6 pagesA Comparative Study of Phenylephrine, Ephedrine and Mephentermine For Maintainance of Arterial Pressure During Spinal Anaesthesia in Caesarean SectionInternational Organization of Scientific Research (IOSR)No ratings yet
- Laryngeal CancerDocument41 pagesLaryngeal CancerNidya PutriNo ratings yet
- Pulmonary Function TestDocument57 pagesPulmonary Function TestDeepika PatelNo ratings yet
- CVPDocument23 pagesCVPShalini KaluraNo ratings yet
- Airway Obstruction Final2Document33 pagesAirway Obstruction Final2Mahindra KumarNo ratings yet
- Paediatric TonsillectomyDocument9 pagesPaediatric TonsillectomyAlbert GheorgheNo ratings yet
- Care of Patient On I C DDocument15 pagesCare of Patient On I C DGeorge John Jeelu SusanNo ratings yet
- Renal TransplantationDocument50 pagesRenal Transplantationregie cuaresmaNo ratings yet
- Laryngeal Mask: Is It The Best Supraglottic Airway?Document12 pagesLaryngeal Mask: Is It The Best Supraglottic Airway?Dr. T. BalasubramanianNo ratings yet
- Dhanusthamba/Dhanurvata/Tetanus: Dr. Mahesh C KundagolDocument19 pagesDhanusthamba/Dhanurvata/Tetanus: Dr. Mahesh C KundagolkundagolNo ratings yet
- Case Study On Lung CancerDocument54 pagesCase Study On Lung CancerQusai BassamNo ratings yet
- CVP MonitoringDocument7 pagesCVP Monitoringgurneet kourNo ratings yet
- Et IntubationDocument33 pagesEt Intubationsoniya josephNo ratings yet
- AtelektasisDocument15 pagesAtelektasisMuhammad Ade RahmanNo ratings yet
- LabyrinthitisDocument13 pagesLabyrinthitisDanica Joy Vinluan Jacoba100% (1)
- Seminar Head InjuriesDocument16 pagesSeminar Head InjuriesBONG AIKCHINGNo ratings yet
- Maxillary Sinus CarcinomaDocument4 pagesMaxillary Sinus CarcinomaSuresh MettaNo ratings yet
- Fulminant Hepatic FailureDocument12 pagesFulminant Hepatic Failureafghansyah arfiantoNo ratings yet
- Paranasal Sinus Cancer A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsFrom EverandParanasal Sinus Cancer A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsNo ratings yet
- The Ideal Neutropenic Diet Cookbook; The Super Diet Guide To Replenish Overall Health For A Vibrant Lifestyle With Nourishing RecipesFrom EverandThe Ideal Neutropenic Diet Cookbook; The Super Diet Guide To Replenish Overall Health For A Vibrant Lifestyle With Nourishing RecipesNo ratings yet
- Head and Neck Cancer Care in a Pandemic: Prioritizing Safe CareFrom EverandHead and Neck Cancer Care in a Pandemic: Prioritizing Safe CareNo ratings yet
- Aira Noreen Leyva - Resume ReviewDocument2 pagesAira Noreen Leyva - Resume Reviewapi-447475293No ratings yet
- Republic of The Philippines Tamag, Vigan City 2700 Ilocos Sur Website: MailDocument2 pagesRepublic of The Philippines Tamag, Vigan City 2700 Ilocos Sur Website: MailRenea Joy ArruejoNo ratings yet
- Taurolock ClassicDocument1 pageTaurolock Classicwael abodiabNo ratings yet
- Biologic Width: Understanding and Its Preservation: Review ArticleDocument6 pagesBiologic Width: Understanding and Its Preservation: Review ArticleMedstudNo ratings yet
- About Cervical CancerDocument18 pagesAbout Cervical Canceramilaa.jNo ratings yet
- Newborn CareDocument15 pagesNewborn Caresupritha50% (2)
- Curriculum VitaeDocument2 pagesCurriculum Vitaebriton11No ratings yet
- Rubella VirusDocument14 pagesRubella VirusLincy JohnyNo ratings yet
- BBOC407 Biology For Engineers (CSE Stream) : Module 1 Part 3Document15 pagesBBOC407 Biology For Engineers (CSE Stream) : Module 1 Part 3siddharthasankarmaitraNo ratings yet
- WelcomeDocument74 pagesWelcomeSagarRathodNo ratings yet
- Endocrinologie Si Nursing Curs 3Document4 pagesEndocrinologie Si Nursing Curs 3gabiflori100% (1)
- Client Intake FormDocument1 pageClient Intake Formapi-162312216No ratings yet
- Sealing Ability of MTA For Repair of Lateral Root Perforations Seung Jong Torabinejad 1993 PDFDocument4 pagesSealing Ability of MTA For Repair of Lateral Root Perforations Seung Jong Torabinejad 1993 PDFNunoGonçalvesNo ratings yet
- Blood Typing Lab: Whodunit?Document20 pagesBlood Typing Lab: Whodunit?Fate GalvezNo ratings yet
- Assignment/Tugasan MPU2312 Health and Wellness 1 January Semester 2022Document12 pagesAssignment/Tugasan MPU2312 Health and Wellness 1 January Semester 2022Mohd Akmal Hadi Bin Abu SamahNo ratings yet
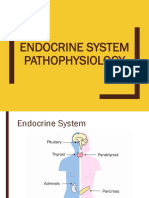
- Endocrine System (Pathophysiology)Document18 pagesEndocrine System (Pathophysiology)roselle legson100% (1)
- Bioreactor Concepts For Cell Culture-Based Viral Vaccine ProductionDocument15 pagesBioreactor Concepts For Cell Culture-Based Viral Vaccine ProductionJohn Lloyd GenerosoNo ratings yet
- Program Book Eye Clinic 2018Document3 pagesProgram Book Eye Clinic 2018Hafiz AzmiNo ratings yet
- Buku OrthopaediDocument6 pagesBuku OrthopaediPriza RazunipNo ratings yet
- Interpersonal Communication Process Recording (Day 1)Document7 pagesInterpersonal Communication Process Recording (Day 1)Kiela Nicole Gatpandan Aguilar100% (2)
- Fear Related To Threat of DystociaDocument2 pagesFear Related To Threat of DystociaMark FernandezNo ratings yet
- 1 Slide BiasaDocument19 pages1 Slide BiasaFransiska Padma Dewi100% (1)
- Revenue Cycle MGMT in Healthcare 414 v1Document426 pagesRevenue Cycle MGMT in Healthcare 414 v1Pravin DixitNo ratings yet
- ProiecttDocument4 pagesProiecttAdriana Elena DoneNo ratings yet
- Understanding Jugular Venous Outflow DisturbanceDocument10 pagesUnderstanding Jugular Venous Outflow DisturbanceAleksandre KordzadzeNo ratings yet
- SultamicillinDocument2 pagesSultamicillinJesselle LasernaNo ratings yet
- Fad Diet ProjectDocument2 pagesFad Diet ProjectHayden GieldaNo ratings yet