Download as xlsx, pdf, or txt
You might also like
- Nbme 30 2021 ADocument200 pagesNbme 30 2021 AUsama Bilal100% (3)
- Best of Five For Dentistry PDFDocument165 pagesBest of Five For Dentistry PDFasraf amirullah67% (3)
- Dental Health CardDocument3 pagesDental Health Cardodessa delos santos100% (1)
- Oral Health Examination Record For Teachers and Non-Teaching PersonnelDocument3 pagesOral Health Examination Record For Teachers and Non-Teaching PersonnelDaisy's Home Cooking100% (6)
- Health Card ElemDocument4 pagesHealth Card ElemBernadette Sambrano EmbienNo ratings yet
- HEALTH CARD CorrectedDocument3 pagesHEALTH CARD CorrectedJoan A. DagdagNo ratings yet
- ITR DentalDocument3 pagesITR Dentalnelmark.pepitoNo ratings yet
- Case History DetailDocument4 pagesCase History DetailNid MadanNo ratings yet
- Oral Health Examination RecordDocument2 pagesOral Health Examination Recordeugene.camahinNo ratings yet
- Oral Health Examination RecordDocument1 pageOral Health Examination RecordJefrey N. Gonzales100% (1)
- Oral HProfile T&NTPDocument1 pageOral HProfile T&NTPMaria Fatima ArnaizNo ratings yet
- Dental Examination Record FormDocument2 pagesDental Examination Record FormHannah Naki Medina0% (1)
- Oral Health Examination Record For TNTPDocument1 pageOral Health Examination Record For TNTPJellyn Cadorna100% (1)
- Dental Examination Record FormDocument2 pagesDental Examination Record FormNinoslav MladenovicNo ratings yet
- Dental Examination Record FormDocument2 pagesDental Examination Record FormNurse AnnNo ratings yet
- Greetings: Pushpagiri College of Dental SciencesDocument27 pagesGreetings: Pushpagiri College of Dental SciencesDilu DavisNo ratings yet
- SHN Form 001 School Health Examination Card ElementaryDocument2 pagesSHN Form 001 School Health Examination Card ElementaryJohn BunayNo ratings yet
- Oral Health Examination Record For Teaching and Non Teaching PersonnelDocument1 pageOral Health Examination Record For Teaching and Non Teaching PersonnelAda RicanaNo ratings yet
- Div Pupils Dental Health CardDocument1 pageDiv Pupils Dental Health CardArexelle Martel EsmaNo ratings yet
- Health Inspection Examination Record.2019Document9 pagesHealth Inspection Examination Record.2019Quennie Edisan MigabonNo ratings yet
- Display PSFItemDocument1 pageDisplay PSFItemjamesjohnsonamazonprimeNo ratings yet
- Department of Education: Republic of The PhilippinesDocument1 pageDepartment of Education: Republic of The PhilippinesLicca ArgallonNo ratings yet
- GR 8-10 AJHS Dental Exam FormDocument1 pageGR 8-10 AJHS Dental Exam FormGeneral KevinNo ratings yet
- School Health Examination Card: Nutritional Status (NS) (BMI/Weight-for-Age)Document4 pagesSchool Health Examination Card: Nutritional Status (NS) (BMI/Weight-for-Age)April Rose CaballeroNo ratings yet
- QBANK PasTest Best of Fives For DentistryDocument165 pagesQBANK PasTest Best of Fives For DentistrylindajenhaniNo ratings yet
- Cleft Lip and PalateDocument77 pagesCleft Lip and PalateDr. Aysha SadafNo ratings yet
- Punjab Health Sector Reforms ProgramDocument1 pagePunjab Health Sector Reforms ProgramAasir NaQviNo ratings yet
- DentalAssistantHealthFormDocument4 pagesDentalAssistantHealthFormcr littleNo ratings yet
- Original Research: Revalence and Predictors of Dental Erosion in School Children of Karachi PakistanDocument5 pagesOriginal Research: Revalence and Predictors of Dental Erosion in School Children of Karachi PakistanAamir BugtiNo ratings yet
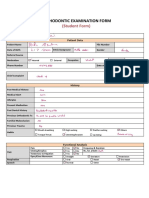
- Ortho Examinathion Form Students Copy Cast AnalysisDocument5 pagesOrtho Examinathion Form Students Copy Cast AnalysisAseel RoziNo ratings yet
- 2018 Introduction To CourseDocument54 pages2018 Introduction To CoursemorfisstefNo ratings yet
- ArticleDocument9 pagesArticleshrk2w4jqhNo ratings yet
- Of Dental Sciences: Original ArticleDocument4 pagesOf Dental Sciences: Original ArticleIntan Nur FajriNo ratings yet
- Saudi Dental Patients Attitude Towards Esthetic Dental Treatment at Ksu, College of Dentistry, RiyadhDocument4 pagesSaudi Dental Patients Attitude Towards Esthetic Dental Treatment at Ksu, College of Dentistry, RiyadhSARA BUARISHNo ratings yet
- Non Carious LesionsDocument70 pagesNon Carious LesionsSayak GuptaNo ratings yet
- Prescott Cosmetic Dentist Prescott Cosmetic DentistDocument54 pagesPrescott Cosmetic Dentist Prescott Cosmetic DentistDavid HerbertNo ratings yet
- Oligodontia: A Case Report: Fatma Ünalan / Is in Ulukapi / Juliana BakirgilDocument4 pagesOligodontia: A Case Report: Fatma Ünalan / Is in Ulukapi / Juliana BakirgilfatimahNo ratings yet
- Dental BHSS 2019Document1 pageDental BHSS 2019roulette laypNo ratings yet
- Health Card FrontDocument3 pagesHealth Card FrontCarlaGomezNo ratings yet
- 2 4th 2018Document9 pages2 4th 2018Oke Soe MoeNo ratings yet
- West Indian Med J 2007 56 (1) : 96Document3 pagesWest Indian Med J 2007 56 (1) : 96Alung Aya KalolaNo ratings yet
- Dental Health Program - Department of Health Website PDFDocument10 pagesDental Health Program - Department of Health Website PDFLeiNo ratings yet
- ArticuloDocument4 pagesArticuloanaNo ratings yet
- Bhola 2015Document12 pagesBhola 2015Maitee MoreiraNo ratings yet
- (CR) Early Childhood Caries A Case Report of An Extensive Rehabilitation (2018)Document3 pages(CR) Early Childhood Caries A Case Report of An Extensive Rehabilitation (2018)MuabhiNo ratings yet
- Praxtical Exam 2022 Ideal MorningDocument2 pagesPraxtical Exam 2022 Ideal MorningMarwan AlamriNo ratings yet
- Dental Caries: Prediction of Dental Caries Among Children of Different Age Groups Using Machine LearningDocument24 pagesDental Caries: Prediction of Dental Caries Among Children of Different Age Groups Using Machine LearningVaishali S.cNo ratings yet
- Dental FormDocument1 pageDental FormnebrejakayeannvillelaNo ratings yet
- 2019 Dent4060Document10 pages2019 Dent4060Jason JNo ratings yet
- INTRODUCTIONDocument18 pagesINTRODUCTIONAyeshaNo ratings yet
- Dentistry 101Document141 pagesDentistry 101bitiashvilinatiaNo ratings yet
- 2 History and ExaminationDocument55 pages2 History and Examinationsamar yousif mohamedNo ratings yet
- DPH Form 3300 PDFDocument2 pagesDPH Form 3300 PDFtomtranNo ratings yet
- Early Childhood Caries, Rampant, Chronic and Arrested CariesDocument28 pagesEarly Childhood Caries, Rampant, Chronic and Arrested CariesDrBhawna AroraNo ratings yet
- Prosthetic Treatments For Patients With Ectodermal DysplasiaDocument5 pagesProsthetic Treatments For Patients With Ectodermal DysplasiaJawad TariqNo ratings yet
- Shiv Rathod Pedo Case HistoryDocument9 pagesShiv Rathod Pedo Case HistoryRitvik RanaNo ratings yet
- Evaluation of The Effects of Different Remineralisation Agents On Initial Enamel Lesions by Scanning Electron Microscope and Energy Distributed X Ray Analysis - En.esDocument9 pagesEvaluation of The Effects of Different Remineralisation Agents On Initial Enamel Lesions by Scanning Electron Microscope and Energy Distributed X Ray Analysis - En.esAreli BetancourtNo ratings yet
- DIY Oral Hygiene: Achieve Clean, White Teeth and Healthy Gums with This Do-It-Yourself Mouth Care RoutineFrom EverandDIY Oral Hygiene: Achieve Clean, White Teeth and Healthy Gums with This Do-It-Yourself Mouth Care RoutineNo ratings yet
- 20180719Document3 pages20180719uxia merinoNo ratings yet
- Surgical Instruments: Grasping and Clamping Retracting Cutting and Dissecting Probing and DilatingDocument22 pagesSurgical Instruments: Grasping and Clamping Retracting Cutting and Dissecting Probing and DilatingTintin TagupaNo ratings yet
- Pulp Testing: A Literature Review: Tahreem Fathima, Anjaneyulu, D. EzhilarasanDocument20 pagesPulp Testing: A Literature Review: Tahreem Fathima, Anjaneyulu, D. EzhilarasanGabriela SolanoNo ratings yet
- YIJOM Molar 36 PDFDocument5 pagesYIJOM Molar 36 PDFCatalin GeorgeNo ratings yet
- Case PresentationDocument5 pagesCase Presentationapi-613926684No ratings yet
- Znbjma1977@codental - Uobaghdad.edu - Iq: Ministry of Health Training Dentist 1 Ministry of Health Gradated Dentist 2Document28 pagesZnbjma1977@codental - Uobaghdad.edu - Iq: Ministry of Health Training Dentist 1 Ministry of Health Gradated Dentist 2maryam.saadNo ratings yet
- Dental Hygiene EssayDocument13 pagesDental Hygiene Essayapi-3173047210% (1)
- The Significance of Anatomic Landmarks in Complete Denture ServiceDocument4 pagesThe Significance of Anatomic Landmarks in Complete Denture ServiceJoshua ValdezNo ratings yet
- Department of Orthodontic Abstracts and ReviewsDocument8 pagesDepartment of Orthodontic Abstracts and ReviewsNguyễn QuỳnhNo ratings yet
- Adhesion To Enamel of Teeth Affected by Molar Incisor Hypomineralization: Literature ReviewDocument7 pagesAdhesion To Enamel of Teeth Affected by Molar Incisor Hypomineralization: Literature ReviewanonimoNo ratings yet
- Seminar On: Chronic PeriodontitisDocument48 pagesSeminar On: Chronic PeriodontitisTuan Nguyen100% (1)
- Lec. OneDocument6 pagesLec. OneHaider F YehyaNo ratings yet
- Clin Adv Periodontics - 2023 - Mallappa - Novel Biomaterial Advanced Platelet Rich Fibrin Plus Block For Multiple GingivalDocument7 pagesClin Adv Periodontics - 2023 - Mallappa - Novel Biomaterial Advanced Platelet Rich Fibrin Plus Block For Multiple GingivalNikit DixitNo ratings yet
- Terminology For Implant Prostheses PDFDocument5 pagesTerminology For Implant Prostheses PDFHugoMoralesTecnicoDentalNo ratings yet
- Paper 2Document6 pagesPaper 2runit nangaliaNo ratings yet
- Article 1496471672Document6 pagesArticle 1496471672Irene KeniaNo ratings yet
- Dental IndexDocument19 pagesDental IndexAli HaDi MohamedNo ratings yet
- Use of Anatomic Post and Core For Reconstructing An Endodontically Treated Tooth: A Case ReportDocument6 pagesUse of Anatomic Post and Core For Reconstructing An Endodontically Treated Tooth: A Case ReportsolangeNo ratings yet
- Orban Chapter 1Document2 pagesOrban Chapter 1Shreya VyasNo ratings yet
- Plant A Better Tomorrow: by Maricon EstrelladoDocument10 pagesPlant A Better Tomorrow: by Maricon EstrelladoCARLOS, Ryan CholoNo ratings yet
- Brochure Veraviewepocs 3D R100 2019 ENDocument16 pagesBrochure Veraviewepocs 3D R100 2019 ENJosé Daniel Campos MéndezNo ratings yet
- Dentist Hong Kong Jain SmithDocument31 pagesDentist Hong Kong Jain SmithcheriesandeepNo ratings yet
- Class I Amalgam Restorations: Operative Dentistry Dent 335 Mohammad Atieh, BDS, MSDocument40 pagesClass I Amalgam Restorations: Operative Dentistry Dent 335 Mohammad Atieh, BDS, MSMahdy AlShammariNo ratings yet
- Questionnaire I. ProfileDocument2 pagesQuestionnaire I. ProfileAnnaNo ratings yet
- Toothpaste Industry in IndiaDocument30 pagesToothpaste Industry in IndiaNaureen ShabnamNo ratings yet
- Clinical Case Presentation Oct 26 AbhishekDocument26 pagesClinical Case Presentation Oct 26 AbhishekDr. Nachammai NagarajanNo ratings yet
- Fabrication of Adams Clasp: Dr. Ramy IshaqDocument48 pagesFabrication of Adams Clasp: Dr. Ramy IshaqhabeebNo ratings yet
- Sahrmann 2010Document12 pagesSahrmann 2010Dragos CiongaruNo ratings yet
- (1-4-20) 2013 - Clinical Recommedation Regarding Use of Cone Beam Computed Tomography in Orthodontics. Position Statement by The American Academi of Oral and Maxillofacial RadiologyDocument20 pages(1-4-20) 2013 - Clinical Recommedation Regarding Use of Cone Beam Computed Tomography in Orthodontics. Position Statement by The American Academi of Oral and Maxillofacial RadiologyBinta Bhirawa AnoragaNo ratings yet
- The Apert and Crouzon Syndromes: General and Dental Aspects and Management in Orthodontics and Dentofacial Orthopaedics: A Review ArticleDocument10 pagesThe Apert and Crouzon Syndromes: General and Dental Aspects and Management in Orthodontics and Dentofacial Orthopaedics: A Review ArticleOral DentNo ratings yet