Download as pdf or txt
You might also like
- Ts Forms LatestDocument40 pagesTs Forms Latestpeter phiri100% (1)
- Be Completed by All Applicants in Triplicate) : Ts. FormDocument4 pagesBe Completed by All Applicants in Triplicate) : Ts. FormLubinda Lubinda Jr.81% (31)
- CC1 Founding StatementDocument10 pagesCC1 Founding Statementmaandero100% (2)
- Personnel Reg FormDocument9 pagesPersonnel Reg FormyodejiNo ratings yet
- Government of Canada: Structure and FunctionDocument7 pagesGovernment of Canada: Structure and FunctionAthena HuynhNo ratings yet
- Music Sync LicenseDocument3 pagesMusic Sync LicenseKahmishKhanNo ratings yet
- Vacation Leave (Form)Document1 pageVacation Leave (Form)Sajoune RoseNo ratings yet
- Contractor FormDocument2 pagesContractor FormMuhammadSyafie100% (1)
- 07 TOTAL PERMANENT DISABILITY Claim Form V1.0 2018Document6 pages07 TOTAL PERMANENT DISABILITY Claim Form V1.0 2018Veron AcNo ratings yet
- New Loan Application FormDocument3 pagesNew Loan Application FormAKANKWASA ERASMUSNo ratings yet
- Professional Engineer Form PDFDocument3 pagesProfessional Engineer Form PDFBob MbuguaNo ratings yet
- 32.leave Application FormDocument1 page32.leave Application FormkomalnkishNo ratings yet
- Attendance Adjustment SlipDocument1 pageAttendance Adjustment Sliparifa siddiquaNo ratings yet
- 13.9001.1leave FormDocument1 page13.9001.1leave FormAshiq Elahi Design & Application EngineerNo ratings yet
- Application For Leave: SL No. Date: .Document1 pageApplication For Leave: SL No. Date: .t m murshedNo ratings yet
- OUS Employment Application Form - 052023Document5 pagesOUS Employment Application Form - 052023amin sarilNo ratings yet
- Employment Application Form - Trader2uDocument5 pagesEmployment Application Form - Trader2uAaron Shahz AdzmieNo ratings yet
- National Insurance Scheme Application For Compliance Certificate (Self-Employed Persons)Document1 pageNational Insurance Scheme Application For Compliance Certificate (Self-Employed Persons)DeSouza JuvitaNo ratings yet
- Form Aplikasi PelamarDocument5 pagesForm Aplikasi PelamarM. RohmatullahNo ratings yet
- Leavea Application FormatDocument1 pageLeavea Application Formatsunshinequalityu4No ratings yet
- Requsest 2Document2 pagesRequsest 2Mesafint lisanuNo ratings yet
- Job Application Form at URSB: Please Fill in All The Information (Where Applicable) 1. Personal InformationDocument4 pagesJob Application Form at URSB: Please Fill in All The Information (Where Applicable) 1. Personal InformationsdsadsadNo ratings yet
- AAS 2025 - Government Approval Letter Template 3Document1 pageAAS 2025 - Government Approval Letter Template 3Ibrahim AdamaNo ratings yet
- Membership Form - 2018-2019Document1 pageMembership Form - 2018-2019sakshiaggarwal838389No ratings yet
- Mks CPSB Form 2022Document3 pagesMks CPSB Form 2022Eunice Mueni paulNo ratings yet
- Mks CPSB Job Application Form 2022Document3 pagesMks CPSB Job Application Form 2022n8brjz5n8zNo ratings yet
- Form B2 A Application For RegistrationDocument2 pagesForm B2 A Application For RegistrationDavid AldoNo ratings yet
- Derric Joyluck 22Document1 pageDerric Joyluck 22kingskevo2024No ratings yet
- Job Application Form-1Document4 pagesJob Application Form-1musa ballah koromaNo ratings yet
- 12 RecruitmentNoticeDocument11 pages12 RecruitmentNoticeABDUL HAINo ratings yet
- Candidate Register FormatDocument2 pagesCandidate Register Formatphyo7799No ratings yet
- Permission LetterDocument1 pagePermission LetterJubilance Tech & RealtorsNo ratings yet
- Application Form For TeachersDocument4 pagesApplication Form For TeachersMunaf M ChowdhuryNo ratings yet
- 1662725026318-1662725013173-Student Reg Form - BlankDocument4 pages1662725026318-1662725013173-Student Reg Form - BlankRuvarasheNo ratings yet
- Photo: The Rwanda Medical and Dental CouncilDocument1 pagePhoto: The Rwanda Medical and Dental CouncilAjay IyerNo ratings yet
- Leave Application FormDocument1 pageLeave Application Formsheireen6No ratings yet
- (B) Application Form For Parcel Sub-Division - KinyaDocument1 page(B) Application Form For Parcel Sub-Division - KinyaNTIGURIRWA JEAN MARIE VIANNEY100% (1)
- Form Requesition StaffDocument1 pageForm Requesition Staffarielaghaim4No ratings yet
- Southsea Skatepark - Application FormDocument4 pagesSouthsea Skatepark - Application FormkadeNo ratings yet
- (Use Only A4 Size Thick Paper For Printing The Form and For The Enclosures. Please ( ) in The Appropriate Boxes)Document7 pages(Use Only A4 Size Thick Paper For Printing The Form and For The Enclosures. Please ( ) in The Appropriate Boxes)Priyabrata PradhanNo ratings yet
- Application Format: Name of The Post Applied ForDocument2 pagesApplication Format: Name of The Post Applied ForArijit ShomeNo ratings yet
- Application Forms For Trainee Professional MembersDocument6 pagesApplication Forms For Trainee Professional MembersSilas Nana-Baah Mensah100% (3)
- Application For Employment Form - THPAL (2014-05) PDFDocument7 pagesApplication For Employment Form - THPAL (2014-05) PDFRome CamingueNo ratings yet
- Umfolozi Municipality Application For Employment: 1. Personal (Block Letters)Document2 pagesUmfolozi Municipality Application For Employment: 1. Personal (Block Letters)ZandileNo ratings yet
- Employment Application Form - NewDocument7 pagesEmployment Application Form - Newshaikh zaidNo ratings yet
- Mine Engineers DiplomaDocument1 pageMine Engineers Diplomacrimson.industries.ltdNo ratings yet
- Log - Book (1) EditedDocument3 pagesLog - Book (1) EditedObaNo ratings yet
- Annual Leave FormsDocument2 pagesAnnual Leave FormsMercy DubeNo ratings yet
- Leave Form 2020Document1 pageLeave Form 2020ABDULLAH AL AHASANNo ratings yet
- Application Form: JOB APPLIED FOR: 1.0 Applicants' ParticularsDocument3 pagesApplication Form: JOB APPLIED FOR: 1.0 Applicants' ParticularsTom SesenteNo ratings yet
- Clearance FormDocument4 pagesClearance FormKenneth AderaNo ratings yet
- Application For The Refund of Caution Money PDFDocument4 pagesApplication For The Refund of Caution Money PDFRadhikaNo ratings yet
- PSC A HodDocument1 pagePSC A HodCharles KahunjaNo ratings yet
- Tick The One That Is Applicable To You Below.: Form KPF 3. VDocument1 pageTick The One That Is Applicable To You Below.: Form KPF 3. VTimoara NatanNo ratings yet
- Confidential: Position Applied For: Salary ExpectedDocument4 pagesConfidential: Position Applied For: Salary ExpectedRichard ZhemiNo ratings yet
- Application - Loan Overdraft Against DepositDocument5 pagesApplication - Loan Overdraft Against DepositUday Kiran0% (1)
- Revised Unit Additional Form - Mku-Adr-F021Document3 pagesRevised Unit Additional Form - Mku-Adr-F021d cNo ratings yet
- Course Title Course Dates: Application FormDocument1 pageCourse Title Course Dates: Application FormMayamiko VililiNo ratings yet
- Feedback FormDocument1 pageFeedback FormAnsar HusainNo ratings yet
- FLI Employee Complaint Report FormDocument3 pagesFLI Employee Complaint Report FormKhisa WekesaNo ratings yet
- Undang-Undang 0Document1 pageUndang-Undang 0lawassarawak2023No ratings yet
- American Credit Repair: Everything U Need to Know About Raising Your Credit ScoreFrom EverandAmerican Credit Repair: Everything U Need to Know About Raising Your Credit ScoreRating: 3 out of 5 stars3/5 (3)
- FQH 102 Assignment Fall 2023Document4 pagesFQH 102 Assignment Fall 2023Moh'd Khamis SongoroNo ratings yet
- IT202 Assignment Fall 2023Document5 pagesIT202 Assignment Fall 2023Moh'd Khamis SongoroNo ratings yet
- Advetisement Sample DesignDocument1 pageAdvetisement Sample DesignMoh'd Khamis SongoroNo ratings yet
- Moh'D Khamis Songoro (Mfalme), Vikunguni Chake Chake, Pemba Tuzitunze Funga ZetuDocument1 pageMoh'D Khamis Songoro (Mfalme), Vikunguni Chake Chake, Pemba Tuzitunze Funga ZetuMoh'd Khamis SongoroNo ratings yet
- Development As FreedomDocument13 pagesDevelopment As FreedomMoh'd Khamis SongoroNo ratings yet
- Costco Mission Statement and Code of EthicsDocument4 pagesCostco Mission Statement and Code of EthicsEduardo PulidoNo ratings yet
- State CourtsDocument142 pagesState Courtsacie600No ratings yet
- Garcia V.calalimanDocument6 pagesGarcia V.calalimanJie JessNo ratings yet
- Chhattisgarh Nagar Tatha Gram Nivesh Adhiniyam, 1973Document12 pagesChhattisgarh Nagar Tatha Gram Nivesh Adhiniyam, 1973Aayushi GodseNo ratings yet
- Transfer Pricing OverviewDocument55 pagesTransfer Pricing OverviewPraygod ManaseNo ratings yet
- Neyra v. NeyraDocument8 pagesNeyra v. NeyraCon PuNo ratings yet
- Imani V MetrobankDocument1 pageImani V MetrobankAllen Windel BernabeNo ratings yet
- Ref. No. 5/2 (T/NT) /2018/data Bank/Pers.: Wapcos LimitedDocument1 pageRef. No. 5/2 (T/NT) /2018/data Bank/Pers.: Wapcos LimitedTridib DeNo ratings yet
- Effect of Repeal of Statutory Law A Judicial Precedent Based StudyDocument21 pagesEffect of Repeal of Statutory Law A Judicial Precedent Based StudyJohn AbrahamNo ratings yet
- Sanchez Leonen IIDocument16 pagesSanchez Leonen IIBfp Siniloan FS LagunaNo ratings yet
- Merseyside: Merseyside (/ Mɜ Rzisaɪd/) Is A Metropolitan County inDocument8 pagesMerseyside: Merseyside (/ Mɜ Rzisaɪd/) Is A Metropolitan County inAnonymous 33NJRexAWlNo ratings yet
- Functions of VDBDocument2 pagesFunctions of VDBTewNo ratings yet
- Daniel Watson v. Robert Adams, 4th Cir. (2016)Document6 pagesDaniel Watson v. Robert Adams, 4th Cir. (2016)Scribd Government DocsNo ratings yet
- Borre vs. CA - DigestDocument2 pagesBorre vs. CA - DigestdudlyriosNo ratings yet
- Law On SalesDocument29 pagesLaw On SalesPaula See Tiong100% (1)
- Primer On Secrecy of Bank Deposits and Foreign Currency DepoDocument10 pagesPrimer On Secrecy of Bank Deposits and Foreign Currency DepoNodlesde Awanab ZurcNo ratings yet
- 5006 TC 05eDocument2 pages5006 TC 05eapi-3836185No ratings yet
- United States v. James R. Gallup, United States of America v. Darryl E. Duke, 812 F.2d 1271, 10th Cir. (1987)Document16 pagesUnited States v. James R. Gallup, United States of America v. Darryl E. Duke, 812 F.2d 1271, 10th Cir. (1987)Scribd Government DocsNo ratings yet
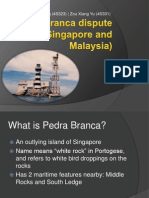
- Pedra Branca DisputeDocument22 pagesPedra Branca DisputeMel VinzNo ratings yet
- Polgov Humss11aDocument11 pagesPolgov Humss11aDiosa Joyce Perico PedroNo ratings yet
- League of Nations PDFDocument19 pagesLeague of Nations PDFEfaz Mahamud AzadNo ratings yet
- Ilogon Vs Sandiganbayan, 218 SCRA 766Document5 pagesIlogon Vs Sandiganbayan, 218 SCRA 766AddAllNo ratings yet
- Dealings in Property-Income TaxationDocument70 pagesDealings in Property-Income TaxationKana Lou Cassandra Besana67% (3)
- Amount Chargeable (In Words)Document1 pageAmount Chargeable (In Words)Saurav Kumar SinghNo ratings yet
- Jimenez, Et Al V NLRC and JuanatasDocument1 pageJimenez, Et Al V NLRC and Juanatasida_chua80230% (1)
- He Imes Eader: 2nd Machete Attack Arrest MadeDocument32 pagesHe Imes Eader: 2nd Machete Attack Arrest MadeThe Times LeaderNo ratings yet
- Sexual Assault of Students in Allentown, Pa., Schools ConsentDocument36 pagesSexual Assault of Students in Allentown, Pa., Schools Consentmary engNo ratings yet