Download as pdf or txt
You might also like
- Sweet Poison - David Gillespie PDFDocument214 pagesSweet Poison - David Gillespie PDFvalterbrigo100% (10)
- Test Method For Water Resistance: Impact Penetration: AATCC TM42-2017eDocument2 pagesTest Method For Water Resistance: Impact Penetration: AATCC TM42-2017eAbraham ToxtleNo ratings yet
- Ketogenic Diet - PresentationDocument14 pagesKetogenic Diet - PresentationMaya Ballout100% (2)
- Anesthesiology Resident Manual of Procedures: A Step-by-Step GuideFrom EverandAnesthesiology Resident Manual of Procedures: A Step-by-Step GuideNo ratings yet
- Basic Thompson Info and HistoryDocument8 pagesBasic Thompson Info and HistoryClara PIMENTELNo ratings yet
- Total Chloride in Alumina Supported Catalysts by Wavelength Dispersive X-Ray FluorescenceDocument5 pagesTotal Chloride in Alumina Supported Catalysts by Wavelength Dispersive X-Ray FluorescenceJesus Gonzalez GracidaNo ratings yet
- NLN Pharmacology Study Guide Final 6-3-2013Document65 pagesNLN Pharmacology Study Guide Final 6-3-2013الأغا محمد زكارنة100% (2)
- Are Daily Anesthesia Machine Checks Needed - Courtemanche & AssociatesDocument3 pagesAre Daily Anesthesia Machine Checks Needed - Courtemanche & Associates建榮廖No ratings yet
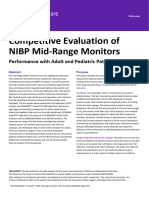
- 14 Evaluation of NIBP Continuous MonitoringPerformance With Adult, Ped Patients White PaperDocument5 pages14 Evaluation of NIBP Continuous MonitoringPerformance With Adult, Ped Patients White PaperxiaoxcorazonNo ratings yet
- CM Vaporiser PPDocument15 pagesCM Vaporiser PPAlaa Ibrahem AhmedNo ratings yet
- Calificacion de Sistema HVAC 5Document11 pagesCalificacion de Sistema HVAC 5Christian QuirozNo ratings yet
- 2710 Tests On Sludges : 1. General DiscussionDocument8 pages2710 Tests On Sludges : 1. General Discussionpollux23No ratings yet
- Me Lab1 Group3Document20 pagesMe Lab1 Group3DECIPOLO, KENNETH JOHN E.No ratings yet
- Sys Master - Pdfs - h47 - h97 - 10137304694814 - COA - RTC PHR 1003 - ST WB CERT 2140232 1 1 1Document7 pagesSys Master - Pdfs - h47 - h97 - 10137304694814 - COA - RTC PHR 1003 - ST WB CERT 2140232 1 1 1Rayan Ayyesha AuliaNo ratings yet
- Instructions For Nitrogen Oxides Detector TubeDocument1 pageInstructions For Nitrogen Oxides Detector TubeJohn Anthony DanaNo ratings yet
- Feasibility of Applying Manual Microplate Elisas To General Purpose Automated InstrumentsDocument4 pagesFeasibility of Applying Manual Microplate Elisas To General Purpose Automated InstrumentsbaileybancroftNo ratings yet
- Uji Potensi Antibiotik Turbidimetri USP 41Document8 pagesUji Potensi Antibiotik Turbidimetri USP 41nicholasNo ratings yet
- 5200 Oxygen USPDocument33 pages5200 Oxygen USPJennie CardozoNo ratings yet
- Accuracy and Precision of Desktop Spirometers in General PracticesDocument9 pagesAccuracy and Precision of Desktop Spirometers in General PracticesMihai PetrescuNo ratings yet
- Analytical Errors & Validation of Analytical ProceduresDocument61 pagesAnalytical Errors & Validation of Analytical ProceduresMtw WondNo ratings yet
- IndikopublicationDocument8 pagesIndikopublicationKalai SelvanNo ratings yet
- Catalase Lab TemplateDocument4 pagesCatalase Lab TemplateMaria SvetlovaNo ratings yet
- Dade Ci-Trol Coagulation Control Level 1 - Rev 04 DXDCM 09017fe9804eb34d-1605649191863Document3 pagesDade Ci-Trol Coagulation Control Level 1 - Rev 04 DXDCM 09017fe9804eb34d-1605649191863xuanhungyteNo ratings yet
- EPA Method 21-DETERMINATION OF VOLATILE ORGANIC COMPOUND LEAKSDocument17 pagesEPA Method 21-DETERMINATION OF VOLATILE ORGANIC COMPOUND LEAKSwholenumberNo ratings yet
- Endotoxin Test Protocol PTSDocument5 pagesEndotoxin Test Protocol PTSSebastián SalazarNo ratings yet
- PreciControl Everolimus - Ms - 07294131190.v1.en PDFDocument2 pagesPreciControl Everolimus - Ms - 07294131190.v1.en PDFARIF AHAMMED PNo ratings yet
- Pricing Analysis of Two ProductsDocument8 pagesPricing Analysis of Two ProductsVJ Reddy RNo ratings yet
- E OVO Lassification Equest For Urve Ositive Irway Ressure YstemDocument12 pagesE OVO Lassification Equest For Urve Ositive Irway Ressure YstemPeyman BakhshandeNo ratings yet
- Transferrin MDDocument1 pageTransferrin MDPhong Nguyễn WindyNo ratings yet
- HHS Public Access: A Test of Validity of A New Open-Circuit Indirect CalorimeterDocument11 pagesHHS Public Access: A Test of Validity of A New Open-Circuit Indirect CalorimeterNyimas HoirunisaNo ratings yet
- A Survey On Long-Term Stability of Stock Standard Solutions in Pesticide Residue AnalysisDocument9 pagesA Survey On Long-Term Stability of Stock Standard Solutions in Pesticide Residue AnalysisVitor Lyrio do Valle Borges de SiqueiraNo ratings yet
- Wa0000.Document4 pagesWa0000.Jashandeep SinghNo ratings yet
- DT123 - 08 - 03 - 18 - L. Walker, 2010Document2 pagesDT123 - 08 - 03 - 18 - L. Walker, 2010Marina CiminoNo ratings yet
- An Evaluation of The Repeatability and Reproducibility of A Surface Test For The Activity of DisinfectantsDocument9 pagesAn Evaluation of The Repeatability and Reproducibility of A Surface Test For The Activity of DisinfectantsalejandraNo ratings yet
- 06 - Immunoturbidimetria e NefelometriaDocument13 pages06 - Immunoturbidimetria e NefelometriaDoris MedinaNo ratings yet
- Quality Assurance Guidelines For ESHO Protocols: TMRC Unit, London W12 UK. of GV Denmark. 9 1 190Document8 pagesQuality Assurance Guidelines For ESHO Protocols: TMRC Unit, London W12 UK. of GV Denmark. 9 1 190gaia34No ratings yet
- FinalprintedversionDocument9 pagesFinalprintedversionشادي العمرNo ratings yet
- Shelf Life Determination byDocument3 pagesShelf Life Determination byNur Asni NurNo ratings yet
- Lab Policies Free Thyroxine FT4 Cobas E601 Lab 4045Document4 pagesLab Policies Free Thyroxine FT4 Cobas E601 Lab 4045TohăneanR.RomeliaNo ratings yet
- Transferrin: OSR6152 4 X 7 ML R1 4 X 8 ML R2Document2 pagesTransferrin: OSR6152 4 X 7 ML R1 4 X 8 ML R2TanveerNo ratings yet
- Anaesthesia Machine Check - 2023Document31 pagesAnaesthesia Machine Check - 2023Melvin CyriacNo ratings yet
- Spirometry Performance and Interpretation For HCP 1615093153Document19 pagesSpirometry Performance and Interpretation For HCP 1615093153Ratih Nurdiany SumiratNo ratings yet
- ASTM D2163 GLP CromatografiaDocument5 pagesASTM D2163 GLP Cromatografiaalejandrogrande100% (1)
- Analytical Platforms and Immunoassay Interference: DR Les Perry Consultant Clinical Scientist Croydon University HospitalDocument27 pagesAnalytical Platforms and Immunoassay Interference: DR Les Perry Consultant Clinical Scientist Croydon University Hospitalmonday125No ratings yet
- Le Souef1Document5 pagesLe Souef1Tavo Aravena TorresNo ratings yet
- Water Resistance: Impact Penetration TestDocument2 pagesWater Resistance: Impact Penetration TestNguyễn Công ThoạiNo ratings yet
- Calibration-Of-Micropipettes ArtDocument8 pagesCalibration-Of-Micropipettes ArtRamNo ratings yet
- Validation of Dynamic Pass BoxDocument5 pagesValidation of Dynamic Pass BoxMichele Volpe100% (1)
- ASTM Chapter E2111Document9 pagesASTM Chapter E2111Chetalee Naik100% (1)
- Manual 0636 9835 6Document16 pagesManual 0636 9835 6izvytorresNo ratings yet
- Table 1Document4 pagesTable 1soemindkshNo ratings yet
- Online Data Supplement For:: 1. Extended Methods 1.1 Breath CollectionDocument8 pagesOnline Data Supplement For:: 1. Extended Methods 1.1 Breath CollectionSilvermist EiceliNo ratings yet
- UOP 555-10 Trace Impurities in Benzene by GCDocument11 pagesUOP 555-10 Trace Impurities in Benzene by GCMorteza SepehranNo ratings yet
- Method 21 - Determination of Volatile Organic Compound LeaksDocument7 pagesMethod 21 - Determination of Volatile Organic Compound LeaksCésar Oswaldo Aguilera Ojeda100% (1)
- Standard Test Method For Vapor Pressure of Liquefied Petroleum Gases (LPG) (Expansion Method)Document7 pagesStandard Test Method For Vapor Pressure of Liquefied Petroleum Gases (LPG) (Expansion Method)José Hernández VázquezNo ratings yet
- E 1135 - 97 RtexmzutotcDocument5 pagesE 1135 - 97 RtexmzutotccarlosNo ratings yet
- Drug Regulation & Regulatory Authorities: Experiment No.: DateDocument12 pagesDrug Regulation & Regulatory Authorities: Experiment No.: DateNeelam MalikNo ratings yet
- 〈151〉 Pyrogen TestDocument2 pages〈151〉 Pyrogen Testjafranco.tfsNo ratings yet
- Vital Widal IfuDocument2 pagesVital Widal IfuMuhammad Rizaldi RidwanNo ratings yet
- Astm D 4052 PDFDocument5 pagesAstm D 4052 PDFRamu NallathambiNo ratings yet
- 5991-1196en - Optimized Method Development of Large Volume Injection For Gc-Ms-Ms of Food PesticidesDocument16 pages5991-1196en - Optimized Method Development of Large Volume Injection For Gc-Ms-Ms of Food PesticidesDiego BermudezNo ratings yet
- HEPA Testing MethodsDocument5 pagesHEPA Testing MethodsLongKimNo ratings yet
- Monitoring Mechanical Ventilation Using Ventilator WaveformsFrom EverandMonitoring Mechanical Ventilation Using Ventilator WaveformsNo ratings yet
- Topic in Mental HealthDocument3 pagesTopic in Mental HealthSin ChiNo ratings yet
- Leader's Guide Summer Camp 2023Document132 pagesLeader's Guide Summer Camp 2023Jonathan ReevesNo ratings yet
- Starland International School Senior High School Department 1st Semester Prelim Exams S.Y. 2021-2022 Physical Education 11Document2 pagesStarland International School Senior High School Department 1st Semester Prelim Exams S.Y. 2021-2022 Physical Education 11Ken PaiiNo ratings yet
- PAYSLIp - Bella Revise May 16-30Document1 pagePAYSLIp - Bella Revise May 16-30bktsuna0201No ratings yet
- Government Response To The PandemicDocument2 pagesGovernment Response To The PandemicMikhail MontanoNo ratings yet
- Newsletter Specialist Welding InspectorDocument2 pagesNewsletter Specialist Welding InspectortraklexNo ratings yet
- NSTP Proposal Sex Education 1Document2 pagesNSTP Proposal Sex Education 1dianne.mae.b.sevillaNo ratings yet
- Parkinson's DiseaseDocument25 pagesParkinson's DiseaseArko duttaNo ratings yet
- LifeShare PPT PresentationDocument12 pagesLifeShare PPT PresentationEriccaNo ratings yet
- Prescription - Apollo 2471659105066202Document2 pagesPrescription - Apollo 2471659105066202JEENEET CHEMISTRYNo ratings yet
- COVID-19: Stigmatising The Unvaccinated Is Not JustifiedDocument1 pageCOVID-19: Stigmatising The Unvaccinated Is Not JustifiedVilag HelyzeteNo ratings yet
- Isolation & Lock Out - Tag Out (LOTO)Document24 pagesIsolation & Lock Out - Tag Out (LOTO)Becha MouradNo ratings yet
- Food Control: SciencedirectDocument5 pagesFood Control: SciencedirectNabbNab Febriani NabfebNo ratings yet
- Pe 12 Week 10Document3 pagesPe 12 Week 10eldrich balinbinNo ratings yet
- Personal Development: Mrs. Jeanny Lou T. BadayosDocument20 pagesPersonal Development: Mrs. Jeanny Lou T. BadayosAngel DelgadoNo ratings yet
- Lplpo Poskeskel 2021Document6 pagesLplpo Poskeskel 2021Michel Caesar Analta MichelNo ratings yet
- The Following Text Is For The Questions Number 1 - 8: Ujian Kenaikan KelasDocument4 pagesThe Following Text Is For The Questions Number 1 - 8: Ujian Kenaikan Kelashari hermawanNo ratings yet
- Matthew Hodson - Shamelessly HIV-positive - Vada MagazineDocument19 pagesMatthew Hodson - Shamelessly HIV-positive - Vada MagazineAdamBeyonceLoweNo ratings yet
- A Glimpse To A Human Person: Who Am I?: Front PageDocument17 pagesA Glimpse To A Human Person: Who Am I?: Front PageGabrielle May LacsamanaNo ratings yet
- Preventol InfoDocument2 pagesPreventol InfoInderpreetKaurMaanNo ratings yet
- Public Notice: (Khair-Un-Nisa) Controller Sindh Nurses Examination BoardDocument9 pagesPublic Notice: (Khair-Un-Nisa) Controller Sindh Nurses Examination BoardMr MWSKNo ratings yet
- Duvvury Et Al. 2013 Intimate Partner Violence. Economic Costs and ImplicatiDocument97 pagesDuvvury Et Al. 2013 Intimate Partner Violence. Economic Costs and Implicatisamson jinaduNo ratings yet
- Advent of Calathea Plants and Its Taxonomy Amidst Covid19Document3 pagesAdvent of Calathea Plants and Its Taxonomy Amidst Covid19International Journal of Innovative Science and Research TechnologyNo ratings yet
- Pandemic ExpressDocument3 pagesPandemic ExpressGabriel KawaiNo ratings yet
- 2020 Can Pelvic Floor Muscle TrainingDocument2 pages2020 Can Pelvic Floor Muscle Trainingjuan pabloNo ratings yet
- Assessments CourseworkDocument1 pageAssessments Courseworkapi-392744023No ratings yet