Professional Documents
Culture Documents
Jamaneurology Diener 2023 RV 220007 1677854360.36406
Jamaneurology Diener 2023 RV 220007 1677854360.36406
Uploaded by
Engr. Naveed MazharOriginal Description:
Original Title
Copyright
Share this document
Did you find this document useful?
Is this content inappropriate?
Report this DocumentCopyright:
Jamaneurology Diener 2023 RV 220007 1677854360.36406
Jamaneurology Diener 2023 RV 220007 1677854360.36406
Uploaded by
Engr. Naveed MazharCopyright:
Clinical Review & Education
JAMA Neurology | Review
Management of Trigeminal Autonomic Cephalalgias
Including Chronic Cluster
A Review
Hans Christoph Diener, MD; Cristina Tassorelli, MD; David W. Dodick, MD
IMPORTANCE Trigeminal autonomic cephalalgias (TACs) comprise a unique collection
of primary headache disorders characterized by moderate or severe unilateral pain, localized
in in the area of distribution of the first branch of the trigeminal nerve, accompanied by
cranial autonomic symptoms and signs. Most TACs are rare diseases, which hampers the
possibility of performing randomized clinical trials and large studies. Therefore, knowledge
of treatment efficacy must be based only on observational studies, rare disease registries,
and case reports, where real-world data and evidence play an important role in health
care decisions.
OBSERVATIONS Chronic cluster headache is the most common of these disorders, and the Author Affiliations: Institute for
Medical Informatics, Biometry and
literature offers some evidence from randomized clinical trials to support the use of Epidemiology (IMIBE), Department
pharmacologic and neurostimulation treatments. Galcanezumab, a monoclonal antibody of Neuroepidemiology, University
targeting the calcitonin gene-related peptide, was not effective at 3 months in a randomized Duisburg-Essen, Essen, Germany
(Diener); Department of Brain and
clinical trial but showed efficacy at 12 months in a large case series. For the other TACs (ie,
Behavioral Sciences, University of
paroxysmal hemicrania, hemicrania continua, short-lasting unilateral neuralgiform headache Pavia, Pavia, Italy (Tassorelli);
attacks with conjunctival injection and tearing, and short-lasting unilateral neuralgiform Headache Science &
headache attacks with cranial autonomic symptoms), only case reports and case series are Neurorehabilitation Centre, IRCCS C.,
Mondino Foundation, Pavia, Italy
available to guide physicians in everyday management.
(Tassorelli); Department of
Neurology, Mayo Clinic, Phoenix,
CONCLUSIONS AND RELEVANCE The accumulation of epidemiologic, pathophysiologic, natural
Arizona (Dodick); Atria Institute,
history knowledge, and data from case series and small controlled trials, especially over the New York, New York (Dodick).
past 20 years from investigators around the world, has added to the previously limited Corresponding Author: Hans
evidence and has helped advance and inform the treatment approach to rare TACs, which Christoph Diener, MD, Institute for
can be extremely challenging for clinicians. Medical Informatics, Biometry and
Epidemiology (IMIBE), Department
of Neuroepidemiology, University
JAMA Neurol. 2023;80(3):308-319. doi:10.1001/jamaneurol.2022.4804 Duisburg-Essen, Hufelandstrasse 55,
Published online January 17, 2023. 45147 Essen, Germany (hans.diener
@uk-essen.de).
T
rigeminal autonomic cephalalgias (TACs) are characterized isolated observations. Management recommendations are mostly
by the presence of autonomic accompanying symptoms based on results from patient series or case reports. Aiming on rare
during headache. The most frequently observed accom- TACS, we decided to report data on chronic cluster headache for
panying symptoms are rhinorrhoea, nasal congestion, conjunctival 2 reasons. First, episodic cluster headache was covered in several
injection, and lacrimation. In addition, patients may report edema recent reviews between 2018 and 2022.1-4 Second, data from the
of the eyelid, miosis, ptosis, redness of the face, and sweating of literature show that episodic and chronic cluster headache respond
the forehead and face. TACs are strictly unilateral headaches. TACs differently to treatments.5-7
include cluster headache, paroxysmal hemicrania, hemicrania con-
tinua, short-lasting unilateral neuralgiform headache attacks with
conjunctival injection and tearing (SUNCT), and short-lasting unilat-
Methods
eral neuralgiform headache attacks with cranial autonomic symp-
toms (SUNA). Most TACs can occur in an episodic or chronic form. A MEDLINE search in PubMed was performed from 2000 to 2022
The most important feature to differentiate between these entities for the terms cluster headache, paroxysmal hemicrania, hemicra-
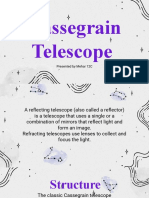
is the duration of the headache attack (Figure). nia continua, SUNCT, and SUNA. Search terms were epidemiology,
This review is dedicated to the management of rare TACs, and pathophysiology, clinical symptoms, management, and therapy.
we summarize the results from studies published in the last 20 For treatment and management, we selected articles reporting
years with a specific focus on research after 2018. Several thera- results from at least 10 patients. For the tables, we selected results
peutic approaches have been tested and proposed, based on the from review articles when only case reports with small numbers
putative mechanism of action of the drugs (Figure) or on previous were available.
308 JAMA Neurology March 2023 Volume 80, Number 3 (Reprinted) jamaneurology.com
© 2023 American Medical Association. All rights reserved.
Downloaded From: https://jamanetwork.com/ by a Zhejiang University Library User on 04/27/2023
Management of Trigeminal Autonomic Cephalalgias Including Chronic Cluster Review Clinical Review & Education
Figure. Phenotypic Spectrum and Treatment Targets for Trigeminal Autonomic Cephalalgias
A Differentiation of trigeminal-autonomic cephalalgias B Therapeutic approaches based on target structure and mechanism of action
Hemicrania continua
Continuous pain with exacerbations
10
Somatosensory cortex
Pain intensity
Pain signal processing
5
Thalamocortical
0 sensory processing
0 6 12 18 24
Therapy options
Time, h
• Topiramate
EX • Carbamazepine
Cluster headache RT
CO • Lamotrigine
Duration: 15-180 min (usually 30-60 min) L
A UM
R OS
Frequency: 0.5-8 per day (mean, 4 per day) B LL
E
CA
R
10
CE
S
U
P
Thalamus
Pain intensity
R
O
C
Pain signal processing
5
Hypothalamus
0 IN
6 60 120 180 240 300 360 Therapy options
A
M
R
Time, min LU • CGRP pathway
DB
L blockers
MI
E
B
• Verapamil
RE
Paroxysmal hemicrania
CE
Duration: 2-30 min (mean, 26 min)
• Steroids
PONS
Frequency: 5-40 per day (mean, 15 per day)
10
Superior salivary nucleus
Pain intensity
Origin of cranial autonomic symptoms
LA Connection to sphenopalatine ganglion
DUL
5
Therapy options
ME
Trigeminal nucleus • Vagal nerve stimulation
0 Trigeminovascular • Sphenopalatine ganglion stimulation
0 60 120 180 240 300 360 system • Indomethacin
Time, min Therapy options
• Topiramate
Trigeminocervical nucleus
SUNCT/SUNA • Carbamazepine
Duration: 5-600 s (usually 10-120 s; mean, 60 s) • COX inhibitors Convergence of upper cervical nerves
Frequency: 3-200 per day (mean, 28 per day) • OnabotulinumtoxinA (eg, greater occipital nerve) with
10 trigeminal nucleus
• Lidocaine
• CGRP pathway Therapy options
Pain intensity
blockers • Greater occipital nerve neuromodulation
5 • Indomethacin • Greater occipital nerve block (lidocaine)
0
0 6 12 18 24 30 36
Time, min
CGRP indicates calcitonin gene-related peptide; SUNA, short-lasting unilateral neuralgiform headache attacks with cranial autonomic symptoms; SUNCT, short-lasting
unilateral neuralgiform headache attacks with conjunctival injection and tearing.
as a disease. In a meta-analysis, pooled data showed a lifetime
Management of Chronic Cluster Headache prevalence of cluster headache of 124 per 100 000.10 Assuming
that about 10% of patients with cluster headache experience
Clinical Presentation chronic cluster headache, the prevalence is estimated to be 10 to
Cluster headache can manifest in 2 forms: episodic and chronic.8 15 per 100 000.
The definition of cluster headache as well as episodic and chronic
cluster were published by the International Headache Society.8 Treatment
For chronic cluster headache, attacks occur for more than 1 year The management of cluster headache is divided into the immedi-
without remission or with remission lasting less than 1 month. In ate treatment of attacks and the preventive treatment for reducing/
about 10% of patients with chronic cluster headache, the chronic stopping recurrence of attacks during the active periods. Most
pattern is present ab initio.9 In terms of nomenclature, a distinc- therapy recommendations are based on the results of open obser-
tion is made between a single cluster attack and cluster headache vational studies.
jamaneurology.com (Reprinted) JAMA Neurology March 2023 Volume 80, Number 3 309
© 2023 American Medical Association. All rights reserved.
Downloaded From: https://jamanetwork.com/ by a Zhejiang University Library User on 04/27/2023
Clinical Review & Education Review Management of Trigeminal Autonomic Cephalalgias Including Chronic Cluster
Table 1. Cluster Headache Attack Treatment
No. of Response No. of attacks
Treatment Dose Route Study patients rate, %a Placebo/sham, %b or end points
100% 7-12 Cohen et al15 76 78 20 150 Attacks
Oxygen Inhalation
L/min Dirkx et al16 55 68 NA 710 Attacks
Ekbom et al17 134 75 35 6 mg
Sumatriptan 3 or 6 mg Subcutaneous 80 12 mg
Hardebo and Dahlöf18 26 49 NA 62 Attacks
Hardebo and Dahlöf18 26 14 NA 52 Attacks
Schuh-Hofer et al19 10 50 NA 154 Attacks
Sumatriptan 20 mg Nasal spray
van Vliet et al14 118 47 18 Pain free at 15 min;
154 attacks
Cittadini et al20 92
5 mg 42 23 65 Attacks
10 mg 61 NA 63 Attacks
Rapoport et al21 52 151 Attacks
Zolmitriptan 5 or 10 mg Nasal spray 5 mg 50 30
10 mg 63 NA
Hedlund et al22 121 121 Attacks
5 mg 48 30
10 mg 63 NA
Three Silberstein et al23 133 27 15 NA
Transcutaneous
Vagus nerve consecutive
at the cervical Goadsby et al24 92 14 12 NA
stimulation 2-min
level
stimulations
Electrical Schoenen et al25 28 67 7 566 Attacks
stimulation
Electrode Goadsby et al26 93 62 39 992 Attacks
Stimulation of the parameters
implanted in the
sphenopalatine adjusted
pterygopalatine
ganglionc according to
fossa
provoked
paresthesias
b
Abbreviation: NA, not applicable. Placebo NA = no placebo group.
a c
Response rate for primary end point and number of attacks. No longer marketed.
Immediate Treatment of the Cluster Attack Noninvasive vagus nerve stimulation has been investigated both
Cluster attacks are quite short with a duration of 15 minutes to 180 for the immediate treatment and the prevention of cluster head-
minutes. Therefore, oral medications are not optimal because they ache. The 2 Acute Treatment of Cluster Headache (ACT1 and ACT2)
take too long to be effective. A very effective and adverse reaction– studies were prospective double-blind placebo-controlled random-
free therapy is the inhalation of oxygen, 100%, through a mask ized trials that investigated the gammaCore (electroCore) device.23,24
covering the mouth and nose in a sitting position. The efficacy of The ACT1 study showed a reduction in pain within 15 minutes in
this therapy was evaluated in a placebo-controlled trial.11 26.7% of patients with active stimulation compared with 15.1% with
Drug therapy for cluster attacks involves subcutaneous admin- sham stimulation.23 Vagus nerve stimulation was more effective
istration of sumatriptan or administration of sumatriptan or zolmi- than sham stimulation in the ACT2 study for the episodic cluster
triptan via the nasal spray modality. The efficacy of subcutaneous headache group with 48% of responders vs 6% in the sham arm
sumatriptan has been demonstrated in several placebo-controlled (P = .003). Sphenopalatine ganglion stimulation was developed for
trials. A meta-analysis found a rate of pain relief after 15 minutes of the treatment of acute cluster attacks and evaluated in 2 con-
48% with sumatriptan and 17% with placebo.12 Sumatriptan is well trolled studies.25,26 In the first study, a reduction in pain intensity
tolerated but is contraindicated in patients with clinically relevant within 15 minutes was achieved in 67% of attacks in the active stimu-
cardiovascular disease.13 lation group compared with 7% in the sham stimulation group. In
Results of randomized placebo-controlled trials are also avail- the second study, the proportion of attacks with relief of pain within
able for the administration of sumatriptan, 20 mg, as a nasal spray. 15 minutes was 62.5% (95% CI, 49.1%-74.1%) in the group with ac-
The rate of being pain free after 30 minutes was 47% for sumatrip- tive stimulation vs 38.9% (95% CI, 28.6%-56.2%) in the sham group.
tan and 18% for placebo.14 Intranasal administration of zolmitrip- Three of 36 patients experienced a serious adverse event during im-
tan in doses of 5 and 10 mg was studied in 2 randomized placebo- plantation (aspiration during intubation, nausea and vomiting, and
controlled trials. A meta-analysis of the studies with 121 patients venous injury or compromise). A fourth serious adverse event was
showed improvement of headache at 30 minutes after zolmitrip- an infection that was attributed to both the stimulation device and
tan, 10 mg, in 63% of patients; after zolmitriptan, 5 mg, in 48% of the implantation procedure. There are additional open studies sug-
patients; and, after placebo in 30% of patients (Table 1).15-22 gesting efficacy of sphenopalatine ganglion stimulation for the
310 JAMA Neurology March 2023 Volume 80, Number 3 (Reprinted) jamaneurology.com
© 2023 American Medical Association. All rights reserved.
Downloaded From: https://jamanetwork.com/ by a Zhejiang University Library User on 04/27/2023
Management of Trigeminal Autonomic Cephalalgias Including Chronic Cluster Review Clinical Review & Education
Table 2. Preventive Treatment of CCH
No. of
cluster
patients No. of
in the patients Response Placebo,
Treatment Dose Modality Study study with CCH rate, % % Outcome
NA Gabai and 48 15 69 NA Improved >75%
Spierings32
Verapamil 200-480 mg Oral Blau and Engel33 70 18 55 NA Complete relief
< or >500 mg Petersen et al34 400 146 23 NA >50% Attack reduction
Lithium 600-900 mg Oral Ekbom35 304 304 78 NA Chronic cluster headache
review article
Mathew et al36 12 3 0 NA Improvement
Láinez et al37 26 14 80 NA Cluster remission
Topiramate 100-200 mg Oral
Leone et al38 33 10 10 NA >50% Attack reduction
Huang et al39 12 1 100 NA Remission of headache
Leandri et al40 12 4 100 NA Cluster remission
Gabapentin 900 mg Oral
Schuh-Hofer et al41 8 8 75 NA Cluster remission
10 mg Leone et al42 20 2 50 NA % Attack reduction
Melatonin Oral
2 mg Pringsheim et al43 9 6 0 0 Add-on therapy
300 mg Subcutaneous Dodick et al6 237 237 32 27 >50% Responders at
week 3
Galcanezumab 300 mg Subcutaneous Riesenberg et al44 164 111 40 NA Open label: 50% very
much better or 29% much
better at 12 mo
Wilbrink et al45 131 NA 4.08 6.50 Reduction in weekly attack
frequency week 21-24
Aibar-Durán et al46 17 17 21 NA Mean reduction in number
of weekly attacks at 6 mo
Occipital nerve 100% Intensity Implanted Miller et al47 51 51 46 NA % Reduction in attack
stimulation vs 30% intensity electrodes frequency at 39 mo
Leplus et al48 105 105 69 NA Percentage >50%
responders at 44 mo
Fontaine et al49 13 13 68 NA % Reduction in attack
frequency at month 12
Jürgens et al28 31 31 35 NA Percentage of >50%
responders at month 24
Implanted Schoenen et al25 28 28 41 NA Percentage of >50%
SPG stimulation NA
electrode responders
Barloese et al29 85 78 55 NA Reduction in attacks/week
Computed NA Transcutaneous Xin et al50 10 10 100 NA Numeric rating scale
tomography–
guided
radiofrequency
thermocoagu-
lation of SPG
Vagus nerve Three 2-min Transcutaneous Gaul et al51 93 NA 40 8a Percentage of >50%
stimulation stimulations stimulation responders
twice daily
Abbreviations: CCH, chronic cluster headache; NA, not applicable; SPG, sphenopalatine ganglion.
a
Comparison with standard of care.
immediate treatment of cluster attacks (Table 1).27-29 In conclu- Prevention of Chronic Cluster Headache
sion, sphenopalatine ganglion stimulation has been shown to be All patients with chronic cluster headache should receive preven-
effective, but due to its invasive nature, it should be restricted to tive treatment. There are only very few randomized placebo-
patients in whom all other prophylactic medications to treat clus- controlled trials, mostly in episodic cluster headache. Most recom-
ter attacks failed. Sphenopalatine ganglion stimulation can be pro- mendations for treatment of chronic cluster headache are based on
posed only if the device and therapy receives regulatory approval case reports, small placebo-controlled studies, or open-label stud-
and there is certainty that the manufacturer will make the technol- ies (Table 2).32,33,36 A scoping review of the literature concluded that
ogy available and ensure maintenance.30,31 the quality of treatment studies in chronic cluster headache did not
In conclusion, the inhalation of oxygen, 100%, is a very effec- allow to perform a network meta-analysis.52 Several of the drugs
tive treatment of cluster attacks, devoid of adverse events. The most listed in Table 2 may induce adverse reactions, especially at the high-
effective immediate therapy is the subcutaneous administration est doses tested in the literature. This requires careful monitoring
of sumatriptan. of the patients to capture and address incident adverse events.
jamaneurology.com (Reprinted) JAMA Neurology March 2023 Volume 80, Number 3 311
© 2023 American Medical Association. All rights reserved.
Downloaded From: https://jamanetwork.com/ by a Zhejiang University Library User on 04/27/2023
Clinical Review & Education Review Management of Trigeminal Autonomic Cephalalgias Including Chronic Cluster
A meta-analysis of the 2 open-label studies investigating ver- chronic cluster headache who were randomized to receive either
apamil showed that 87% of patients either had complete elimina- 100% stimulus intensity (n = 65) or 30% stimulus intensity (n = 66).
tion of cluster attacks or a 50% or greater reduction in attack The median weekly attack frequency in the total population de-
frequency.53 The Danish Headache Center observed a 44% effi- creased from 15.75 attacks at baseline to 7.38 (2.50 to 18.50; P < .001)
cacy for the end point of more than 50% attack reduction in 146 in weeks 21 to 24. The most common adverse reactions were local
patients with chronic cluster headache.34 One underpowered study pain, wound healing disorders, local infections, neck stiffness, cable
compared lithium and placebo for the prevention of cluster at- breaks, and malfunction of the stimulator. The lack of a proper con-
tacks. The trial was terminated due to futility.54 Open and small stud- trol group and the absence of difference in the efficacy observed with
ies summarized by Ekbom35 observed a positive response to lithium the low- and high-intensity stimulations weakens the results.45
in about 75% of patients. A meta-analysis of 3 open studies with Several open studies investigated the efficacy of occipital nerve
a total of 103 patients found that lithium was effective in inducing stimulation in patients with chronic cluster headache (Table 2). The
cluster remission or reducing attack frequency by at least 50% in success rate measured by a reduction more than 50% in the fre-
77% of patients.53 In patients treated with lithium, plasma levels quency of cluster attacks per week or month ranged from 40% to
should be monitored on a regular basis due to the potential toxicity 70%.46-49,58,59
of the drug. A potential preventive effect has been suggested for spheno-
There are only open studies on topiramate for the prevention palatine ganglion stimulation in 2 long-term studies investigating
of cluster headache. Doses of topiramate ranged from 100 to 200 the efficacy of the procedure in the immediate treatment.25,28 One
mg daily, and due to the small patient numbers, efficacy cannot study investigated the long-term effects.29 Between 35% and 55%
be evaluated (Table 2). Gabapentin showed efficacy in 2 small of patients had a reduction in cluster attack frequency. However,
studies.40,41 Given the circadian rhythm of cluster attacks, melato- sphenopalatine ganglion stimulation is no longer available because
nin has also been studied for the prevention of cluster headache. In the company left the market. A small open study performed com-
a small randomized placebo-controlled trial of 20 patients, melato- puted tomography–guided radiofrequency thermocoagulation of
nin, 10 mg, was more effective than placebo over a 14-day period.42 the sphenopalatine ganglion in 10 patients with chronic cluster
The study had only 2 patients with chronic cluster headache. A study hedache.50 The authors claimed a positive treatment response in
with 6 patients showed no efficacy.43 all patients. Another treatment option is gamma knife radiosur-
Calcitonin gene-related peptide plays an important role not only gery of the trigeminal nerve or the sphenopalatine ganglion. A sys-
in the pathophysiology of migraine but also in cluster headache. Se- tematic review from 5 open studies and 48 patients reported a
rum levels of calcitonin gene-related peptide are elevated during meaningful pain reduction in 77%.60
cluster attacks.55 Galcanezumab, a monoclonal antibody targeting Noninvasive vagus nerve stimulation was examined as adjunc-
calcitonin gene-related peptide, was studied in episodic and chronic tive prophylactic treatment of chronic cluster headache in the PREVA
cluster headache.7 When tested in a subgroup of patients with trial.51 PREVA was a prospective, open-label, randomized study
chronic cluster headache, galcanezumab did not prove superior that compared adjunctive prophylactic noninvasive vagus nerve
to placebo.6 However, the study had a high placebo response. In stimulation (n = 48) with standard of care alone (n = 49). During
a long-term open-label safety study, 111 patients with chronic clus- the randomization phase, patients treated with standard of care plus
ter headache who participated in the placebo-controlled study noninvasive vagus nerve stimulation had a significantly greater re-
continued treatment with galcanezumab for 6 to 12 months. At duction in the number of attacks per week vs controls (−5.9 vs −2.1)
month 12, data from 79 patients were available, and 50% and 29% for a mean therapeutic gain of 3.9 fewer attacks per week (95% CI,
of these patients reported to be very much better or much better, 0.5-7.2; P = .02).
respectively.44 The most common adverse reactions were naso- The potential benefit of invasive stimulation of the posterior
pharyngitis and injection site pain.56 Galcanezumab was approved hypothalamus has been suggested in relatively large case series of
only for episodic cluster headache prevention in the US. A clinical patients with refractory chronic cluster headache, but the efficacy
trial evaluating the efficacy of fremanezumab for the prevention of was not confirmed in a randomized phase of a controlled study, al-
chronic cluster headache (NCT02964338) was terminated due to though a benefit was reported by 6 of 11 patients in the open-label
futility. Clinical trials evaluating eptinezumab for chronic cluster 10-month phase.61 In this study, there were 3 serious adverse events,
headache (NCT05064397) are ongoing. including subcutaneous infection, transient loss of consciousness,
and micturition syncope. Of note, in a previous open-label study,
Neurostimulation for the Preventive Treatment a fatal event occurred in 1 of the 6 patients who underwent the pro-
of Chronic Cluster Headache cedure. Because of the possible serious adverse events, invasive
Noninvasive and invasive methods of neurostimulation are used for stimulation of the posterior hypothalamus should only be consid-
patients with chronic cluster headache in whom drug therapy is not ered in cases of failure of all pharmacological preventive treat-
sufficiently effective or is not tolerated.57 ments, used also in combination, and the extracranial invasive or
Bilateral stimulation of the occipital nerve acts through both pe- noninvasive neurostimulation methods.62
ripheral and central mechanisms.1 For the procedure, stimulating
electrodes are placed subcutaneously over the occipital nerves. Elec- Conclusions and Future Treatment Concepts
trical stimulation is provided via an implantable pulse generator. The In conclusion, bilateral stimulation of the greater occipital nerve is
only randomized double-blind multicenter study conducted to date probably the most effective therapy in patients with chronic clus-
and to our knowledge to evaluate occipital nerve stimulation for clus- ter headache who do not tolerate treatment with verapamil or
ter headache prevention (ICON trial45) included 131 patients with lithium. However, the optimal parameters for stimulation have not
312 JAMA Neurology March 2023 Volume 80, Number 3 (Reprinted) jamaneurology.com
© 2023 American Medical Association. All rights reserved.
Downloaded From: https://jamanetwork.com/ by a Zhejiang University Library User on 04/27/2023
Management of Trigeminal Autonomic Cephalalgias Including Chronic Cluster Review Clinical Review & Education
yet been definitively determined. The failure of galcanezumab to Conclusion
show superiority over placebo for the preventive treatment of In conclusion, paroxysmal hemicrania is a TAC characterized by uni-
chronic cluster headache, despite efficacy being demonstrated in lateral and severe pain, predominantly located in the orbital region,
episodic cluster headache, has raised several questions about associated with cranial parasympathetic features. The attacks re-
differences in etiology, pathophysiology, and trial design.63,64 The spond completely to indomethacin. A few other treatment options
discrepancy between the results of the placebo-controlled study and are available for patients who cannot tolerate indomethacin.
the open long-term study might be due to the high placebo re-
sponse. Further research elucidating the reasons for what may be
a differential response to preventive treatments, and careful trial
Hemicrania Continua
designs in both patient populations are needed.
Ketamine, a noncompetitive N-methyl-D-aspartic acid recep- Clinical Presentation
tor antagonist, has been increasingly used in pain management in Hemicrania continua is a unilateral continuous headache. Pain is usu-
recent years. In a small study of 13 patients with chronic cluster head- ally described as dull and pressing, typically located in the tempo-
ache, low-dose intravenous ketamine was given every 2 weeks.65 ral, orbital, or frontal region, although sometimes it may be re-
Half of the patients had a reduction in the number of cluster at- ported in the retro-orbital, occipital, and parietal regions.87 Typically,
tacks. Pasireotide is a somatostatin analogue and was studied in a the continuous headache has superimposed exacerbations with stab-
double-blind placebo-controlled trial in patients with episodic or bing or pulling pain of moderate to severe intensity. The duration of
chronic cluster headache. The study was terminated early due to lack pain exacerbations varies markedly from a few seconds to days or
of efficacy (NCT02619617). OnabotulinumtoxinA has been evaluated even weeks.76 Accompanying the headache are autonomic symp-
in a small open-label study involving 17 patients with chronic cluster toms ipsilateral to the pain. The most important diagnostic feature
headache.66 The results obtained show that 59% of the study is the complete, although transient, response of the headache to
patients achieved the primary outcome measure represented therapeutic doses of indomethacin.8
by a more than 50% reduction in cumulative headache minutes.
Treatment
Recent advancements in treatment options for hemicrania conti-
nua have prompted the possibility to use either invasive or nonin-
Paroxysmal Hemicrania vasive approaches (Table 3). Indomethacin serves to confirm the
Clinical Presentation diagnosis,88 although cases of secondary hemicrania continua with
Paroxysmal hemicrania is characterized by severe short attacks of complete response to indomethacin have been reported.
head and facial pain with high frequency, averaging 10 attacks per Hemicrania continua does not necessarily respond immediately
day with a range between 5 to 40 attacks in 24 hours. Pain is asso- to therapy. In one case series, only 10% of patients showed a re-
ciated with autonomic symptoms or signs including lacrimation, sponse within 24 hours, whereas 43% of patients reported a com-
conjunctival injection, nasal congestion, and/or rhinorrhea. The plete response within 1 week and some patients might require up to
pain is unilateral, very rarely bilateral, and the attacks last 2 to 30 4 weeks.89,90 An interesting observation is that other nonsteroidal
minutes.67 The definition is provided by the International Head- anti-inflammatory drugs are much less effective than indomethacin.
ache Society.8 In preclinical models, data implicated a nitric oxide–related signaling
Paroxysmal hemicrania occurs in 2 subtypes: episodic and mechanism underlying the unique response to indomethacin.91
chronic.8 One of the clinical landmarks of paroxysmal hemicrania In patients who cannot tolerate indomethacin or have contra-
is the complete efficacy of indomethacin when taken regularly. indications to it, other drugs have been proposed in case reports
and open studies (Table 3). A positive treatment response has
Treatment been observed with the COX-2 inhibitor celecoxib, piroxicam, and
The attacks of paroxysmal hemicrania are too short for immediate topiramate.76,92 Topiramate can also be used in association to in-
drug therapy to be effective. Therefore, preventive therapy is rec- domethacin as a sparing agent of this latter.93 Melatonin (6-9 mg/d)
ommended (Table 3). The most effective treatment is indometha- was effective in a few patients in combination with indomethacin,77
cin. The dose is slowly increased from 25 mg 3 times per day to 150 allowing the reduction of indomethacin in half the patients.77 Posi-
mg per day. Higher doses, up to 300 mg daily, have also been re- tive case reports were also published for corticosteroids, high-
ported in the literature. For most patients, the maintenance dose is dose ibuprofen, aspirin, gabapentin, amitriptyline, acemethacin,
between 25 and 100 mg daily. After discontinuation of indometha- verapamil, and onabotulinumtoxinA (Table 3).76
cin, the symptoms of paroxysmal hemicrania usually return within Nerve blocks can be effective in hemicrania continua with
hours to days.68 Some patients are unable to take indomethacin a benefit that lasts up to 2 to 10 months. Blockade of the greater
long term because of gastrointestinal adverse reactions despite occipital or supraorbital nerves, alone or in combination, may be
taking proton pump inhibitors. considered.94 A crossover study and an open study in 16 patients
Single-case reports suggest the efficacy of COX-2 inhibitors, also reported a positive response to occipital nerve stimulation.95,96
topiramate, verapamil, and carbamazepine (Table 3). The efficacy A small case series with botulinum toxin showed a reduction of 50%
of blockade of the sphenopalatine ganglion, occipital nerve or more in moderate to severe headache days in 5 of 9 patients.78
stimulation,86 and neuromodulation with noninvasive stimulation Noninvasive vagus nerve stimulation was used in 9 patients with
of the vagus nerve with 2 consecutive 2-minute doses delivered hemicrania continua who could not tolerate indomethacin and
3 daily stimulations have been reported.74,75 induced a reduction in continuous pain.75
jamaneurology.com (Reprinted) JAMA Neurology March 2023 Volume 80, Number 3 313
© 2023 American Medical Association. All rights reserved.
Downloaded From: https://jamanetwork.com/ by a Zhejiang University Library User on 04/27/2023
Clinical Review & Education Review Management of Trigeminal Autonomic Cephalalgias Including Chronic Cluster
Table 3. Preventive Treatment of Paroxysmal Hemicrania, Hemicrania Continua, and SUNCT and SUNA
No. of Response Outcomes or
Treatment Dose Modality Study patients rate, % Placebo No. of publications
Paroxysmal hemicrania
25-150 mg Pareja et al68 10 100 Relief of symptoms
50-300 mg Cittadini et al69 31 96 Absolute response
50-225 mg Prakash et al70 17 100 Complete response
Indomethacin Oral NA
50-200 mg Boes and Dodick71 40 75 Data for 40 of 74 patients
2.75 mg/kg of Mauritz et al72 8 75 Pediatric patients
Body weight
Verapamil 250 mg Oral Baraldi et al73 30 47 NA 11 Publications
Carbamazepine 800 mg Oral Baraldi et al73 15 20 NA 6 Publications
Topiramate 50-200 mg Oral Baraldi et al73 12 75 NA 7 Publications
Kamourieh et al74 8 75 >50% Improvement
Two 2-min
Vagus nerve Tso et al75 6 75 Complete cessation to
stimulations Transcutaneous NA
stimulation decreased severity; 2
3 times/d
patients had no response
Hemicrania continua
Indomethacin 25-200 mg Oral Baraldi et al73 159 99 NA 55 Publications
Topiramate 100-200 mg Oral Prakash and Patel76 16 100 NA 7 Publications
Gabapentin 1600 mg Oral Baraldi et al73 13 85 NA 6 Publications
Melatonin 10 mg Oral Rozen77 11 45 NA <20% Pain freedom
OnabotulinumtoxinA 155 Injection Miller et al78 9 55 NA >50% Reduction in
headache days
73
COX-2 inhibitors NA Oral Baraldi et al 18 83 NA Celecoxib, piroxicam
Nerve blocksa Local anesthetic NA Baraldi et al73 32 72 NA NA
Neurostimulationb NA NA Baraldi et al73 14 86 NA NA
Vagus nerve 2 min 3 Times/d NA Trimboli et al79 4 60 NA NA
stimulation
SUNCT and SUNA
Lidocaine 1.3-3.3 mg/kg of Intravenous Marmura80 34 95 NA Short-term treatment;
Body weight 4 publications
Lambru et al81
SUNCT, 50-700 mg SUNCT 74 77 NA Improvement
SUNA 60 77
Weng et al82 Percentage with reduction
Lamotrigine Oral
in frequency and severity
SUNCT 29 62 NA of attacks
SUNA, 150-600 mg SUNA 16 31
Baraldi et al73 84 81 NA Percentage of responders;
21 studies
81
Lambru et al
SUNCT 48 54 NA Improvement
SUNA 31 35
Weng et al82
Topiramate 50-400 mg Oral Percentage with reduction
SUNCT 27 48 NA in frequency and severity
of attacks
SUNA 9 11
Baraldi et al73 36 56 NA Percentage of responders;
11 studies
Lambru et al81
SUNCT 50 32 NA Improvement
SUNA 30 33
Weng et al82
Gabapentin 300-3600 mg Oral Percentage with reduction
SUNCT 29 38 NA in frequency and severity
of attacks
SUNA 18 39
Baraldi et al73 48 59 NA Percentage of responders;
11 studies
Lambru et al81
Pregabalin 25-600 mg Oral SUNCT 37 32 NA Improvement
SUNA 29 31
(continued)
314 JAMA Neurology March 2023 Volume 80, Number 3 (Reprinted) jamaneurology.com
© 2023 American Medical Association. All rights reserved.
Downloaded From: https://jamanetwork.com/ by a Zhejiang University Library User on 04/27/2023
Management of Trigeminal Autonomic Cephalalgias Including Chronic Cluster Review Clinical Review & Education
Table 3. Preventive Treatment of Paroxysmal Hemicrania, Hemicrania Continua, and SUNCT and SUNA (continued)
No. of Response Outcomes or
Treatment Dose Modality Study patients rate, % Placebo No. of publications
Lambru et al81
SUNCT 44 38 NA Improvement
SUNA 43 63
Weng et al82
Carbamazepine 100-2000 mg Oral Percentage with reduction
SUNCT 43 36 NA in frequency and severity
of attacks
SUNA 20 20
Baraldi et al73 78 49 NA Percentage of responders;
27 studies
Lambru et al81
SUNCT 29 69 NA Improvement
SUNA 34 73
Oxcarbazepine 600-3600 mg Oral
Weng et al82
Percentage with reduction
SUNCT 7 14 NA in frequency and severity
of attacks
SUNA 6 0
Lambru et al81
Duloxetine 30-120 mg Oral SUNCT 20 60 NA Improvement
SUNA 17 35
Deep brain 185 Hz; amplitude, Stimulation Miller et al83 11 82 NA Percentage >50% reduction
stimulation 4 mV in attack frequency; median
follow-up, 29 mo
Greater occipital Methylprednisolone Local injection Lambru et al81 58 37 NA Improvement
nerve block and lidocaine, 2%
Occipital nerve Amplitude, Stimulation Miller et al84 31 77 NA Percentage >50% reduction
stimulation 0.3-3.15 V; in daily attacks; median
frequency, follow-up, 45 mo
60-130 Hz
Trigeminal NA Surgery Lambru et al85 47 79 NA 75%-100% Reduction in
microvascular weekly attack frequency
decompression
a
Abbreviations: NA, not applicable; SUNA, short-lasting unilateral neuralgiform Nerve blocks: supraorbital nerve block and occipital nerve block.
headache attacks with cranial autonomic symptoms; SUNCT, short-lasting b
Neurostimulation: occipital nerve stimulation.
unilateral neuralgiform headache attacks with conjunctival injection and tearing.
Conclusions fication of Headache Disorders.8 SUNCT is characterized by the si-
In conclusion, hemicrania continua requires an absolute response multaneous presence of conjunctival injection and lacrimation, while
to indomethacin, which can take several weeks to occur. Indometha- in SUNA, either 1 of the 2 symptoms is present. The frequency of daily
cin dose-sparing treatment options include melatonin and topira- pain attacks can be between 1 and 100 attacks, with the number vary-
mate, while extracranial nerve blocks can provide a sustained re- ing extremely from patient to patient. Sixty percent of all patients
sponse lasting months in some patients. have episodic SUNCT or SUNA with periods of pain-free weeks or
months and 40% have the chronic form.97 A certain degree of over-
lap exists between the clinical features of SUNCT/SUNA and trigemi-
nal neuralgia98 when considering the very high frequency and short
Short-Lasting Unilateral Neuralgiform
duration of attacks, the neuralgiform quality of the pain, and the lack
Headache Attacks of circadian rhythmicity. Furthermore, SUNCT and SUNA attacks may
Clinical Presentation be triggered by ipsilateral cutaneous or intraoral stimulations. This
This group of trigeminal autonomic cephalalgias refers to head- partial overlap is also found in the therapeutic options (see below).
ache occurring with daily attacks of moderate or severe unilateral
head pain, with orbital, supraorbital, temporal, and/or other trigemi- Treatment
nal distribution, lasting for 1 to 600 seconds and manifesting as single Individual attacks of SUNCT and SUNA are so short that immediate
stabs, series of stabs, or in a sawtooth pattern. Typical accompany- treatment is not useful. Preventive therapy is separated into short
ing symptoms include conjunctival injection, lacrimation, rhinor- term and long term (Table 3). In short-term prevention, a therapeu-
rhoea, nasal congestion, ptosis, and eyelid edema. Two subtypes are tic effect of intravenous lidocaine was observed over a period of up
known: SUNCT and SUNA. to 12 weeks.82,99 Sumatriptan, 6 mg, subcutaneous and intrave-
SUNCT and SUNA are rare primary headache syndromes. Af- nous dihydroergotamine, corticosteroids, indomethacin, and inha-
fected patients experience very frequent, brief attacks of head and lation of oxygen were not effective.82
facial pain combined with autonomic symptoms. The diagnostic cri- There are only observational studies on long-term prevention.
teria of SUNA and SUNCT are provided by the International Classi- The only placebo-controlled trial found a beneficial effect of topi-
jamaneurology.com (Reprinted) JAMA Neurology March 2023 Volume 80, Number 3 315
© 2023 American Medical Association. All rights reserved.
Downloaded From: https://jamanetwork.com/ by a Zhejiang University Library User on 04/27/2023
Clinical Review & Education Review Management of Trigeminal Autonomic Cephalalgias Including Chronic Cluster
Table 4. Priority of Treatments for Trigeminal Autonomic Cephalalgias
Chronic cluster headache Prevention
Priority Acute Paroxysmal Hemicrania
of treatment immediate Prevention hemicrania continua SUNCT/SUNA
First choice Oxygen Verapamil Indomethacin Indomethacin Lamotrigine
Second choice Sumatriptan Lithium Topiramate Topiramate Topiramate
(subcutaneous) Abbreviations: SUNA, short-lasting
Third choice Zolmitriptan Occipital nerve Verapamil Neurostimulation Carbamazepine unilateral neuralgiform headache
nasal spray stimulation, vagus attacks with cranial autonomic
nerve stimulation symptoms; SUNCT, short-lasting
Other possibly Vagus nerve Topiramate, Vagus nerve Gabapentin Occipital nerve unilateral neuralgiform headache
effective stimulation galcanezumab, stimulation stimulation attacks with conjunctival injection
options gabapentin and tearing.
ramate compared with placebo.82 Open-label studies found effi- Conclusions
cacy of lamotrigine (effectiveness, 62%) and topiramate (effective- In conclusion, SUNCT and SUNA are excruciating, unilateral, short-
ness, 48%) (Table 3).82 Other positive treatment results have been lasting periorbital paroxysms of pain with cranial autonomic
reported with gabapentin, carbamazepine, oxcarbazepine, du- features that occur between 1 to 100 times per day. Intravenous
loxetine, and zonisamide.73,81 In clinical practice, a combination of lidocaine can provide sustained relief for months, while placebo-
preventive medications is sometimes necessary. controlled efficacy exists for topiramate only. Lamotrigine and other
Among procedural treatments, efficacy of occipital nerve ma- anticonvulsants may be effective. When pharmacological treat-
jor blocks and infraorbital and supraorbital nerve blocks have been ments fail, surgical options in selected patients include occipital nerve
described.100 There are also positive therapeutic effects of micro- stimulation, microvascular decompression of the trigeminal nerve,
vascular decompression of the trigeminal nerve root101 that have gamma knife radiosurgery or pulsed radiofrequency of the spheno-
recently been confirmed in a larger population62 The largest study palatine ganglion, and deep brain stimulation.
so far was an uncontrolled open-label prospective single-center
study conducted between 2012 and 2020 to evaluate the efficacy
and safety of trigeminal microvascular decompression in refrac-
Conclusions and Future Directions
tory chronic SUNCT or SUNA in patients with magnetic resonance
imaging evidence of trigeminal neurovascular conflict ipsilateral to Recent progress has been made in our understanding of the epi-
the pain side.85 The study group consisted of 47 patients of whom demiology, pathogenesis, prognosis, and treatment of TACs. The
31 had SUNCT and 16 had SUNA. The mean postsurgery follow-up extreme severity of pain and the rare nature for chronic cluster
was 57 months. Postoperatively, 78.7% of patients obtained either headache, paroxysmal hemicranias, hemicrania continua, and
an excellent or a good response. SUNCT/SUNA has made controlled clinical trials a challenge and as
Stimulation of the greater occipital nerves seems also to be such, there is a less than robust evidence base that identifies the
effective.84 Seven of 9 patients treated with sphenopalatine gan- optimal first and second-line treatments for these disorders. Nev-
glion pulsed radiofrequency were considered responders.102 Miller ertheless, the accumulation of data from clinical case series
et al83 presented a case series of 11 patients treated with ventral teg- around the world has advanced our knowledge and provided guid-
mental area deep brain stimulation in an uncontrolled, open-label ance on appropriate treatments and management strategies
prospective observational study. The responder rate (defined as (Table 4). Further advances will require consortia of multiple cen-
at least a 50% improvement in daily attack frequency) was 82% ters participating in collaborative prospective patient registries
and 4 patients became pain free for prolonged periods of time. where standardized patient-level data are systematically collected
Initially, drug therapy should be proposed. If this is not effec- and sample sizes sufficient for proper controlled clinical treatment
tive or tolerated, neuromodulation procedures can be considered. trials are generated. However, the lack of a reliable biomarker of
The best data are available for bilateral chronic stimulation of the oc- disease, the difficulty in proper blinding, and ethical consider-
cipital nerve. If microvascular compression of the trigeminal nerve ations about stopping a potentially effective treatment in rare con-
in the posterior fossa is demonstrated on magnetic resonance angi- ditions may represent important limitations and undermine the
ography, microvascular decompression surgery may be considered. solidity of results.
ARTICLE INFORMATION study; serves on the editorial board of Cephalalgia, Italian Ministry of University, and the Migraine
Accepted for Publication: November 3, 2022. Lancet Neurology, and Drugs; and is a member of Research Foundation; is president of and serves on
the clinical trials committee of the International the clinical trials committee for the International
Published Online: January 17, 2023. Headache Society. Dr Tassorelli reported personal Headache Society; and serves on the editorial
doi:10.1001/jamaneurol.2022.4804 fees from AbbVie, Eli Lilly and Company, Novartis, boards of Cephalalgia and The Journal of Headache
Conflict of Interest Disclosures: Dr Diener Teva Pharmaceuticals, Lundbeck, Dompé, and and Pain. Dr Dodick reported personal fees from
reported personal fees from Eli Lilly and Company, WebMD; grants from AbbVie during the conduct AbbVie, Acorda, AEON, Alcobra, Alder, Allergan,
Lundbeck, Novartis, Pfizer, and Teva of the study; is principal investigator or collaborator American Academy of Neurology, Amgen, Arteaus,
Pharmaceuticals; other support from WebMD as in clinical trials sponsored by Alder, Eli Lilly and Atria Health, Autonomic Technologies, Axsome,
author; grants from the German Research Council, Company, IBSA, Novartis, and Teva Biocentric, Biohaven, Boston Scientific, Bristol
German Ministry of Education and Research, and Pharmaceuticals; grants from the European Myers Squibb, CapiThera, CC Ford West Group,
the European Union during the conduct of the Commission, the Italian Ministry of Health, the Cerecin, Ceruvia, Charleston Laboratories, Colucid,
316 JAMA Neurology March 2023 Volume 80, Number 3 (Reprinted) jamaneurology.com
© 2023 American Medical Association. All rights reserved.
Downloaded From: https://jamanetwork.com/ by a Zhejiang University Library User on 04/27/2023
Management of Trigeminal Autonomic Cephalalgias Including Chronic Cluster Review Clinical Review & Education
CoolTech Medical, CTRLM, Decision Resources, 2018;17(1):75-83. doi:10.1016/S1474-4422(17) study. J Headache Pain. 2018;19(1):94. doi:10.1186/
Dr Reddy’s–Promius Pharma, electroCore, Eli Lilly 30405-2 s10194-018-0917-4
and Company, eNeura, Equinox, Ethicon, Foresight, 2. Diener HC, May A. Drug treatment of cluster 17. Ekbom K, Monstad I, Prusinski A, Cole JA,
Genentech, GSK, Impax, Impel, Insys, IntraMed, headache. Drugs. 2022;82(1):33-42. doi:10.1007/ Pilgrim AJ, Noronha D; The Sumatriptan Cluster
Ispen, Labrys, Linpharma, Lundbeck, Magellan, s40265-021-01658-z Headache Study Group. Subcutaneous sumatriptan
MAP BioPharma, Medtronic, Merck, Neurolief, in the acute treatment of cluster headache: a dose
Nocira, Novartis, NuPathe, Oxford University Press, 3. Burish MJ, Rozen TD. Trigeminal autonomic
cephalalgias. Neurol Clin. 2019;37(4):847-869. comparison study. Acta Neurol Scand. 1993;88(1):
Perfood, Pfizer, Pieris, Praxis, Revance, SAGE 63-69. doi:10.1111/j.1600-0404.1993.tb04189.x
Publishing, Salvia, Satsuma, St Jude, Supernus, doi:10.1016/j.ncl.2019.07.001
Teva Pharmaceuticals, Theranica, Tonix, UpToDate, 4. Schindler EAD, Burish MJ. Recent advances 18. Hardebo JE, Dahlöf C. Sumatriptan nasal spray
Vedanta, Wiley Blackwell, WL Gore, Wolters Kluwer in the diagnosis and management of cluster (20 mg/dose) in the acute treatment of cluster
Health, Xenon, Xoc Pharmaceuticals, Zogenix, headache. BMJ. 2022;376:e059577. headache. Cephalalgia. 1998;18(7):487-489.
Zosano, and ZP Opco; grants and personal fees doi:10.1136/bmj-2020-059577 doi:10.1046/j.1468-2982.1998.1807487.x
from Cefaly, electroCore, Eli Lilly and Company, 5. de Coo IF, Marin JC, Silberstein SD, et al. 19. Schuh-Hofer S, Reuter U, Kinze S, Einhäupl KM,
Novartis, Merz Pharma, Teva Pharmaceuticals, Differential efficacy of non-invasive vagus nerve Arnold G. Treatment of acute cluster headache with
Specifar, Amgen, Biogen, and Genesis Pharma; stimulation for the acute treatment of episodic 20 mg sumatriptan nasal spray: an open pilot study.
personal fees and nonfinancial support from West and chronic cluster headache: a meta-analysis. J Neurol. 2002;249(1):94-99. doi:10.1007/
Virginia University Foundation, Canadian Headache Cephalalgia. 2019;39(8):967-977. doi:10.1177/ PL00007854
Society, Healthlogix, Universal Meeting 0333102419856607 20. Cittadini E, May A, Straube A, Evers S,
Management, WebMD/Medscape, Oregon Health Bussone G, Goadsby PJ. Effectiveness of
Science Center, Albert Einstein University, 6. Dodick DW, Goadsby PJ, Lucas C, et al.
Phase 3 randomized, placebo-controlled study intranasal zolmitriptan in acute cluster headache:
University of Toronto, Synergy, MedNet, Peer View a randomized, placebo-controlled, double-blind
Institute for Medical Education, Medicom, of galcanezumab in patients with chronic cluster
headache: results from 3-month double-blind crossover study. Arch Neurol. 2006;63(11):1537-1542.
Medlogix, Chameleon Communications, Academy doi:10.1001/archneur.63.11.nct60002
for Continued Healthcare Learning, Haymarket treatment. Cephalalgia. 2020;40(9):935-948.
Medical Education, Global Scientific doi:10.1177/0333102420905321 21. Rapoport AM, Mathew NT, Silberstein SD, et al.
Communications, Miller Medical, MeetingLogiX, 7. Goadsby PJ, Dodick DW, Leone M, et al. Zolmitriptan nasal spray in the acute treatment of
University of British Columbia, University of Trial of galcanezumab in prevention of episodic cluster headache: a double-blind study. Neurology.
Southern California, University of California cluster headache. N Engl J Med. 2019;381(2):132-141. 2007;69(9):821-826. doi:10.1212/01.wnl.
(Los Angeles), American Academy of Neurology, doi:10.1056/NEJMoa1813440 0000267886.85210.37
and Canadian Headache Society outside the 8. Headache Classification Committee of 22. Hedlund C, Rapoport AM, Dodick DW,
submitted work; nonfinancial support from Starr the International Headache Society (IHS) The Goadsby PJ. Zolmitriptan nasal spray in the acute
Clinical, International Headache Society, American International Classification of Headache Disorders, treatment of cluster headache: a meta-analysis of
Headache Society, American Brain Foundation, 3rd edition. Cephalalgia. 2018;38(1):1-211. two studies. Headache. 2009;49(9):1315-1323.
and American Migraine Foundation; a patent for doi:10.1177/0333102417738202 doi:10.1111/j.1526-4610.2009.01518.x
Wolters Kluwer with royalties paid, for Oxford 23. Silberstein SD, Mechtler LL, Kudrow DB, et al;
University Press with royalties paid, Cambridge 9. Giani L, Proietti Cecchini A, Leone M. Cluster
headache and risk of chronic transformation. Neurol ACT1 Study Group. Non-invasive vagus nerve
University Press with royalties paid, for botulinum stimulation for the acute treatment of cluster
toxin dosage regimen for chronic migraine Sci. 2020;41(suppl 2):497-498. doi:10.1007/
s10072-020-04674-1 headache: findings from the randomized,
prophylaxis (nonroyalty bearing) issued, and for double-blind, sham-controlled ACT1 study. Headache.
Synaquell (Precon Health) pending; research 10. Fischera M, Marziniak M, Gralow I, Evers S. 2016;56(8):1317-1332. doi:10.1111/head.12896
support from Department of Defense, National The incidence and prevalence of cluster headache:
Institutes of Health, Henry Jackson Foundation, a meta-analysis of population-based studies. 24. Goadsby PJ, de Coo IF, Silver N, et al; ACT2
Sperling Foundation, American Migraine Cephalalgia. 2008;28(6):614-618. doi:10.1111/j.1468- Study Group. Non-invasive vagus nerve stimulation
Foundation, and Patient-Centered Outcomes 2982.2008.01592.x for the acute treatment of episodic and chronic
Research Institute; leadership or fiduciary role in cluster headache: a randomized, double-blind,
11. Cohen AS, Mathura MS, Burns B, Goadsby PJ. sham-controlled ACT2 study. Cephalalgia. 2018;38
other board, society, committee or advocacy group, Randomized, double-blind placebo-controlled
paid or unpaid from American Migraine Foundation, (5):959-969. doi:10.1177/0333102417744362
trial of high-flow inhaled oxygen in acute cluster
American Brain Foundation, International headache. Cephalalgia. 2007;27:1188. 25. Schoenen J, Jensen RH, Lantéri-Minet M, et al.
Headache Society Global Patient Advocacy Stimulation of the sphenopalatine ganglion (SPG)
Coalition; stock options/shareholder/patents/board 12. Law S, Derry S, Moore RA. Triptans for acute for cluster headache treatment: pathway CH-1:
of directors from Aural Analytics, Axon cluster headache. Cochrane Database Syst Rev. a randomized, sham-controlled study. Cephalalgia.
Therapeutics, ExSano, Man and Science, Healint, 2013;2013(7):CD008042. doi:10.1002/14651858. 2013;33(10):816-830. doi:10.1177/0333102412473667
Theranica, Second Opinion/Mobile Health, Epien, CD008042.pub3
26. Goadsby PJ, Sahai-Srivastava S, Kezirian EJ,
Nocira, Matterhorn, Ontologics, King-Devick 13. Dodick D, Lipton RB, Martin V, et al; Triptan et al. Safety and efficacy of sphenopalatine
Technologies, Precon Health, AYYA Biosciences, Cardiovascular Safety Expert Panel. Consensus ganglion stimulation for chronic cluster headache:
and Atria Health; payment or honoraria for lectures, statement: cardiovascular safety profile of triptans a double-blind, randomised controlled trial. Lancet
presentations, and educational events from (5-HT agonists) in the acute treatment of migraine. Neurol. 2019;18(12):1081-1090. doi:10.1016/
Amgen, Novartis, Eli Lilly and Company, Teva Headache. 2004;44(5):414-425. doi:10.1111/j.1526- S1474-4422(19)30322-9
Pharmaceuticals, Allergan, AbbVie, Lundbeck, 4610.2004.04078.x
Biohaven, and Pfizer; and honoraria from Vector 27. Ansarinia M, Rezai A, Tepper SJ, et al.
14. van Vliet JA, Bahra A, Martin V, et al. Intranasal Electrical stimulation of sphenopalatine ganglion
Psychometric Group, Clinical Care Solutions, sumatriptan in cluster headache: randomized
CME Outfitters, Curry Rockefeller Group, for acute treatment of cluster headaches. Headache.
placebo-controlled double-blind study. Neurology. 2010;50(7):1164-1174. doi:10.1111/j.1526-4610.2010.
DeepBench, Global Access Meetings, 2003;60(4):630-633. doi:10.1212/01.WNL.
KLJ Associates, Academy for Continued 01661.x
0000046589.45855.30
Healthcare Learning, Majallin LLC, Medlogix 28. Jürgens TP, Barloese M, May A, et al.
Communications, MJH Lifesciences, Miller Medical 15. Cohen AS, Burns B, Goadsby PJ. High-flow Long-term effectiveness of sphenopalatine
Communications, and WebMD Health/Medscape. oxygen for treatment of cluster headache: ganglion stimulation for cluster headache.
a randomized trial. JAMA. 2009;302(22):2451-2457. Cephalalgia. 2017;37(5):423-434. doi:10.1177/
REFERENCES doi:10.1001/jama.2009.1855 0333102416649092
1. Hoffmann J, May A. Diagnosis, pathophysiology, 16. Dirkx THT, Haane DYP, Koehler PJ. Oxygen 29. Barloese M, Petersen A, Stude P, Jürgens T,
and management of cluster headache. Lancet Neurol. treatment for cluster headache attacks at different Jensen RH, May A. Sphenopalatine ganglion
flow rates: a double-blind, randomized, crossover stimulation for cluster headache, results from
jamaneurology.com (Reprinted) JAMA Neurology March 2023 Volume 80, Number 3 317
© 2023 American Medical Association. All rights reserved.
Downloaded From: https://jamanetwork.com/ by a Zhejiang University Library User on 04/27/2023
Clinical Review & Education Review Management of Trigeminal Autonomic Cephalalgias Including Chronic Cluster
a large, open-label European registry. J Headache 45. Wilbrink LA, de Coo IF, Doesborg PGG, et al; 58. Magis D, Gerardy PY, Remacle JM, Schoenen J.
Pain. 2018;19(1):6. doi:10.1186/s10194-017-0828-9 ICON study group. Safety and efficacy of occipital Sustained effectiveness of occipital nerve
30. Jürgens TP, Schoenen J, Rostgaard J, et al. nerve stimulation for attack prevention in medically stimulation in drug-resistant chronic cluster
Stimulation of the sphenopalatine ganglion in intractable chronic cluster headache (ICON): headache. Headache. 2011;51(8):1191-1201.
intractable cluster headache: expert consensus on a randomised, double-blind, multicentre, phase 3, doi:10.1111/j.1526-4610.2011.01973.x
patient selection and standards of care. Cephalalgia. electrical dose-controlled trial. Lancet Neurol. 59. Mueller O, Diener HC, Dammann P, et al.
2014;34(13):1100-1110. doi:10.1177/ 2021;20(7):515-525. doi:10.1016/S1474-4422(21) Occipital nerve stimulation for intractable chronic
0333102414530524 00101-0 cluster headache or migraine: a critical analysis of
31. May A. The need for continued care after 46. Aibar-Durán JA, Álvarez Holzapfel MJ, direct treatment costs and complications.
sponsor closure. Lancet Neurol. 2020;19(3):205. Rodríguez R, Belvis Nieto R, Roig Arnall C, Cephalalgia. 2013;33(16):1283-1291. doi:10.1177/
doi:10.1016/S1474-4422(20)30023-5 Molet Teixido J. Occipital nerve stimulation and 0333102413493193
deep brain stimulation for refractory cluster 60. Franzini A, Clerici E, Navarria P, Picozzi P.
32. Gabai IJ, Spierings EL. Prophylactic treatment headache: a prospective analysis of efficacy over
of cluster headache with verapamil. Headache. Gamma knife radiosurgery for the treatment of
time. J Neurosurg. Published online January 17, 2020. cluster headache: a systematic review. Neurosurg Rev.
1989;29(3):167-168. doi:10.1111/j.1526-4610.1989. doi:10.3171/2019.11.JNS192042
hed2903167.x 2022;45(3):1923-1931. doi:10.1007/s10143-021-
47. Miller S, Watkins L, Matharu M. Treatment of 01725-9
33. Blau JN, Engel HO. Individualizing treatment intractable chronic cluster headache by occipital
with verapamil for cluster headache patients. 61. Leone M. Deep brain stimulation in headache.
nerve stimulation: a cohort of 51 patients. Eur J Lancet Neurol. 2006;5(10):873-877. doi:10.1016/
Headache. 2004;44(10):1013-1018. doi:10.1111/j.1526- Neurol. 2017;24(2):381-390. doi:10.1111/ene.13215
4610.2004.04196.x S1474-4422(06)70575-0
48. Leplus A, Fontaine D, Donnet A, et al; 62. Coppola G, Magis D, Casillo F, et al.
34. Petersen AS, Lund N, Jensen RH, Barloese M. French ONS registry group. Long-term efficacy of
Real-life treatment of cluster headache in a tertiary Neuromodulation for chronic daily headache. Curr
occipital nerve stimulation for medically intractable Pain Headache Rep. 2022;26(3):267-278.
headache center: results from the Danish Cluster cluster headache. Neurosurgery. 2021;88(2):375-383.
Headache Survey. Cephalalgia. 2021;41(5):525-534. doi:10.1007/s11916-022-01025-x
doi:10.1093/neuros/nyaa373
doi:10.1177/0333102420970455 63. Dodick DW, Goadsby PJ, Ashina M, et al.
49. Fontaine D, Christophe Sol J, Raoul S, et al. Challenges and complexities in designing cluster
35. Ekbom K. Treatment of cluster headache: Treatment of refractory chronic cluster headache
clinical trials, design and results. Cephalalgia. 1995; headache prevention clinical trials: a narrative
by chronic occipital nerve stimulation. Cephalalgia. review. Headache. 2022;62(4):453-472.
15(suppl 15):33-36. 2011;31(10):1101-1105. doi:10.1177/0333102411412086 doi:10.1111/head.14292
36. Mathew NT, Kailasam J, Meadors L. Prophylaxis 50. Xin B, Xie K, Luo G, Yao M. Long-term
of migraine, transformed migraine, and cluster 64. Barloese MCJ, Beske RP, Petersen AS, Haddock
follow-up safety and effectiveness of CT-guided B, Lund N, Jensen RH. Episodic and chronic cluster
headache with topiramate. Headache. 2002;42(8): radiofrequency thermocoagulation of
796-803. doi:10.1046/j.1526-4610.2002.02183.x headache: differences in family history, traumatic
sphenopalatine ganglion in refractory headache head injury, and chronorisk. Headache. 2020;60
37. Láinez MJ, Pascual J, Pascual AM, Santonja JM, treatment. Pain Ther. 2022;11(3):1011-1023. (3):515-525. doi:10.1111/head.13730
Ponz A, Salvador A. Topiramate in the prophylactic doi:10.1007/s40122-022-00401-0
treatment of cluster headache. Headache. 2003;43 65. Moisset X, Giraud P, Meunier E, et al.
51. Gaul C, Diener HC, Silver N, et al; PREVA Study Ketamine-magnesium for refractory chronic cluster
(7):784-789. doi:10.1046/j.1526-4610.2003.03137.x Group. Non-invasive vagus nerve stimulation for headache: a case series. Headache. 2020;60(10):
38. Leone M, Dodick D, Rigamonti A, et al. PREVention and Acute treatment of chronic cluster 2537-2543. doi:10.1111/head.14005
Topiramate in cluster headache prophylaxis: an headache (PREVA): a randomised controlled study.
open trial. Cephalalgia. 2003;23(10):1001-1002. Cephalalgia. 2016;36(6):534-546. doi:10.1177/ 66. Lampl C, Rudolph M, Bräutigam E.
doi:10.1046/j.1468-2982.2003.00665.x 0333102415607070 OnabotulinumtoxinA in the treatment of refractory
chronic cluster headache. J Headache Pain. 2018;
39. Huang WY, Lo MC, Wang SJ, Tsai JJ, Wu HM. 52. Medrea I, Christie S, Tepper SJ, Thavorn K, 19(1):45. doi:10.1186/s10194-018-0874-y
Topiramate in prevention of cluster headache in Hutton B. Effects of acute and preventive therapies
the Taiwanese. Neurol India. 2010;58(2):284-287. for episodic and chronic cluster headache: 67. Degirmenci Y, Kececi H. Can paroxysmal
doi:10.4103/0028-3886.63784 a scoping review of the literature. Headache. 2022; hemicrania be bilateral? a case report. Neurol Sci.
62(3):329-362. doi:10.1111/head.14284 2016;37(8):1377-1378. doi:10.1007/s10072-016-
40. Leandri M, Luzzani M, Cruccu G, Gottlieb A. 2560-7
Drug-resistant cluster headache responding to 53. Pompilio G, Migliore A, Integlia D.
gabapentin: a pilot study. Cephalalgia. 2001;21(7): Systematic literature review and Bayesian network 68. Pareja JA, Caminero AB, Franco E, Casado JL,
744-746. doi:10.1046/j.1468-2982.2001.00260.x meta-analysis of episodic cluster headache drugs. Pascual J, Sánchez del Río M. Dose, efficacy and
Eur Rev Med Pharmacol Sci. 2021;25(3):1631-1640. tolerability of long-term indomethacin treatment
41. Schuh-Hofer S, Israel H, Neeb L, Reuter U, of chronic paroxysmal hemicrania and hemicrania
Arnold G. The use of gabapentin in chronic cluster doi:10.26355/eurrev_202102_24874
continua. Cephalalgia. 2001;21(9):906-910.
headache patients refractory to first-line therapy. 54. Steiner TJ, Hering R, Couturier EG, Davies PT, doi:10.1046/j.1468-2982.2001.00287.x
Eur J Neurol. 2007;14(6):694-696. doi:10.1111/j. Whitmarsh TE. Double-blind placebo-controlled
1468-1331.2007.01738.x trial of lithium in episodic cluster headache. 69. Cittadini E, Matharu MS, Goadsby PJ.
Cephalalgia. 1997;17(6):673-675. doi:10.1046/j.1468- Paroxysmal hemicrania: a prospective clinical study
42. Leone M, D’Amico D, Moschiano F, Fraschini F, of 31 cases. Brain. 2008;131(pt 4):1142-1155.
Bussone G. Melatonin versus placebo in the 2982.1997.1706673.x
doi:10.1093/brain/awn010
prophylaxis of cluster headache: a double-blind 55. Goadsby PJ, Edvinsson L. Human in vivo
pilot study with parallel groups. Cephalalgia. 1996; evidence for trigeminovascular activation in cluster 70. Prakash S, Belani P, Susvirkar A, Trivedi A,
16(7):494-496. doi:10.1046/j.1468-2982.1996. headache: neuropeptide changes and effects of Ahuja S, Patel A. Paroxysmal hemicrania:
1607494.x acute attacks therapies. Brain. 1994;117(Pt 3):427- a retrospective study of a consecutive series of
434. doi:10.1093/brain/117.3.427 22 patients and a critical analysis of the diagnostic
43. Pringsheim T, Magnoux E, Dobson CF, Hamel E, criteria. J Headache Pain. 2013;14(1):26.
Aubé M. Melatonin as adjunctive therapy in the 56. Láinez MJA, Schoenen J, Stroud C, et al. doi:10.1186/1129-2377-14-26
prophylaxis of cluster headache: a pilot study. Tolerability and safety of galcanezumab in patients
Headache. 2002;42(8):787-792. doi:10.1046/j.1526- with chronic cluster headache with up to 15 months 71. Boes CJ, Dodick DW. Refining the clinical
4610.2002.02181.x of galcanezumab treatment. Headache. 2022;62(1): spectrum of chronic paroxysmal hemicrania:
65-77. doi:10.1111/head.14234 a review of 74 patients. Headache. 2002;42(8):
44. Riesenberg R, Gaul C, Stroud CE, et al. 699-708. doi:10.1046/j.1526-4610.2002.02171.x
Long-term open-label safety study of 57. Vukovic Cvetkovic V, Jensen RH.
galcanezumab in patients with episodic or chronic Neurostimulation for the treatment of chronic 72. Mauritz MD, Enninger A, Wamsler C, Wager J,
cluster headache. Cephalalgia. 2022;42(11-12):1225- migraine and cluster headache. Acta Neurol Scand. Zernikow B. Long-term outcome of indomethacin
1235. doi:10.1177/03331024221103509 2019;139(1):4-17. doi:10.1111/ane.13034 treatment in pediatric patients with paroxysmal
318 JAMA Neurology March 2023 Volume 80, Number 3 (Reprinted) jamaneurology.com
© 2023 American Medical Association. All rights reserved.
Downloaded From: https://jamanetwork.com/ by a Zhejiang University Library User on 04/27/2023
Management of Trigeminal Autonomic Cephalalgias Including Chronic Cluster Review Clinical Review & Education
hemicrania: a case series. Children (Basel). 2021;8 placebo-controlled trial. Cephalalgia. 2018;38(9): continua: a report of 2 cases. Headache. 2019;59
(2):101. doi:10.3390/children8020101 1554-1563. doi:10.1177/0333102417739304 (3):444-445. doi:10.1111/head.13490
73. Baraldi C, Pellesi L, Guerzoni S, Cainazzo MM, 83. Miller S, Akram H, Lagrata S, Hariz M, Zrinzo L, 94. Guerrero AL, Herrero-Velázquez S, Peñas ML,
Pini LA. Therapeutical approaches to paroxysmal Matharu M. Ventral tegmental area deep brain et al. Peripheral nerve blocks: a therapeutic
hemicrania, hemicrania continua and short lasting stimulation in refractory short-lasting unilateral alternative for hemicrania continua. Cephalalgia.
unilateral neuralgiform headache attacks: a critical neuralgiform headache attacks. Brain. 2016;139(Pt 2012;32(6):505-508. doi:10.1177/
appraisal. J Headache Pain. 2017;18(1):71. 10):2631-2640. doi:10.1093/brain/aww204 0333102412439800
doi:10.1186/s10194-017-0777-3 84. Miller S, Watkins L, Matharu M. Long-term 95. Miller S, Watkins L, Matharu MS. Treatment of
74. Kamourieh S, Lagrata S, Matharu MS. follow up of intractable chronic short lasting intractable hemicrania continua by occipital nerve
Non-invasive vagus nerve stimulation is beneficial unilateral neuralgiform headache disorders treated stimulation. J Neurol Neurosurg Psychiatry. 2017;88
in chronic paroxysmal hemicrania. J Neurol with occipital nerve stimulation. Cephalalgia. (9):805-806. doi:10.1136/jnnp-2017-315747
Neurosurg Psychiatry. 2019;90(9):1072-1074. 2018;38(5):933-942. doi:10.1177/0333102417721716 96. Burns B, Watkins L, Goadsby PJ. Treatment of
doi:10.1136/jnnp-2018-319538 85. Lambru G, Lagrata S, Levy A, et al. Trigeminal hemicrania continua by occipital nerve stimulation
75. Tso AR, Marin J, Goadsby PJ. Noninvasive microvascular decompression for short-lasting with a bion device: long-term follow-up of a
vagus nerve stimulation for treatment of unilateral neuralgiform headache attacks. Brain. crossover study. Lancet Neurol. 2008;7(11):1001-1012.
indomethacin-sensitive headaches. JAMA Neurol. 2022;145(8):2882-2893. doi:10.1093/brain/awac109 doi:10.1016/S1474-4422(08)70217-5
2017;74(10):1266-1267. doi:10.1001/jamaneurol. 86. Miller S, Lagrata S, Watkins L, Matharu M. 97. Cohen AS, Matharu MS, Goadsby PJ.
2017.2122 Occipital nerve stimulation for medically refractory Short-lasting unilateral neuralgiform headache
76. Prakash S, Patel P. Hemicrania continua: chronic paroxysmal hemicrania. Headache. 2017;57 attacks with conjunctival injection and tearing
clinical review, diagnosis and management. J Pain Res. (10):1610-1613. doi:10.1111/head.13187 (SUNCT) or cranial autonomic features (SUNA)--
2017;10:1493-1509. doi:10.2147/JPR.S128472 87. Cittadini E, Goadsby PJ. Hemicrania continua: a prospective clinical study of SUNCT and SUNA.
77. Rozen TD. How effective is melatonin as a clinical study of 39 patients with diagnostic Brain. 2006;129(Pt 10):2746-2760. doi:10.1093/
a preventive treatment for hemicrania continua? implications. Brain. 2010;133(Pt 7):1973-1986. brain/awl202
a clinic-based study. Headache. 2015;55(3): doi:10.1093/brain/awq137 98. Lambru G, Matharu MS. SUNCT, SUNA and
430-436. doi:10.1111/head.12489 88. Mehta A, Chilakamarri P, Zubair A, Kuruvilla DE. trigeminal neuralgia: different disorders or variants
78. Miller S, Correia F, Lagrata S, Matharu MS. Hemicrania continua: a clinical perspective on of the same disorder? Curr Opin Neurol. 2014;27(3):
OnabotulinumtoxinA for hemicrania continua: open diagnosis and management. Curr Neurol Neurosci Rep. 325-331. doi:10.1097/WCO.0000000000000090
label experience in 9 patients. J Headache Pain. 2018;18(12):95. doi:10.1007/s11910-018-0899-2 99. Williams MH, Broadley SA. SUNCT and SUNA:
2015;16:19. doi:10.1186/s10194-015-0502-z 89. Prakash S, Golwala P. A proposal for revision clinical features and medical treatment. J Clin
79. Trimboli M, Al-Kaisy A, Andreou AP, Murphy M, of hemicrania continua diagnostic criteria based on Neurosci. 2008;15(5):526-534. doi:10.1016/j.jocn.
Lambru G. Non-invasive vagus nerve stimulation critical analysis of 62 patients. Cephalalgia. 2012;32 2006.09.006
for the management of refractory primary chronic (11):860-868. doi:10.1177/0333102412452043 100. Yalın OO, Uludüz D, Özge A. Peripheral nerve
headaches: a real-world experience. Cephalalgia. 90. Prakash S, Shah ND. Delayed response of blocks for the treatment of short-lasting unilateral
2017;333102417731349. doi:10.1177/ indomethacin in patients with hemicrania continua: neuralgiform headache with conjunctival injection
0333102417731349 real or phantom headache? Cephalalgia. 2010;30 and tearing (SUNCT) during pregnancy. Agri. 2018;
80. Marmura MJ. Intravenous lidocaine and (3):375-379. doi:10.1111/j.1468-2982.2009.01910.x 30(1):28-30. doi:10.5505/agri.2016.25991
mexiletine in the management of trigeminal 91. Summ O, Andreou AP, Akerman S, Holland PR, 101. Hassan S, Lagrata S, Levy A, Matharu M,
autonomic cephalalgias. Curr Pain Headache Hoffmann J, Goadsby PJ. Differential actions of Zrinzo L. Microvascular decompression or
Rep. 2010;14(2):145-150. doi:10.1007/s11916-010- indomethacin: clinical relevance in headache. Pain. neuromodulation in patients with SUNCT and
0098-6 2021;162(2):591-599. doi:10.1097/j.pain. trigeminal neurovascular conflict? Cephalalgia.
81. Lambru G, Stubberud A, Rantell K, Lagrata S, 0000000000002032 2018;38(2):393-398. doi:10.1177/0333102417735847
Tronvik E, Matharu MS. Medical treatment of 92. Fantini J, Koscica N, Zorzon M, Belluzzo M, 102. Ornello R, Palmisani S, Murphy M, Sacco S,
SUNCT and SUNA: a prospective open-label study Granato A. Hemicrania continua with visual aura Al-Kaisy A, Lambru G. Sphenopalatine ganglion
including single-arm meta-analysis. J Neurol successfully treated with a combination of pulsed radiofrequency for the treatment of
Neurosurg Psychiatry. 2021;92(3):233-241. indomethacin and topiramate. Neurol Sci. 2015;36 refractory chronic SUNCT and SUNA: a prospective
doi:10.1136/jnnp-2020-323999 (4):643-644. doi:10.1007/s10072-014-2036-6 case series. Headache. 2020;60(5):938-945.
82. Weng HY, Cohen AS, Schankin C, Goadsby PJ. doi:10.1111/head.13788
93. Prakash S, Rana K. Topiramate as an
Phenotypic and treatment outcome data on SUNCT indomethacin-sparing agent in hemicrania
and SUNA, including a randomised
jamaneurology.com (Reprinted) JAMA Neurology March 2023 Volume 80, Number 3 319
© 2023 American Medical Association. All rights reserved.
Downloaded From: https://jamanetwork.com/ by a Zhejiang University Library User on 04/27/2023
You might also like
- Advances in Diagnosis, Classification, Pathophysiology and Mannagement of Trigeminal Neuralgia PDFDocument13 pagesAdvances in Diagnosis, Classification, Pathophysiology and Mannagement of Trigeminal Neuralgia PDFSergio A SalgadoNo ratings yet
- Mini-Dungeon - HMD-005 The Temporal Clock TowerDocument5 pagesMini-Dungeon - HMD-005 The Temporal Clock TowerАлексей ЖуравлевNo ratings yet
- Pathophysiology of Migraine.5Document11 pagesPathophysiology of Migraine.5Bryan100% (1)
- Approach To Neurologic Infections.4 PDFDocument18 pagesApproach To Neurologic Infections.4 PDFosmarfalboreshotmail.comNo ratings yet
- Cluster Headache and Other Trigeminal Autonomic CephalalgiasDocument19 pagesCluster Headache and Other Trigeminal Autonomic CephalalgiasBryan100% (1)
- Autoimmune Axonal Neuropathies. 2023Document15 pagesAutoimmune Axonal Neuropathies. 2023Arbey Aponte PuertoNo ratings yet
- Cervical Artery Dissection.11Document26 pagesCervical Artery Dissection.11OTTO VEGA VEGANo ratings yet
- D1. Neurologic ExaminationDocument33 pagesD1. Neurologic ExaminationpancseszNo ratings yet
- Tac - Jama 2023Document12 pagesTac - Jama 2023donadoguillermoNo ratings yet
- REFERAT 1-S2.0-S1201971210023684-MainDocument14 pagesREFERAT 1-S2.0-S1201971210023684-MainVantyNo ratings yet
- 9.1 An Approach To Identifying Headache Patients That Require Neuroimaging (Curr, Inst and Pedagogy 2019)Document6 pages9.1 An Approach To Identifying Headache Patients That Require Neuroimaging (Curr, Inst and Pedagogy 2019)Katherine RodríguezNo ratings yet
- Do Not Copy: Headaches and Facial Pain in RhinologyDocument4 pagesDo Not Copy: Headaches and Facial Pain in RhinologyZauzaa NabilaNo ratings yet
- Vestibular Migraine An UpdateDocument15 pagesVestibular Migraine An UpdateSerdar MeteNo ratings yet
- Block Na Crise Aguda de EnxaquecaDocument8 pagesBlock Na Crise Aguda de EnxaquecaRoberta Lessa RibeiroNo ratings yet
- Fpsyg 12 664235Document9 pagesFpsyg 12 664235prof.psicomelanyNo ratings yet
- PARANEOPLASTICDocument8 pagesPARANEOPLASTICMuhammad Imran MirzaNo ratings yet
- Updates in The Diagnostic ApprDocument9 pagesUpdates in The Diagnostic ApprKenia Jazmin CervantesNo ratings yet
- Acute Metronidazole-Induced NeurotoxicityDocument7 pagesAcute Metronidazole-Induced Neurotoxicityveerraju tvNo ratings yet
- 3 Pitfals in Recognition and Management of Trigeminal Neuralgia 2020Document8 pages3 Pitfals in Recognition and Management of Trigeminal Neuralgia 2020Gabriela Elizabeth Gomez CardenasNo ratings yet
- Base Pra Revisao TdcsDocument7 pagesBase Pra Revisao TdcsHelena CysneirosNo ratings yet
- Association of Migraine With Patent Foramen Ovale Closure A Systematic Review and Meta-AnalysisDocument6 pagesAssociation of Migraine With Patent Foramen Ovale Closure A Systematic Review and Meta-AnalysisEndin Nokik StujannaNo ratings yet
- Clinical Description of Attack-Related Cognitive Symptoms in Migraine: A Systematic ReviewDocument16 pagesClinical Description of Attack-Related Cognitive Symptoms in Migraine: A Systematic ReviewLindenberger BoriszNo ratings yet
- Makalah Jurnal SensitivityDocument24 pagesMakalah Jurnal Sensitivityairin shabrinaNo ratings yet
- Bacterial Brain Abscess: An Outline For Diagnosis and ManagementDocument10 pagesBacterial Brain Abscess: An Outline For Diagnosis and ManagementWIWI HRNo ratings yet
- Brain Abscess in Pediatric Patients With Congenital Heart Disease: A Case Report and Review of The LiteratureDocument2 pagesBrain Abscess in Pediatric Patients With Congenital Heart Disease: A Case Report and Review of The LiteratureSannita Mayusda BadiriNo ratings yet
- Migraine Integrated Approaches To Clinical ManagementDocument14 pagesMigraine Integrated Approaches To Clinical ManagementJOHN ROMERO CEVALLOSNo ratings yet
- A Neuroscience Perspective of Physical Treatment of Headache and Neck PainDocument7 pagesA Neuroscience Perspective of Physical Treatment of Headache and Neck PainOcha24 TupamahuNo ratings yet
- Greater Occipital Nerve Block For Migraine Prophylaxis - Full Text View - ClinicalTrials - GovDocument10 pagesGreater Occipital Nerve Block For Migraine Prophylaxis - Full Text View - ClinicalTrials - Govkillingeyes177No ratings yet
- Current Epidemiological Trends of Brain Abscess: A Clinicopathological StudyDocument9 pagesCurrent Epidemiological Trends of Brain Abscess: A Clinicopathological StudyNur Fadhilah KusnadiNo ratings yet
- Biomedicines 11 00044 v3Document19 pagesBiomedicines 11 00044 v3mariel gonzalezNo ratings yet
- Empijem SinusaDocument4 pagesEmpijem SinusaIvan GalicNo ratings yet
- CephalgiaDocument24 pagesCephalgiaNurlita Ranti YulistyaNo ratings yet
- Acupuntura para EnxaquecaDocument9 pagesAcupuntura para EnxaquecaEsmeraldino NetoNo ratings yet
- AbcesoDocument2 pagesAbcesoRocio LedesmaNo ratings yet
- Diagnosis, Treatment and Follow-Up of The Carpal Tunnel Syndrome: A ReviewDocument10 pagesDiagnosis, Treatment and Follow-Up of The Carpal Tunnel Syndrome: A ReviewBogdan TudorNo ratings yet
- Original Research Paper General MedicineDocument10 pagesOriginal Research Paper General MedicineKriti KumariNo ratings yet
- Treatment of Medically Intractable Cluster Headache by Occipital Nerve Stimulation: Long-Term Follow-Up of Eight PatientsDocument8 pagesTreatment of Medically Intractable Cluster Headache by Occipital Nerve Stimulation: Long-Term Follow-Up of Eight PatientsareteusNo ratings yet
- Bevilaqua-Grossi Et Al. 2010 CephalalgiaDocument8 pagesBevilaqua-Grossi Et Al. 2010 Cephalalgiacris.endo.ceNo ratings yet
- Cluster Headache: Epidemiology, Pathophysiology, Clinical Features, and DiagnosisDocument6 pagesCluster Headache: Epidemiology, Pathophysiology, Clinical Features, and DiagnosisadindaNo ratings yet
- Steiner2010 PDFDocument14 pagesSteiner2010 PDFLilisNo ratings yet
- Original Papers: Bacterial Brain Abscess: Microbiological Features, Epidemiological Trends and Therapeutic OutcomesDocument9 pagesOriginal Papers: Bacterial Brain Abscess: Microbiological Features, Epidemiological Trends and Therapeutic OutcomesIqbal AbdillahNo ratings yet
- European Journal of Paediatric Neurology: SciencedirectDocument6 pagesEuropean Journal of Paediatric Neurology: Sciencedirectsergio cabreraNo ratings yet
- Tratamiento de La Neurocisticercosis Revision CritDocument9 pagesTratamiento de La Neurocisticercosis Revision CritKarem Santos HinostrozaNo ratings yet
- Alça VascularDocument10 pagesAlça Vascularceciliatigre10No ratings yet
- Multicenter, Prospective, Single Arm, Open Label, Observational Study of STMS For Migraine Prevention (ESPOUSE Study Starling2018Document11 pagesMulticenter, Prospective, Single Arm, Open Label, Observational Study of STMS For Migraine Prevention (ESPOUSE Study Starling2018CESAR AUGUSTO CARVAJAL RENDONNo ratings yet
- Headache 2: SeriesDocument9 pagesHeadache 2: SeriesAzam alausyNo ratings yet
- Migrain TreatmentDocument10 pagesMigrain TreatmentveNo ratings yet
- Surgical Management of Occipital Neuralgia A Systematic Review of The LiteratureDocument10 pagesSurgical Management of Occipital Neuralgia A Systematic Review of The Literatureosobucox1967No ratings yet
- Estenosis Sub 4Document12 pagesEstenosis Sub 4Nicolás HenaoNo ratings yet
- Ketamine Vs Haloperidol For Prevention of CognitivDocument8 pagesKetamine Vs Haloperidol For Prevention of CognitivSilvia MoraNo ratings yet
- Fneur 14 1193752Document10 pagesFneur 14 1193752Juliane Farinelli PanontinNo ratings yet
- Primer: Tension-Type HeadacheDocument21 pagesPrimer: Tension-Type HeadachefiqriNo ratings yet
- EANO Guideline On The Diagnosis and Management ofDocument14 pagesEANO Guideline On The Diagnosis and Management ofJames E. WalkerNo ratings yet
- Pharmacological Management of Painful Peripheral Neuropathies: A Systematic ReviewDocument14 pagesPharmacological Management of Painful Peripheral Neuropathies: A Systematic Reviewgck85fj8pnNo ratings yet
- Pyogenic Brain Abscess and Subdural Empyema: Presentation, Management, and Factors Predicting OutcomeDocument8 pagesPyogenic Brain Abscess and Subdural Empyema: Presentation, Management, and Factors Predicting OutcomedaniNo ratings yet
- J Pharep 2017 02 019Document8 pagesJ Pharep 2017 02 019Daniel Garcia del PinoNo ratings yet
- SodaPDF Converted AIAN 21 3Document11 pagesSodaPDF Converted AIAN 21 3adindaNo ratings yet
- Idsa NeurocisticercosisDocument27 pagesIdsa Neurocisticercosistucto849915No ratings yet
- 1 s2.0 S2352873718300350 MainDocument7 pages1 s2.0 S2352873718300350 Mainsolifugae123No ratings yet
- Stolovitzky Et Al 2021 Effect of Radiofrequency Neurolysis On The Symptoms of Chronic Rhinitis A Randomized ControlledDocument7 pagesStolovitzky Et Al 2021 Effect of Radiofrequency Neurolysis On The Symptoms of Chronic Rhinitis A Randomized ControlledfrischaNo ratings yet
- Journal Neurologi 2Document10 pagesJournal Neurologi 2fatya azaraNo ratings yet
- A Secured Botnet Prevention Mechanism For HTTP Flooding Based DDoS AttackDocument5 pagesA Secured Botnet Prevention Mechanism For HTTP Flooding Based DDoS AttackEngr. Naveed MazharNo ratings yet
- Yash ShuklaDocument22 pagesYash ShuklaEngr. Naveed MazharNo ratings yet
- Chap4a - Steady State Errors - ELE353 - Spr21Document23 pagesChap4a - Steady State Errors - ELE353 - Spr21Engr. Naveed MazharNo ratings yet
- Chap5a Stability Analysis - ELE353 - Spr21Document4 pagesChap5a Stability Analysis - ELE353 - Spr21Engr. Naveed MazharNo ratings yet
- Evaluation of The Innovative Value Proposition For The Rail Freight Transport: An Integrated Dematel-Anp ApproachDocument27 pagesEvaluation of The Innovative Value Proposition For The Rail Freight Transport: An Integrated Dematel-Anp ApproachEngr. Naveed MazharNo ratings yet
- 4 Your Design Case StudyDocument9 pages4 Your Design Case StudyEngr. Naveed MazharNo ratings yet
- 1 s2.0 S1059056022000685 MainDocument16 pages1 s2.0 S1059056022000685 MainEngr. Naveed MazharNo ratings yet
- 10 Further Investigation and More On Final ReportDocument26 pages10 Further Investigation and More On Final ReportEngr. Naveed MazharNo ratings yet
- Chap5b - Routh Stability Analysis - ELE353 - Spr21Document25 pagesChap5b - Routh Stability Analysis - ELE353 - Spr21Engr. Naveed MazharNo ratings yet
- Chap4b Control Actions - ELE353 - Spr21Document20 pagesChap4b Control Actions - ELE353 - Spr21Engr. Naveed MazharNo ratings yet
- 6 Digital Controller DesignDocument23 pages6 Digital Controller DesignEngr. Naveed MazharNo ratings yet
- Fault Tolerant Flight Control Using Sliding Modes and Subspace Identification-Based Predictive ControlDocument21 pagesFault Tolerant Flight Control Using Sliding Modes and Subspace Identification-Based Predictive ControlEngr. Naveed MazharNo ratings yet
- Matlab: All All LongDocument5 pagesMatlab: All All LongEngr. Naveed MazharNo ratings yet
- Outdated Example For Previous Version of Supplied SchematicDocument2 pagesOutdated Example For Previous Version of Supplied SchematicEngr. Naveed MazharNo ratings yet
- Wheel Slip Control For The Electric Vehicle With IDocument9 pagesWheel Slip Control For The Electric Vehicle With IEngr. Naveed MazharNo ratings yet
- For (0.1,0.2,0.4,0.6,0.8,1) The ARL Chart Is As FollowsDocument5 pagesFor (0.1,0.2,0.4,0.6,0.8,1) The ARL Chart Is As FollowsEngr. Naveed MazharNo ratings yet
- State Space Equations - Pole Assignment by State Feedback - Observer DesignDocument27 pagesState Space Equations - Pole Assignment by State Feedback - Observer DesignEngr. Naveed MazharNo ratings yet
- ListDocument2 pagesListEngr. Naveed MazharNo ratings yet
- Lec03 MotorControlDocument45 pagesLec03 MotorControlEngr. Naveed MazharNo ratings yet
- HW1Document4 pagesHW1Engr. Naveed MazharNo ratings yet
- ECE 106: Digital Computer LabDocument6 pagesECE 106: Digital Computer LabEngr. Naveed MazharNo ratings yet
- Drive Calculator - DCbaseDocument1 pageDrive Calculator - DCbaseEngr. Naveed MazharNo ratings yet
- List of Designated Branches HBLDocument1 pageList of Designated Branches HBLEngr. Naveed MazharNo ratings yet
- In This Report We Have Deal With Stability in Aircraft by Auto Control System and Also by Using Pilot Stick ControlDocument12 pagesIn This Report We Have Deal With Stability in Aircraft by Auto Control System and Also by Using Pilot Stick ControlEngr. Naveed MazharNo ratings yet
- EE 4313 Homework 02 - 2Document1 pageEE 4313 Homework 02 - 2Engr. Naveed MazharNo ratings yet
- Starkville Dispatch Eedition 5-20-20 CORRDocument16 pagesStarkville Dispatch Eedition 5-20-20 CORRThe DispatchNo ratings yet
- Herbert SpencerDocument1 pageHerbert Spencerng kamchungNo ratings yet
- Green Light HPS Laser Operator ManualDocument81 pagesGreen Light HPS Laser Operator ManualPhillip V Mitchell0% (1)
- Cassegrain Telescope: Presented by Mehar 12CDocument10 pagesCassegrain Telescope: Presented by Mehar 12CMehar FathimaNo ratings yet
- Pink Floyd - LyricsDocument97 pagesPink Floyd - LyricsИван ВащенкоNo ratings yet
- Parkin Econ SM CH30 GeDocument22 pagesParkin Econ SM CH30 GeMuri SetiawanNo ratings yet
- The Incredible Analysis of W D GannDocument79 pagesThe Incredible Analysis of W D GannJohn Kent97% (31)
- Ncert Solutions Class 12 Accountancy Part 2 Chapter 1 Accounting For Share CapitalDocument42 pagesNcert Solutions Class 12 Accountancy Part 2 Chapter 1 Accounting For Share CapitalcchendrimadaNo ratings yet
- Filtrec F040 SeriesDocument8 pagesFiltrec F040 Serieshkhan10No ratings yet
- Applied Physics On Spectros PDFDocument71 pagesApplied Physics On Spectros PDFKaskus FourusNo ratings yet
- HIRARC FormDocument43 pagesHIRARC FormFachri Hidayat50% (2)
- Voltage Regulation Performance of Smart Inverters: Power Factor Versus Volt-VAR ControlDocument6 pagesVoltage Regulation Performance of Smart Inverters: Power Factor Versus Volt-VAR ControllucasNo ratings yet
- Toxicon: Tamara Sajevic, Adrijana Leonardi, Igor Kri ZajDocument19 pagesToxicon: Tamara Sajevic, Adrijana Leonardi, Igor Kri Zajaulia rahmahNo ratings yet
- Guda Guda Honnouji Rerun FAQDocument7 pagesGuda Guda Honnouji Rerun FAQRufus LoackerNo ratings yet
- Module 17 TAI - TC.MTO Basic Knowledge Examination Summary DataDocument27 pagesModule 17 TAI - TC.MTO Basic Knowledge Examination Summary DataChatchai PrasertsukNo ratings yet
- Lecture 5 PDFDocument8 pagesLecture 5 PDFMuhammad Hamza EjazNo ratings yet
- PR 2001219Document10 pagesPR 2001219Amr Mohamed GalalNo ratings yet
- Gammagard Us PiDocument4 pagesGammagard Us Pibmartindoyle6396No ratings yet
- Adc March 2018 SolvedDocument73 pagesAdc March 2018 SolvedKish BNo ratings yet
- Igcse Economics Rev NotesDocument69 pagesIgcse Economics Rev Noteskityk60% (5)
- FortiOS 7.0.1 CLI ReferenceDocument1,751 pagesFortiOS 7.0.1 CLI ReferenceMoacir Nunes NetoNo ratings yet
- 20 - Feb - 2019 - 170439480IDKL5X0QAnnexPFRDocument44 pages20 - Feb - 2019 - 170439480IDKL5X0QAnnexPFRGavoutha BisnisNo ratings yet
- Lesson Plan - 2 1Document20 pagesLesson Plan - 2 1api-311773794No ratings yet
- CCE Quiz Batasan Set - SolutionDocument4 pagesCCE Quiz Batasan Set - SolutionJoovs JoovhoNo ratings yet
- 26 32LC2R-TJDocument45 pages26 32LC2R-TJJens Enoch-LarsenNo ratings yet
- Final Sample Report of Maruti Car CompanyDocument69 pagesFinal Sample Report of Maruti Car Companyofficial vrNo ratings yet
- Waste Heat Boiler Deskbook PDFDocument423 pagesWaste Heat Boiler Deskbook PDFwei zhou100% (1)
- Reverse CalculationDocument7 pagesReverse CalculationKanishka Thomas Kain100% (1)
- Transducers & Isolators: TR - IsoDocument1 pageTransducers & Isolators: TR - IsoManikandan B100% (1)