
Therapy Space Proposal
Therapy Space Proposal
You might also like
- Effect of Elements On SteelDocument18 pagesEffect of Elements On SteelMohamed Ahmed MaherNo ratings yet
- 10 AGRI CROP Tle10 Afa Agricropprod q2 Mod2 Cleaninguponcompletionofcroppingwork v3 (44 Pages)Document44 pages10 AGRI CROP Tle10 Afa Agricropprod q2 Mod2 Cleaninguponcompletionofcroppingwork v3 (44 Pages)Rye San100% (2)
- Health Insurance Notes: Done By: Mohamed Arash (2020)Document18 pagesHealth Insurance Notes: Done By: Mohamed Arash (2020)Jag ProductionsNo ratings yet
- (1970) Differential Binding of Alkylaing Fluorochrome in Human ChromosomesDocument5 pages(1970) Differential Binding of Alkylaing Fluorochrome in Human Chromosomesmaulia praditaNo ratings yet
- FOSTERING DIGNITY AND RESPECT IN CARE NewDocument5 pagesFOSTERING DIGNITY AND RESPECT IN CARE NewSidra Waqar Khan100% (2)
- Attending BehaviourDocument4 pagesAttending BehaviourkanshaNo ratings yet
- Communication Skills: Dr. Hisham S. Abou-AudaDocument17 pagesCommunication Skills: Dr. Hisham S. Abou-Audadccompressor50% (2)
- Drinking Milk Products in Vietnam - Analysis: Country Report - Aug 2019Document3 pagesDrinking Milk Products in Vietnam - Analysis: Country Report - Aug 2019Tiger HồNo ratings yet
- Therapeutic CommunicationDocument82 pagesTherapeutic CommunicationYvette Vallejo100% (2)
- Study Guide Psych Nursing 4Document14 pagesStudy Guide Psych Nursing 4christine mercadoNo ratings yet
- CamileDocument42 pagesCamilebabypauNo ratings yet
- A Good and Effective Communication Is Essential For A NurseDocument5 pagesA Good and Effective Communication Is Essential For A NurseFaisalNo ratings yet
- Communication in MedicineDocument41 pagesCommunication in MedicineIvan OnggoNo ratings yet
- Interpersonal Communication Skills Research PaperDocument7 pagesInterpersonal Communication Skills Research PaperaflbrfeijNo ratings yet
- Essay - Therapeutic CommunicationDocument5 pagesEssay - Therapeutic CommunicationTimoci NavacokowaleNo ratings yet
- Chapter 4. 101. Week 7Document8 pagesChapter 4. 101. Week 7RAGOS Jeffrey Miguel P.No ratings yet
- Communication Skills For Health Care WorkersDocument25 pagesCommunication Skills For Health Care WorkersnketjimotswalediNo ratings yet
- Nurse - Client RelationshipDocument88 pagesNurse - Client RelationshipShara SampangNo ratings yet
- Factors Influencing The Communication ProcessDocument2 pagesFactors Influencing The Communication ProcessDilruba Umi67% (3)
- Persuasive Communication in NursingDocument4 pagesPersuasive Communication in NursingNicole Audrey JoaquinNo ratings yet
- 1 PBDocument17 pages1 PBsaul-miranda-ramosNo ratings yet
- Communication and Culture: The Basic ConceptsDocument12 pagesCommunication and Culture: The Basic ConceptsWidyawati SalsabilaNo ratings yet
- Concept and Theory Communication and Therapeutic CommunicationDocument22 pagesConcept and Theory Communication and Therapeutic CommunicationDzi Putri CiemNo ratings yet
- Nursing and Midwifery Training CollegeDocument3 pagesNursing and Midwifery Training CollegeCirilo JuniorNo ratings yet
- Communication NEWDocument16 pagesCommunication NEWNawaloka NTSNo ratings yet
- Skill Lab Komunikasi Interpersonal Blok 1Document16 pagesSkill Lab Komunikasi Interpersonal Blok 1Elsafani FaddiasyaNo ratings yet
- Key Skills in CounsellingDocument11 pagesKey Skills in CounsellingJohn Jj LawlessNo ratings yet
- Nama: 1. Intan Sari (59) 2. Evina Dian Rahmawati 60) Tingkat: 2BDocument23 pagesNama: 1. Intan Sari (59) 2. Evina Dian Rahmawati 60) Tingkat: 2BEvina DianNo ratings yet
- Kelompok 8, 3a-1Document21 pagesKelompok 8, 3a-1Tyania MaharaniNo ratings yet
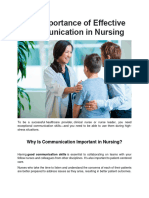
- The Importance of Effective Communication in NursinDocument7 pagesThe Importance of Effective Communication in NursinCARLA ROCIO ORTEGA RIVERANo ratings yet
- Advanced Communications Final Paper 3Document14 pagesAdvanced Communications Final Paper 3api-316574434No ratings yet
- Therapeutic Communication-1Document24 pagesTherapeutic Communication-1Chelsa Yuliana putriNo ratings yet
- Mutual Help Meeting Website DownloadDocument5 pagesMutual Help Meeting Website DownloadmeillisaNo ratings yet
- Skillful Communication AND COORDINATION SCRIPTDocument12 pagesSkillful Communication AND COORDINATION SCRIPTDanna Faye EcaruanNo ratings yet
- FOSTERING DIGNITY AND RESPECT IN CARE NewDocument5 pagesFOSTERING DIGNITY AND RESPECT IN CARE NewSidra Waqar KhanNo ratings yet
- Working With Mandated Substance Abusers - Language of SolutionsDocument33 pagesWorking With Mandated Substance Abusers - Language of SolutionsbmckNo ratings yet
- Unit 10 CommunicationDocument3 pagesUnit 10 CommunicationlauraNo ratings yet
- Interviewing SkillsDocument6 pagesInterviewing SkillsEchoNo ratings yet
- Describing The Purposes of CommunicationDocument4 pagesDescribing The Purposes of CommunicationFRANCINE JULIA DAUGNo ratings yet
- Effective Communication: Urwa Naseer Clinical Psychologist Sughra Shafi Medical Complex NarowalDocument29 pagesEffective Communication: Urwa Naseer Clinical Psychologist Sughra Shafi Medical Complex NarowalSamia AsgharNo ratings yet
- Therapeutic Relationship and CommunicationDocument12 pagesTherapeutic Relationship and CommunicationLAGRANA, MA. ANGELICA A.No ratings yet
- CounsellingDocument12 pagesCounsellingbanerjeerhiNo ratings yet
- Therapeutic Communication: Emilio Aguinaldo CollegeDocument13 pagesTherapeutic Communication: Emilio Aguinaldo CollegeJor GarciaNo ratings yet
- Miller 5 StagiiDocument40 pagesMiller 5 Stagiivera veronicaNo ratings yet
- The Interview (Clinical Psych)Document6 pagesThe Interview (Clinical Psych)Elijah DiazNo ratings yet
- Critical Inquiry EssayDocument6 pagesCritical Inquiry EssayDaniel PrattNo ratings yet
- RRLDocument5 pagesRRLRhoxie RoxasNo ratings yet
- Chapter 2 Review of Related LiteratureDocument10 pagesChapter 2 Review of Related Literaturenin0ybaltazar09No ratings yet
- Communication Skills in Family MedicineDocument24 pagesCommunication Skills in Family MedicineTheop AyodeleNo ratings yet
- Communication ProcessDocument4 pagesCommunication Processdebora saroinsongNo ratings yet
- Communication For PHLEBOTOMISTSDocument8 pagesCommunication For PHLEBOTOMISTSlisalov0% (1)
- Interaction Nursing Staff PDFDocument12 pagesInteraction Nursing Staff PDFLina SafitriNo ratings yet
- NUR HOSSEN (UZZAL) Stamford University BangladeshDocument7 pagesNUR HOSSEN (UZZAL) Stamford University Bangladeshuzzal ahmed100% (1)
- Ask & Tell ModelDocument4 pagesAsk & Tell ModelForam ShahNo ratings yet
- Connecting in The Acute SettingDocument3 pagesConnecting in The Acute SettingSpeech & Language Therapy in PracticeNo ratings yet
- Danilo Reflective AccountDocument3 pagesDanilo Reflective AccountGracie S. VergaraNo ratings yet
- Therapist Perspectives On Using Silence in Therapy: A Qualitative StudyDocument36 pagesTherapist Perspectives On Using Silence in Therapy: A Qualitative StudyÖzge YükselNo ratings yet
- CounsellingDocument55 pagesCounsellinghasna.psyyNo ratings yet
- 315 Cultural Safety Assignment 2023Document21 pages315 Cultural Safety Assignment 2023api-651972035No ratings yet
- 2.interpersonal CommDocument6 pages2.interpersonal CommJulius Kent QuilapioNo ratings yet
- Process RecordingDocument7 pagesProcess RecordingKim ApuradoNo ratings yet
- Week 1 DQDocument3 pagesWeek 1 DQapi-461854481No ratings yet
- Therapeutic Communication AND Nurse - Patient RelationshipDocument12 pagesTherapeutic Communication AND Nurse - Patient Relationshipdhiya sNo ratings yet
- Year 9 Biology InvestigationDocument2 pagesYear 9 Biology Investigationapi-222503660No ratings yet
- Murder MemoDocument3 pagesMurder MemoRishika AgarwalNo ratings yet
- Microcontroller Based Heart Rate Monitor: Sharanabasappa Sali, Pooja Durge, Monika Pokar, Namrata KasgeDocument4 pagesMicrocontroller Based Heart Rate Monitor: Sharanabasappa Sali, Pooja Durge, Monika Pokar, Namrata Kasgemahavarun3096No ratings yet
- About PolyethyleneDocument4 pagesAbout PolyethyleneMifzal IzzaniNo ratings yet
- Broken BeautyDocument143 pagesBroken BeautyAngelica MakAngelNo ratings yet
- Mindmap For Hands Held HighDocument1 pageMindmap For Hands Held Highapi-523333030No ratings yet
- SPE-177272-MS Replacement of ESP With Long Stroke Pumping Units in Heavy and High Viscous Oil in Maranta Block WellsDocument16 pagesSPE-177272-MS Replacement of ESP With Long Stroke Pumping Units in Heavy and High Viscous Oil in Maranta Block WellsFajar Putra NugrahaNo ratings yet
- Supply Chain Risk Management Script - EditedDocument2 pagesSupply Chain Risk Management Script - EditedshahzaibNo ratings yet
- Dui PDFDocument2 pagesDui PDFbearj7637No ratings yet
- Chapter 10tifDocument41 pagesChapter 10tifManP130% (1)
- It's Cool Supplies Purchases JournalDocument11 pagesIt's Cool Supplies Purchases JournalCharina Jane PascualNo ratings yet
- HHS Public Access: Sodium-Glucose CotransportDocument12 pagesHHS Public Access: Sodium-Glucose CotransportAlexandra VásquezNo ratings yet
- Klarer Alexandra Resume 2020Document4 pagesKlarer Alexandra Resume 2020api-372551104No ratings yet
- Dental Changes in Humans With Untreated Normal Occlusion Throughout Lifetime A Systematic Scoping ReviewDocument26 pagesDental Changes in Humans With Untreated Normal Occlusion Throughout Lifetime A Systematic Scoping ReviewNatasha NascimentoNo ratings yet
- Approach To Coagulation DisordersDocument20 pagesApproach To Coagulation DisordersTri P BukerNo ratings yet
- High Yield Full Test 13 Aug NEETPrepDocument24 pagesHigh Yield Full Test 13 Aug NEETPrepchichaNo ratings yet
- Dispelling Myths Surrounding ISO Final HenryDocument25 pagesDispelling Myths Surrounding ISO Final HenrySankaranarayananNo ratings yet
- SYNCHRONIZE 1 Resources U5Document13 pagesSYNCHRONIZE 1 Resources U5Sabah Samadi El HassouniNo ratings yet
- CBSE Class 11 English Core Sample Paper 05 (2019-20) : Material Downloaded From - 1 / 19Document19 pagesCBSE Class 11 English Core Sample Paper 05 (2019-20) : Material Downloaded From - 1 / 19Samridh GuptaNo ratings yet
- UT NotesDocument8 pagesUT NotesAbhijith ChandranNo ratings yet
- Parental Satisfaction (Parents of Children 0-17, Elementary-High School) - 0Document4 pagesParental Satisfaction (Parents of Children 0-17, Elementary-High School) - 0Sergio Alejandro Blanes CàceresNo ratings yet
- Faradic Type CurrentDocument26 pagesFaradic Type CurrentzainabnoorNo ratings yet
- How To Love Your Parents PoemDocument2 pagesHow To Love Your Parents Poemwenna janeNo ratings yet
- How Rfid Technology Boosts Walmart S Sup PDFDocument10 pagesHow Rfid Technology Boosts Walmart S Sup PDFKshitij ShuklaNo ratings yet
- Rod Bending - Eastwood - 21320Q - InstDocument8 pagesRod Bending - Eastwood - 21320Q - InstsimplyrajuNo ratings yet
























































































Download as docx, pdf, or txt
You might also like
- Effect of Elements On SteelDocument18 pagesEffect of Elements On SteelMohamed Ahmed MaherNo ratings yet
- 10 AGRI CROP Tle10 Afa Agricropprod q2 Mod2 Cleaninguponcompletionofcroppingwork v3 (44 Pages)Document44 pages10 AGRI CROP Tle10 Afa Agricropprod q2 Mod2 Cleaninguponcompletionofcroppingwork v3 (44 Pages)Rye San100% (2)
- Health Insurance Notes: Done By: Mohamed Arash (2020)Document18 pagesHealth Insurance Notes: Done By: Mohamed Arash (2020)Jag ProductionsNo ratings yet
- (1970) Differential Binding of Alkylaing Fluorochrome in Human ChromosomesDocument5 pages(1970) Differential Binding of Alkylaing Fluorochrome in Human Chromosomesmaulia praditaNo ratings yet
- FOSTERING DIGNITY AND RESPECT IN CARE NewDocument5 pagesFOSTERING DIGNITY AND RESPECT IN CARE NewSidra Waqar Khan100% (2)
- Attending BehaviourDocument4 pagesAttending BehaviourkanshaNo ratings yet
- Communication Skills: Dr. Hisham S. Abou-AudaDocument17 pagesCommunication Skills: Dr. Hisham S. Abou-Audadccompressor50% (2)
- Drinking Milk Products in Vietnam - Analysis: Country Report - Aug 2019Document3 pagesDrinking Milk Products in Vietnam - Analysis: Country Report - Aug 2019Tiger HồNo ratings yet
- Therapeutic CommunicationDocument82 pagesTherapeutic CommunicationYvette Vallejo100% (2)
- Study Guide Psych Nursing 4Document14 pagesStudy Guide Psych Nursing 4christine mercadoNo ratings yet
- CamileDocument42 pagesCamilebabypauNo ratings yet
- A Good and Effective Communication Is Essential For A NurseDocument5 pagesA Good and Effective Communication Is Essential For A NurseFaisalNo ratings yet
- Communication in MedicineDocument41 pagesCommunication in MedicineIvan OnggoNo ratings yet
- Interpersonal Communication Skills Research PaperDocument7 pagesInterpersonal Communication Skills Research PaperaflbrfeijNo ratings yet
- Essay - Therapeutic CommunicationDocument5 pagesEssay - Therapeutic CommunicationTimoci NavacokowaleNo ratings yet
- Chapter 4. 101. Week 7Document8 pagesChapter 4. 101. Week 7RAGOS Jeffrey Miguel P.No ratings yet
- Communication Skills For Health Care WorkersDocument25 pagesCommunication Skills For Health Care WorkersnketjimotswalediNo ratings yet
- Nurse - Client RelationshipDocument88 pagesNurse - Client RelationshipShara SampangNo ratings yet
- Factors Influencing The Communication ProcessDocument2 pagesFactors Influencing The Communication ProcessDilruba Umi67% (3)
- Persuasive Communication in NursingDocument4 pagesPersuasive Communication in NursingNicole Audrey JoaquinNo ratings yet
- 1 PBDocument17 pages1 PBsaul-miranda-ramosNo ratings yet
- Communication and Culture: The Basic ConceptsDocument12 pagesCommunication and Culture: The Basic ConceptsWidyawati SalsabilaNo ratings yet
- Concept and Theory Communication and Therapeutic CommunicationDocument22 pagesConcept and Theory Communication and Therapeutic CommunicationDzi Putri CiemNo ratings yet
- Nursing and Midwifery Training CollegeDocument3 pagesNursing and Midwifery Training CollegeCirilo JuniorNo ratings yet
- Communication NEWDocument16 pagesCommunication NEWNawaloka NTSNo ratings yet
- Skill Lab Komunikasi Interpersonal Blok 1Document16 pagesSkill Lab Komunikasi Interpersonal Blok 1Elsafani FaddiasyaNo ratings yet
- Key Skills in CounsellingDocument11 pagesKey Skills in CounsellingJohn Jj LawlessNo ratings yet
- Nama: 1. Intan Sari (59) 2. Evina Dian Rahmawati 60) Tingkat: 2BDocument23 pagesNama: 1. Intan Sari (59) 2. Evina Dian Rahmawati 60) Tingkat: 2BEvina DianNo ratings yet
- Kelompok 8, 3a-1Document21 pagesKelompok 8, 3a-1Tyania MaharaniNo ratings yet
- The Importance of Effective Communication in NursinDocument7 pagesThe Importance of Effective Communication in NursinCARLA ROCIO ORTEGA RIVERANo ratings yet
- Advanced Communications Final Paper 3Document14 pagesAdvanced Communications Final Paper 3api-316574434No ratings yet
- Therapeutic Communication-1Document24 pagesTherapeutic Communication-1Chelsa Yuliana putriNo ratings yet
- Mutual Help Meeting Website DownloadDocument5 pagesMutual Help Meeting Website DownloadmeillisaNo ratings yet
- Skillful Communication AND COORDINATION SCRIPTDocument12 pagesSkillful Communication AND COORDINATION SCRIPTDanna Faye EcaruanNo ratings yet
- FOSTERING DIGNITY AND RESPECT IN CARE NewDocument5 pagesFOSTERING DIGNITY AND RESPECT IN CARE NewSidra Waqar KhanNo ratings yet
- Working With Mandated Substance Abusers - Language of SolutionsDocument33 pagesWorking With Mandated Substance Abusers - Language of SolutionsbmckNo ratings yet
- Unit 10 CommunicationDocument3 pagesUnit 10 CommunicationlauraNo ratings yet
- Interviewing SkillsDocument6 pagesInterviewing SkillsEchoNo ratings yet
- Describing The Purposes of CommunicationDocument4 pagesDescribing The Purposes of CommunicationFRANCINE JULIA DAUGNo ratings yet
- Effective Communication: Urwa Naseer Clinical Psychologist Sughra Shafi Medical Complex NarowalDocument29 pagesEffective Communication: Urwa Naseer Clinical Psychologist Sughra Shafi Medical Complex NarowalSamia AsgharNo ratings yet
- Therapeutic Relationship and CommunicationDocument12 pagesTherapeutic Relationship and CommunicationLAGRANA, MA. ANGELICA A.No ratings yet
- CounsellingDocument12 pagesCounsellingbanerjeerhiNo ratings yet
- Therapeutic Communication: Emilio Aguinaldo CollegeDocument13 pagesTherapeutic Communication: Emilio Aguinaldo CollegeJor GarciaNo ratings yet
- Miller 5 StagiiDocument40 pagesMiller 5 Stagiivera veronicaNo ratings yet
- The Interview (Clinical Psych)Document6 pagesThe Interview (Clinical Psych)Elijah DiazNo ratings yet
- Critical Inquiry EssayDocument6 pagesCritical Inquiry EssayDaniel PrattNo ratings yet
- RRLDocument5 pagesRRLRhoxie RoxasNo ratings yet
- Chapter 2 Review of Related LiteratureDocument10 pagesChapter 2 Review of Related Literaturenin0ybaltazar09No ratings yet
- Communication Skills in Family MedicineDocument24 pagesCommunication Skills in Family MedicineTheop AyodeleNo ratings yet
- Communication ProcessDocument4 pagesCommunication Processdebora saroinsongNo ratings yet
- Communication For PHLEBOTOMISTSDocument8 pagesCommunication For PHLEBOTOMISTSlisalov0% (1)
- Interaction Nursing Staff PDFDocument12 pagesInteraction Nursing Staff PDFLina SafitriNo ratings yet
- NUR HOSSEN (UZZAL) Stamford University BangladeshDocument7 pagesNUR HOSSEN (UZZAL) Stamford University Bangladeshuzzal ahmed100% (1)
- Ask & Tell ModelDocument4 pagesAsk & Tell ModelForam ShahNo ratings yet
- Connecting in The Acute SettingDocument3 pagesConnecting in The Acute SettingSpeech & Language Therapy in PracticeNo ratings yet
- Danilo Reflective AccountDocument3 pagesDanilo Reflective AccountGracie S. VergaraNo ratings yet
- Therapist Perspectives On Using Silence in Therapy: A Qualitative StudyDocument36 pagesTherapist Perspectives On Using Silence in Therapy: A Qualitative StudyÖzge YükselNo ratings yet
- CounsellingDocument55 pagesCounsellinghasna.psyyNo ratings yet
- 315 Cultural Safety Assignment 2023Document21 pages315 Cultural Safety Assignment 2023api-651972035No ratings yet
- 2.interpersonal CommDocument6 pages2.interpersonal CommJulius Kent QuilapioNo ratings yet
- Process RecordingDocument7 pagesProcess RecordingKim ApuradoNo ratings yet
- Week 1 DQDocument3 pagesWeek 1 DQapi-461854481No ratings yet
- Therapeutic Communication AND Nurse - Patient RelationshipDocument12 pagesTherapeutic Communication AND Nurse - Patient Relationshipdhiya sNo ratings yet
- Year 9 Biology InvestigationDocument2 pagesYear 9 Biology Investigationapi-222503660No ratings yet
- Murder MemoDocument3 pagesMurder MemoRishika AgarwalNo ratings yet
- Microcontroller Based Heart Rate Monitor: Sharanabasappa Sali, Pooja Durge, Monika Pokar, Namrata KasgeDocument4 pagesMicrocontroller Based Heart Rate Monitor: Sharanabasappa Sali, Pooja Durge, Monika Pokar, Namrata Kasgemahavarun3096No ratings yet
- About PolyethyleneDocument4 pagesAbout PolyethyleneMifzal IzzaniNo ratings yet
- Broken BeautyDocument143 pagesBroken BeautyAngelica MakAngelNo ratings yet
- Mindmap For Hands Held HighDocument1 pageMindmap For Hands Held Highapi-523333030No ratings yet
- SPE-177272-MS Replacement of ESP With Long Stroke Pumping Units in Heavy and High Viscous Oil in Maranta Block WellsDocument16 pagesSPE-177272-MS Replacement of ESP With Long Stroke Pumping Units in Heavy and High Viscous Oil in Maranta Block WellsFajar Putra NugrahaNo ratings yet
- Supply Chain Risk Management Script - EditedDocument2 pagesSupply Chain Risk Management Script - EditedshahzaibNo ratings yet
- Dui PDFDocument2 pagesDui PDFbearj7637No ratings yet
- Chapter 10tifDocument41 pagesChapter 10tifManP130% (1)
- It's Cool Supplies Purchases JournalDocument11 pagesIt's Cool Supplies Purchases JournalCharina Jane PascualNo ratings yet
- HHS Public Access: Sodium-Glucose CotransportDocument12 pagesHHS Public Access: Sodium-Glucose CotransportAlexandra VásquezNo ratings yet
- Klarer Alexandra Resume 2020Document4 pagesKlarer Alexandra Resume 2020api-372551104No ratings yet
- Dental Changes in Humans With Untreated Normal Occlusion Throughout Lifetime A Systematic Scoping ReviewDocument26 pagesDental Changes in Humans With Untreated Normal Occlusion Throughout Lifetime A Systematic Scoping ReviewNatasha NascimentoNo ratings yet
- Approach To Coagulation DisordersDocument20 pagesApproach To Coagulation DisordersTri P BukerNo ratings yet
- High Yield Full Test 13 Aug NEETPrepDocument24 pagesHigh Yield Full Test 13 Aug NEETPrepchichaNo ratings yet
- Dispelling Myths Surrounding ISO Final HenryDocument25 pagesDispelling Myths Surrounding ISO Final HenrySankaranarayananNo ratings yet
- SYNCHRONIZE 1 Resources U5Document13 pagesSYNCHRONIZE 1 Resources U5Sabah Samadi El HassouniNo ratings yet
- CBSE Class 11 English Core Sample Paper 05 (2019-20) : Material Downloaded From - 1 / 19Document19 pagesCBSE Class 11 English Core Sample Paper 05 (2019-20) : Material Downloaded From - 1 / 19Samridh GuptaNo ratings yet
- UT NotesDocument8 pagesUT NotesAbhijith ChandranNo ratings yet
- Parental Satisfaction (Parents of Children 0-17, Elementary-High School) - 0Document4 pagesParental Satisfaction (Parents of Children 0-17, Elementary-High School) - 0Sergio Alejandro Blanes CàceresNo ratings yet
- Faradic Type CurrentDocument26 pagesFaradic Type CurrentzainabnoorNo ratings yet
- How To Love Your Parents PoemDocument2 pagesHow To Love Your Parents Poemwenna janeNo ratings yet
- How Rfid Technology Boosts Walmart S Sup PDFDocument10 pagesHow Rfid Technology Boosts Walmart S Sup PDFKshitij ShuklaNo ratings yet
- Rod Bending - Eastwood - 21320Q - InstDocument8 pagesRod Bending - Eastwood - 21320Q - InstsimplyrajuNo ratings yet