Download as pdf or txt
You might also like
- TB Skin Test FormDocument1 pageTB Skin Test Formapi-381635811No ratings yet
- MOA Template - Ambulance TemplateDocument4 pagesMOA Template - Ambulance TemplatevgruayaNo ratings yet
- Educational Assessment Mcqs For PSC HeadmasterDocument24 pagesEducational Assessment Mcqs For PSC Headmastersrinivasana67% (132)
- Rev2 4132015 Mfows Coa atDocument7 pagesRev2 4132015 Mfows Coa atGlenn PecoroNo ratings yet
- Policy & Procedure For Retention and Destruction of Medical RecordsDocument7 pagesPolicy & Procedure For Retention and Destruction of Medical RecordsAniruddha ChatterjeeNo ratings yet
- Annual Health Check Up FormDocument1 pageAnnual Health Check Up FormNayan RoychowdhuryNo ratings yet
- BGH - CAre PlanDocument55 pagesBGH - CAre PlanmalaramamurthyNo ratings yet
- Program For Calibration, Preventive Maintenance Final PDFDocument28 pagesProgram For Calibration, Preventive Maintenance Final PDFMatthew Pacardo100% (1)
- Lercanidipine Hydrochloride 10mg and 20mg Film-Coated TabletsDocument65 pagesLercanidipine Hydrochloride 10mg and 20mg Film-Coated TabletsPai GampaengkamNo ratings yet
- HPD-DRG-002-1 Custody and Control Form (Form DT-002B - Copy For The Collection Site) - WES - Rev 04 OLD FROMDocument1 pageHPD-DRG-002-1 Custody and Control Form (Form DT-002B - Copy For The Collection Site) - WES - Rev 04 OLD FROMmbyedithNo ratings yet
- QSP 04 Procedure For Referral of PatientDocument6 pagesQSP 04 Procedure For Referral of PatientAniruddha ChatterjeeNo ratings yet
- Pasay City General Hospital: Group 5 Trogon Trovela Vicera Ylade Zapata Bs Pharmacy-Q3ADocument18 pagesPasay City General Hospital: Group 5 Trogon Trovela Vicera Ylade Zapata Bs Pharmacy-Q3AKronii OuroNo ratings yet
- Medical Check Up ProposalDocument4 pagesMedical Check Up ProposalAnggia YanuarNo ratings yet
- Nmhaacqsp1 Policy & Procedure For Admission and Registration of Patient & Non-Availability of BedsDocument16 pagesNmhaacqsp1 Policy & Procedure For Admission and Registration of Patient & Non-Availability of BedsAniruddha ChatterjeeNo ratings yet
- Restricted Antimicrobial Order FormDocument1 pageRestricted Antimicrobial Order FormAina HaravataNo ratings yet
- Mindray BS 3600 Laboratory Preventive MaintenanceDocument1 pageMindray BS 3600 Laboratory Preventive MaintenanceCaesar A. AlesnaNo ratings yet
- Inventory of Reagents APRIL 2017Document2 pagesInventory of Reagents APRIL 2017Gretchel Pontilar0% (1)
- Final Scaling SOPDocument12 pagesFinal Scaling SOPBilal Al AliNo ratings yet
- Contingency Plan in Case of Equipment BreakdownDocument1 pageContingency Plan in Case of Equipment BreakdownIcdl BalayanNo ratings yet
- DM 2020-0439 "Omnibus Interim Guidelines On Prevention, Detection, Isolation, Treatment, and Reintegration Strategies For COVID-19"Document55 pagesDM 2020-0439 "Omnibus Interim Guidelines On Prevention, Detection, Isolation, Treatment, and Reintegration Strategies For COVID-19"Seriel TismoNo ratings yet
- Catheterisation Standard Operating ProcedureDocument27 pagesCatheterisation Standard Operating ProcedureSherly RositaNo ratings yet
- Drug Test Request: Accession No.: OR#: Code No.Document6 pagesDrug Test Request: Accession No.: OR#: Code No.OptimaCare MalabonNo ratings yet
- Policies and Procedures CQIPDocument4 pagesPolicies and Procedures CQIPRobjun AlvarezNo ratings yet
- SOP - CQI Policy and PlanDocument13 pagesSOP - CQI Policy and Planaaminah tariqNo ratings yet
- Application For License To Operate A General Clinical LaboratoryDocument6 pagesApplication For License To Operate A General Clinical LaboratoryJasper LimNo ratings yet
- HIV Treatment Hub Self Assessment FormDocument4 pagesHIV Treatment Hub Self Assessment FormGeliza Recede100% (1)
- Blood Station Operational Plan For 2022Document1 pageBlood Station Operational Plan For 2022Edgardo GepullanoNo ratings yet
- Roche Cobas C111 Installation ManualDocument43 pagesRoche Cobas C111 Installation ManualViolet Nampeera0% (1)
- dc2022-0492 Advisory On The Proof of Submission To National Database of Human Resources For Health Information Ssytem (NDHRHIS)Document4 pagesdc2022-0492 Advisory On The Proof of Submission To National Database of Human Resources For Health Information Ssytem (NDHRHIS)HSQMRAD MPINo ratings yet
- Rev 2 REPORTING LABORATORY RESULTS - RevisedDocument1 pageRev 2 REPORTING LABORATORY RESULTS - RevisedAccuprobe Drug TestingNo ratings yet
- SFMC-AnesthesiabPolicies and Procedures (2017)Document77 pagesSFMC-AnesthesiabPolicies and Procedures (2017)HAMMYER ALROKHAMINo ratings yet
- Inspection DrugtestingDocument29 pagesInspection DrugtestingMarvin BautistaNo ratings yet
- Master Health CheckupDocument8 pagesMaster Health CheckupstephenvedhamalarNo ratings yet
- 9-Recruitment of Nursing StaffDocument3 pages9-Recruitment of Nursing StaffakositabonNo ratings yet
- Drug Testing Consent Form SampleDocument1 pageDrug Testing Consent Form SampleRichard R M ThodéNo ratings yet
- Policy Critical ResultDocument6 pagesPolicy Critical ResultSafiqulatif AbdillahNo ratings yet
- Basic Doh Peme For OcwDocument44 pagesBasic Doh Peme For OcwEvangeline Antonio-TorresNo ratings yet
- Review Checklist For Hospital RenewalDocument1 pageReview Checklist For Hospital RenewalRhodora BenipayoNo ratings yet
- Standards For MIS - 2nd Edition - EditedDocument75 pagesStandards For MIS - 2nd Edition - EditedSmita SaxenaNo ratings yet
- PBF Manual Hospital and Health CenterDocument44 pagesPBF Manual Hospital and Health CenterDamasceneNo ratings yet
- MOU CanteenDocument3 pagesMOU CanteenT AnandNo ratings yet
- Blood Requisition FormDocument2 pagesBlood Requisition FormPrashant Kumar Singh100% (1)
- Rights of The PatientDocument2 pagesRights of The PatientJaymart CostillasNo ratings yet
- New Discount Letter FormatDocument2 pagesNew Discount Letter FormatvikashNo ratings yet
- DHCC - Standards For Clinical Laboratory ServicesDocument25 pagesDHCC - Standards For Clinical Laboratory ServicesRahul MandalNo ratings yet
- Dialysis Application For LTO Rev1 1232014Form-HDC-LTO-A-2007Document12 pagesDialysis Application For LTO Rev1 1232014Form-HDC-LTO-A-2007al gulNo ratings yet
- dc2019 0497Document6 pagesdc2019 0497frenzybabyNo ratings yet
- DRAFT NABH BBStandards 3rdeditionDocument101 pagesDRAFT NABH BBStandards 3rdeditionGagan DudejaNo ratings yet
- List of Committees With Their Roles and Composition 1. Quality Improvement CommitteeDocument12 pagesList of Committees With Their Roles and Composition 1. Quality Improvement CommitteetanishaNo ratings yet
- Clinical Incident ReportDocument2 pagesClinical Incident ReportSooraj ThomasNo ratings yet
- Final Admission PolicyDocument6 pagesFinal Admission PolicytanishaNo ratings yet
- Standards For Accreditation of CLINICS Practicing Modern System of Medicine (Allopathy)Document80 pagesStandards For Accreditation of CLINICS Practicing Modern System of Medicine (Allopathy)shubham solankiNo ratings yet
- Himedia BGLB Broth 2% M121Document2 pagesHimedia BGLB Broth 2% M121grjhb100% (1)
- SOP For Dermatologist For DOH PuplicationDocument13 pagesSOP For Dermatologist For DOH Puplicationhitham shehataNo ratings yet
- Procedure(s) Guide Collection, Identification, Handling, Safe Transportation, Processing andDocument3 pagesProcedure(s) Guide Collection, Identification, Handling, Safe Transportation, Processing andVEEKU HOSPITALSNo ratings yet
- Clinical Competency ChecklistDocument9 pagesClinical Competency ChecklistSHAFIQNo ratings yet
- Sah-Lab: St. Andrew HospitalDocument2 pagesSah-Lab: St. Andrew HospitalRazel Ann ElagioNo ratings yet
- QA Policy ManualDocument65 pagesQA Policy Manualmba07-807No ratings yet
- Patient-And Family-Centered Care Organizational Self-Assessment ToolDocument3 pagesPatient-And Family-Centered Care Organizational Self-Assessment ToolAndi AbelloNo ratings yet
- Laboratory Quality Control A Complete Guide - 2020 EditionFrom EverandLaboratory Quality Control A Complete Guide - 2020 EditionNo ratings yet
- Application FormDocument1 pageApplication FormAglaia OrtileNo ratings yet
- Infectious APDocument7 pagesInfectious APNick ANo ratings yet
- English - Performance Task 1Document3 pagesEnglish - Performance Task 1Jeffrey LunaNo ratings yet
- PT2 - EnglishDocument2 pagesPT2 - EnglishJeffrey LunaNo ratings yet
- Passport ApplicationDocument1 pagePassport ApplicationJeffrey LunaNo ratings yet
- Jeffrey Vaccination CardDocument1 pageJeffrey Vaccination CardJeffrey LunaNo ratings yet
- Narrative Report On The Purchase of Drugs/Medicines and Medical Supplies From Gender and Development Fund For Sy 2021-2022Document2 pagesNarrative Report On The Purchase of Drugs/Medicines and Medical Supplies From Gender and Development Fund For Sy 2021-2022JAYSON BALINBINNo ratings yet
- Health and Safety Assurance Standards R4Document153 pagesHealth and Safety Assurance Standards R4besongNo ratings yet
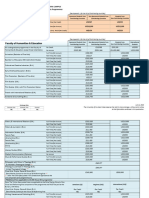
- UWI-Mona 2023-2024 Undergraduate Fee Schedule (June 2023)Document6 pagesUWI-Mona 2023-2024 Undergraduate Fee Schedule (June 2023)AnastasiaNo ratings yet
- Fowler, Gasiorek, & Giles (2015) - Don't Talk Yourself Into An Early Grave! The Role of Communication in Aging WellDocument2 pagesFowler, Gasiorek, & Giles (2015) - Don't Talk Yourself Into An Early Grave! The Role of Communication in Aging WellCraig FowlerNo ratings yet
- Provisional Bill: Multi Normal DischargeDocument3 pagesProvisional Bill: Multi Normal Dischargeparth dataNo ratings yet
- SerratiaDocument26 pagesSerratiaduverney.gaviriaNo ratings yet
- 2022 Year 10 Camp EXTREMEDocument11 pages2022 Year 10 Camp EXTREMEJohn BroughtonNo ratings yet
- Tugas Matriks JurnalDocument24 pagesTugas Matriks JurnalEti NurmahdaniNo ratings yet
- Mouth Preparation For RPDDocument45 pagesMouth Preparation For RPDArbaz SajjadNo ratings yet
- Aip Budget 2024 Needed DataDocument22 pagesAip Budget 2024 Needed Datamoox TVNo ratings yet
- Types of Cloud - 60589042Document1 pageTypes of Cloud - 60589042Violet ChertokNo ratings yet
- Ethics Review E1 FormDocument3 pagesEthics Review E1 FormShivali RS SrivastavaNo ratings yet
- Professional PracticeDocument7 pagesProfessional PracticeMQ SpotifyNo ratings yet
- Special Power of AttorneyDocument2 pagesSpecial Power of AttorneyCustodian Chase MegaNo ratings yet
- Hyperplast PC318 MSDS BH PDFDocument4 pagesHyperplast PC318 MSDS BH PDFShaik QutubuddinNo ratings yet
- Ozone Disco FireDocument2 pagesOzone Disco FireNoeme BaylonNo ratings yet
- Moxibustion OneSheetDocument1 pageMoxibustion OneSheetmatan sternNo ratings yet
- Atopic Dermatitis and Skin Microbiome Ne PDFDocument6 pagesAtopic Dermatitis and Skin Microbiome Ne PDFSmaranda ADNo ratings yet
- Back To Nature: The Selfie Generation Gets OutsideDocument154 pagesBack To Nature: The Selfie Generation Gets OutsideCansu CansuNo ratings yet
- Position Paper (Final)Document4 pagesPosition Paper (Final)Justin Marius DecierdoNo ratings yet
- Strategic Management (Assignment) HMSM 4032Document6 pagesStrategic Management (Assignment) HMSM 4032MOZAIDNo ratings yet
- Specifications For Neuropsychological Evaluations For Potential Neurocognitive ImpairmentDocument3 pagesSpecifications For Neuropsychological Evaluations For Potential Neurocognitive ImpairmentVoltha HerryNo ratings yet
- 4 Weeks To Total Posture & Spinal Mobility: Beginner - IntermediateDocument14 pages4 Weeks To Total Posture & Spinal Mobility: Beginner - Intermediate714 BaliNo ratings yet
- Social Taboos and Superstitions in Food Consumption During Pre and Post Natal Period of Tribal Women in Rayagada DistrictDocument3 pagesSocial Taboos and Superstitions in Food Consumption During Pre and Post Natal Period of Tribal Women in Rayagada DistrictRashmi MishraNo ratings yet
- Proofex Torchseal 3PDocument4 pagesProofex Torchseal 3PFZweiNo ratings yet
- Risk Factors For Pelvic Surgery: Y.E. Erata B. Kilic S. Güçlü U. Saygili T. UsluDocument5 pagesRisk Factors For Pelvic Surgery: Y.E. Erata B. Kilic S. Güçlü U. Saygili T. UsluGleiciane AguiarNo ratings yet
- Ota Go Correctional FacilityDocument14 pagesOta Go Correctional FacilityKier Marcial V. Collao IVNo ratings yet
- Department of Education: Republic of The PhilippinesDocument2 pagesDepartment of Education: Republic of The PhilippinesAnatasukiNo ratings yet