Download as pdf or txt
You might also like
- Final Ethical AnalysisDocument5 pagesFinal Ethical Analysisapi-472030023No ratings yet
- NRC Sam Chart: For Oedematous Child Admission Weight Will Be The Weight Taken On The Day The Child Has No OedemaDocument5 pagesNRC Sam Chart: For Oedematous Child Admission Weight Will Be The Weight Taken On The Day The Child Has No OedemaadiNo ratings yet
- Factors Associated With Molar-Incisor Hypomineralization: A Population-Based Case-Control StudyDocument7 pagesFactors Associated With Molar-Incisor Hypomineralization: A Population-Based Case-Control StudyanonimoNo ratings yet
- Medication ErrorsDocument11 pagesMedication ErrorsagegnehuNo ratings yet
- Ijerph 16 03996Document11 pagesIjerph 16 03996Cristine ChubiboNo ratings yet
- Knowledge, Attitudes and Practices of The Medical Personnel Regarding Atopic Dermatitis in Yaoundé, CameroonDocument7 pagesKnowledge, Attitudes and Practices of The Medical Personnel Regarding Atopic Dermatitis in Yaoundé, CameroonNadira Juanti PratiwiNo ratings yet
- The Influence of An Accredited Pediatric Emergency Medicine Program On The Management of Pediatric Pain and AnxietyDocument5 pagesThe Influence of An Accredited Pediatric Emergency Medicine Program On The Management of Pediatric Pain and AnxietyLotta AyuniyahNo ratings yet
- Journal PNTD 0001732Document8 pagesJournal PNTD 0001732itho23No ratings yet
- Child Abuse Inventory at Emergency Rooms: CHAIN-ER Rationale and DesignDocument7 pagesChild Abuse Inventory at Emergency Rooms: CHAIN-ER Rationale and DesignIsnaNo ratings yet
- Artigo 2 Prevalencia ChinaDocument7 pagesArtigo 2 Prevalencia ChinaCarmen AdamesNo ratings yet
- Development and Pilot Study of A Pediatric Screening ForDocument12 pagesDevelopment and Pilot Study of A Pediatric Screening Forsiramliw3No ratings yet
- Effectiveness of Structured Teaching Program On Knowledge Regarding Home Care Management of Children With Hydrocephalus and Shunt Among Their ParentsDocument3 pagesEffectiveness of Structured Teaching Program On Knowledge Regarding Home Care Management of Children With Hydrocephalus and Shunt Among Their ParentsIrnayanti MamiDgSiameNo ratings yet
- Medication Error Factors, Safety Guideline System, Flow of Drug Usage, and Code of Conduct To Prevent Medication ErrorDocument5 pagesMedication Error Factors, Safety Guideline System, Flow of Drug Usage, and Code of Conduct To Prevent Medication ErrorskyNo ratings yet
- The Use of Patient Complaints To Drive QualityDocument8 pagesThe Use of Patient Complaints To Drive QualitysanaaNo ratings yet
- Integrated Management of Childhood Illness in Outpatient Department of A University HospitalDocument6 pagesIntegrated Management of Childhood Illness in Outpatient Department of A University Hospitalpastizal123456No ratings yet
- J Pedn 2019 09 022Document8 pagesJ Pedn 2019 09 022aminNo ratings yet
- NursingDocument15 pagesNursingVikash KumarNo ratings yet
- 1471 2431 12 72Document8 pages1471 2431 12 72Manuel DuranNo ratings yet
- WeeFIM Clinical ReviewDocument10 pagesWeeFIM Clinical Reviewsss_sarzzzNo ratings yet
- Article 4Document8 pagesArticle 4gogih64190No ratings yet
- Kumpulan Jurnal InternasionalDocument15 pagesKumpulan Jurnal InternasionalTIKANo ratings yet
- 2018 - Baraki Et AlDocument8 pages2018 - Baraki Et AlazeemathmariyamNo ratings yet
- Pengobatan Alternatif AnakDocument8 pagesPengobatan Alternatif AnakjayaNo ratings yet
- Sociodemographic Factors and Health Care Seeking Behaviours For Childhood IllnessesDocument7 pagesSociodemographic Factors and Health Care Seeking Behaviours For Childhood IllnessesTengiz VerulavaNo ratings yet
- Out 17Document10 pagesOut 17laodesyuhadarNo ratings yet
- CitarDocument3 pagesCitarVictor NamurNo ratings yet
- A Cross-Sectional Study of Behavioural Disorders in Children With Human Immunodeficiency Virus / Acquired Immuno Deficiency Syndrome Attending An Anti-Retroviral Therapy CentreDocument6 pagesA Cross-Sectional Study of Behavioural Disorders in Children With Human Immunodeficiency Virus / Acquired Immuno Deficiency Syndrome Attending An Anti-Retroviral Therapy CentreKumaravel KSNo ratings yet
- Pone 0201107Document12 pagesPone 0201107Khoirul AnwarNo ratings yet
- Utilization of The Naranjo Scale To Evaluate Adverse Drug Reactions at A Free-Standing Children's HospitalDocument10 pagesUtilization of The Naranjo Scale To Evaluate Adverse Drug Reactions at A Free-Standing Children's HospitalSheerazNo ratings yet
- INCLEN Diagnostic Tool For Epilepsy (INDT-EPI) For Primary Care Physicians: Development and ValidationDocument5 pagesINCLEN Diagnostic Tool For Epilepsy (INDT-EPI) For Primary Care Physicians: Development and ValidationAulya ArchuletaNo ratings yet
- Rapid Detection of Internalizing Diagnosis in Young Children - Ryan McGinnin Et. Al2019Document16 pagesRapid Detection of Internalizing Diagnosis in Young Children - Ryan McGinnin Et. Al2019Vitória AlvesNo ratings yet
- 431 2011 Article 1608Document6 pages431 2011 Article 1608Ahmad NurdiansyahNo ratings yet
- Jurnal Baru 2Document6 pagesJurnal Baru 2FIRDA RIDHAYANINo ratings yet
- Rudeness and PerformanceDocument11 pagesRudeness and Performanceluisoliveira94No ratings yet
- 10 1093@intqhc@mzx017 PDFDocument6 pages10 1093@intqhc@mzx017 PDFMeli SariNo ratings yet
- Systematic Review of The Measurement Properties of Tools Used To Measure Behaviour Problems in Young Children With Autism - PMCDocument26 pagesSystematic Review of The Measurement Properties of Tools Used To Measure Behaviour Problems in Young Children With Autism - PMCDaniel NovakNo ratings yet
- Retrospective Evaluation of Single Patient InvestiDocument9 pagesRetrospective Evaluation of Single Patient InvestiDawit BirhanuNo ratings yet
- PrEP WulandariDocument12 pagesPrEP WulandariSeptian 99No ratings yet
- Ijic PDFDocument7 pagesIjic PDFitalatif1No ratings yet
- 7.delirium Knowledge, Self-Confidence, and Attitude in Pediatric IntensiveDocument6 pages7.delirium Knowledge, Self-Confidence, and Attitude in Pediatric IntensivemarieNo ratings yet
- Research Article: Preoperative Anxiety in Greek Children and Their Parents When Presenting For Routine SurgeryDocument7 pagesResearch Article: Preoperative Anxiety in Greek Children and Their Parents When Presenting For Routine SurgeryVania CasaresNo ratings yet
- Evaluation of Poisoning Cases Admitted To Pediatric Emergency DepartmentDocument6 pagesEvaluation of Poisoning Cases Admitted To Pediatric Emergency DepartmentniaNo ratings yet
- His 4Document165 pagesHis 4Anjum100% (2)
- Pone 0230187Document8 pagesPone 0230187Azizah HalidNo ratings yet
- Chapter Three Research Methodology 3.1 Research DesignDocument7 pagesChapter Three Research Methodology 3.1 Research DesignAmeliaNo ratings yet
- 50 10402 1 PB1Document5 pages50 10402 1 PB1Ramya SaravananNo ratings yet
- Health&Clinical ManagementDocument125 pagesHealth&Clinical ManagementAnjum100% (1)
- Refractive Errors and Visual AnomaliesDocument19 pagesRefractive Errors and Visual Anomaliesfor documentNo ratings yet
- 2018 Article 5790Document10 pages2018 Article 5790fitri asymidaNo ratings yet
- PAEDSDocument8 pagesPAEDSAtzi FNo ratings yet
- A Guide For Monitoring Child Development PDFDocument11 pagesA Guide For Monitoring Child Development PDFneutralna0% (1)
- Triage Methods inDocument3 pagesTriage Methods inAvinooNo ratings yet
- Priyanka K P Synopsis-1Document18 pagesPriyanka K P Synopsis-1RAJESHWARI PNo ratings yet
- Reflex Anal Dilatation An Observational Study On Non-Abused ChildrenDocument5 pagesReflex Anal Dilatation An Observational Study On Non-Abused Childrenaniendyawijaya0% (1)
- Stunting 2 PDFDocument7 pagesStunting 2 PDFPermata HatiNo ratings yet
- The Use of Patient Complaints To Drive Quality Improvement: An Exploratory Study in TaiwanDocument7 pagesThe Use of Patient Complaints To Drive Quality Improvement: An Exploratory Study in TaiwanNurhafifa YusufNo ratings yet
- Assessing The Construct Validity and Reliability of The Parental Perception On Antibiotics (PAPA) ScalesDocument9 pagesAssessing The Construct Validity and Reliability of The Parental Perception On Antibiotics (PAPA) ScalesAl ANo ratings yet
- SisayDocument9 pagesSisaysisayNo ratings yet
- Effects of Self-Education On Patient Safety Via Smartphone Application For Self-Efficacy and Safety Behaviors of Inpatients in KoreaDocument9 pagesEffects of Self-Education On Patient Safety Via Smartphone Application For Self-Efficacy and Safety Behaviors of Inpatients in Korea'Amel'AyuRizkyAmeliyahNo ratings yet
- Adherence To Medication Behavior Among TuberculosiDocument7 pagesAdherence To Medication Behavior Among TuberculosiPPI RSUI MBNo ratings yet
- Manuscript UvA DAREDocument60 pagesManuscript UvA DAREMaria Carmela DomocmatNo ratings yet
- Tips and Guidelines For Being A Successful ResearcherDocument11 pagesTips and Guidelines For Being A Successful ResearcherMaria Carmela DomocmatNo ratings yet
- Identifying Child AbuseDocument36 pagesIdentifying Child AbuseMaria Carmela DomocmatNo ratings yet
- Teenage Pregnancy. The Making and Unmaking of A ProblemDocument190 pagesTeenage Pregnancy. The Making and Unmaking of A ProblemMaria Carmela DomocmatNo ratings yet
- Wahid Identifying Risk Factors and Detection Strategies... A Delphi Consensus StudyDocument9 pagesWahid Identifying Risk Factors and Detection Strategies... A Delphi Consensus StudyMaria Carmela DomocmatNo ratings yet
- Saturation Controversy in Qualitative ResearchDocument18 pagesSaturation Controversy in Qualitative ResearchMaria Carmela DomocmatNo ratings yet
- WHO. Fatherhood and Health Outcomes in EuropeDocument40 pagesWHO. Fatherhood and Health Outcomes in EuropeMaria Carmela DomocmatNo ratings yet
- Adolescent Motherhood.Document7 pagesAdolescent Motherhood.Maria Carmela DomocmatNo ratings yet
- Addressing Policy Barriers To Paternal Involvement During Pregnancy.Document7 pagesAddressing Policy Barriers To Paternal Involvement During Pregnancy.Maria Carmela DomocmatNo ratings yet
- Thesis. It Takes Two - Exploring The Supportive Role of Fathers During PRDocument17 pagesThesis. It Takes Two - Exploring The Supportive Role of Fathers During PRMaria Carmela DomocmatNo ratings yet
- Covid Vaccine StatewiseDocument488 pagesCovid Vaccine Statewisearun prakashNo ratings yet
- World Breastfeeding Week CeleberationDocument9 pagesWorld Breastfeeding Week CeleberationanchalNo ratings yet
- National Immunization Program (NIP) : Mary Ann E. Lopez MAN RN LPTDocument26 pagesNational Immunization Program (NIP) : Mary Ann E. Lopez MAN RN LPTJanaica JuanNo ratings yet
- LBWelmiskiryDocument24 pagesLBWelmiskirywizborrlyzo006No ratings yet
- GROW VP NB Combined Zs Boys enDocument2 pagesGROW VP NB Combined Zs Boys enHazel GaringoNo ratings yet
- Test Bank For Pediatric Nursing: Caring For Children and Their Families, 3rd Edition, Nicki L. Potts, Barbara L. MandlecoDocument33 pagesTest Bank For Pediatric Nursing: Caring For Children and Their Families, 3rd Edition, Nicki L. Potts, Barbara L. Mandlecoterreity.warfarehsstta100% (15)
- Pediatric Exercise ScienceDocument5 pagesPediatric Exercise ScienceRomee Nica LegaspiNo ratings yet
- 68W Perform A Medical Patient AssessmentDocument6 pages68W Perform A Medical Patient Assessmentsmith.kevin1420344No ratings yet
- 5.Gianotti-Crosti SyndromeDocument3 pages5.Gianotti-Crosti SyndromeerwinssNo ratings yet
- SohailDocument1 pageSohailfamliyli670No ratings yet
- Breastfeeding TechniqueDocument2 pagesBreastfeeding TechniqueKaye Niale BaleteNo ratings yet
- Immunizations For TravelDocument5 pagesImmunizations For TravelMuhammad AdilNo ratings yet
- Tugas KKPMT Kamis, 17 Juni 2021 Nama: Amellia Gustha Chintya Cristy NIM: 195044 Kelas: 2BDocument2 pagesTugas KKPMT Kamis, 17 Juni 2021 Nama: Amellia Gustha Chintya Cristy NIM: 195044 Kelas: 2BDyah CitraNo ratings yet
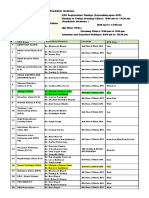
- OPD Schedule DoctorsDocument3 pagesOPD Schedule DoctorssahilNo ratings yet
- 14 Congenital Anomalies of CNSDocument5 pages14 Congenital Anomalies of CNSBella DonnaNo ratings yet
- Certificate For COVID-19 Vaccination: Beneficiary DetailsDocument1 pageCertificate For COVID-19 Vaccination: Beneficiary DetailsLakshya NagotaNo ratings yet
- Vaccination CentersDocument4 pagesVaccination CentersdmonlinelkNo ratings yet
- Certificate For COVID-19 Vaccination: Beneficiary DetailsDocument1 pageCertificate For COVID-19 Vaccination: Beneficiary DetailsDIGITAL 143No ratings yet
- Rachel Corbin FNP - Curriculum VitaeDocument4 pagesRachel Corbin FNP - Curriculum Vitaeapi-311508350No ratings yet
- Etiology and Clinical Presentation of Birth DefectDocument8 pagesEtiology and Clinical Presentation of Birth DefectJohnjohnNo ratings yet
- Certificate For COVID-19 Vaccination: Beneficiary DetailsDocument1 pageCertificate For COVID-19 Vaccination: Beneficiary DetailsAbdul khadarNo ratings yet
- Barangay Monthly Inventory of Vaccinated PopulationDocument2 pagesBarangay Monthly Inventory of Vaccinated PopulationGenzo TaniaNo ratings yet
- National Course Dates 2024Document2 pagesNational Course Dates 20245gr4wvbbg5No ratings yet
- Neonatal Intensive Care UnitDocument2 pagesNeonatal Intensive Care Unitapi-453449063No ratings yet
- NURS FPX 6111 Assessment 1 Course Definition and Alignment TableDocument5 pagesNURS FPX 6111 Assessment 1 Course Definition and Alignment TableCarolyn HarkerNo ratings yet
- Holding Company For Biological Products & Vaccines: DR: Mostafa Mohamady General Manager of VaccinesDocument65 pagesHolding Company For Biological Products & Vaccines: DR: Mostafa Mohamady General Manager of Vaccineskoky123456789No ratings yet
- Carcinocine in PaediatricsDocument5 pagesCarcinocine in Paediatricssimiliadoc100% (1)
- Pengaruh Pemberian Terapi Latihan Metode SchrothDocument7 pagesPengaruh Pemberian Terapi Latihan Metode SchrothsulaimanNo ratings yet
- PediaDocument3 pagesPediabalas4u89No ratings yet