Download as pdf or txt
You might also like
- Peri cesárea - bupi x ropiDocument12 pagesPeri cesárea - bupi x ropiarissoneuclidesNo ratings yet
- Amniotomy For Shortening Spontaneous Labour: Cochrane UpdateDocument2 pagesAmniotomy For Shortening Spontaneous Labour: Cochrane UpdatesuderiNo ratings yet
- Acupuncture and Acupressure in LaborDocument5 pagesAcupuncture and Acupressure in LaborAstri YuliandiniNo ratings yet
- Uog 20140Document11 pagesUog 20140vincentharlling90No ratings yet
- FertilSciRes5248-8504745 233727Document7 pagesFertilSciRes5248-8504745 233727JouleAlSBNo ratings yet
- Thesis PaperDocument5 pagesThesis PaperbhalNo ratings yet
- 2 Kata Pengantar HiDocument5 pages2 Kata Pengantar Hiaryo aryoNo ratings yet
- Methods To Induce Labour: A Systematic Review, Network Meta-Analysis and Cost-Effectiveness AnalysisDocument9 pagesMethods To Induce Labour: A Systematic Review, Network Meta-Analysis and Cost-Effectiveness AnalysisNinanu Nida-nnNo ratings yet
- Effects of Delayed Cord Clamping On The Third Stage of Labour, MaternalDocument4 pagesEffects of Delayed Cord Clamping On The Third Stage of Labour, MaternalmelatiNo ratings yet
- Ojog 2023071715223408Document12 pagesOjog 2023071715223408Julien BwamaNo ratings yet
- Kritika Poddar PDFDocument6 pagesKritika Poddar PDFmanish agrawalNo ratings yet
- Management of Third Stage of Labor: A Comparison of Intraumbilical Oxytocin and Placental Cord DrainageDocument8 pagesManagement of Third Stage of Labor: A Comparison of Intraumbilical Oxytocin and Placental Cord DrainageesterNo ratings yet
- Complementary Therapies in Clinical Practice: Raana Haj Najafi, Fan Xiao-NongDocument12 pagesComplementary Therapies in Clinical Practice: Raana Haj Najafi, Fan Xiao-NongSofiaNo ratings yet
- Metanalisis Carbetocina Vs OxiDocument7 pagesMetanalisis Carbetocina Vs OxiSergio ZhinaNo ratings yet
- Clinical Green Top Guidelines: 3.1 Using PostureDocument6 pagesClinical Green Top Guidelines: 3.1 Using PostureResti RusydiNo ratings yet
- Risk and Benefit of CSDocument22 pagesRisk and Benefit of CSbudi haryadiNo ratings yet
- Risk and Benefit of CSDocument22 pagesRisk and Benefit of CSbudi haryadiNo ratings yet
- Contraception: Erica P. Cahill, Andrea Henkel, Jonathan G. Shaw, Kate A. ShawDocument5 pagesContraception: Erica P. Cahill, Andrea Henkel, Jonathan G. Shaw, Kate A. ShawLinaMarcelaEcheverryBermudezNo ratings yet
- 08 Re-LaparotomyaftercesareanDocument8 pages08 Re-LaparotomyaftercesareanFarhanNo ratings yet
- Jurnal Obsgyn 2Document11 pagesJurnal Obsgyn 2hasrapriliana hersyaNo ratings yet
- Um - Haemorrhage/cd001337 - Diazv - Com/en/: SumberDocument4 pagesUm - Haemorrhage/cd001337 - Diazv - Com/en/: SumberrifkialbanaNo ratings yet
- 425-Article Text-1517-1-10-20210601Document7 pages425-Article Text-1517-1-10-20210601Power Electronics Lab IIT GuwahatiNo ratings yet
- OBSOS1Document6 pagesOBSOS1Bernas Arion NapitupuluNo ratings yet
- W 3 e WDDocument6 pagesW 3 e WDsupaidi97No ratings yet
- Long-Term Complications and Patient-Reported Outcomes After Alloplastic Breast ReconstructionDocument7 pagesLong-Term Complications and Patient-Reported Outcomes After Alloplastic Breast Reconstruction郭竹瑩No ratings yet
- PregnancyDocument5 pagesPregnancygabbbbbyNo ratings yet
- Prophylactic Uterine Artery Embolization in Second-Trimester Pregnancy Termination With Complete Placenta PreviaDocument8 pagesProphylactic Uterine Artery Embolization in Second-Trimester Pregnancy Termination With Complete Placenta PreviaAs AsNo ratings yet
- Clinical Study: Nitroglycerin For Management of Retained Placenta: A Multicenter StudyDocument7 pagesClinical Study: Nitroglycerin For Management of Retained Placenta: A Multicenter StudyTri Anna FitrianiNo ratings yet
- Bjo 12328Document12 pagesBjo 12328Afiqah So JasmiNo ratings yet
- Defining Failed Induction of LaborDocument10 pagesDefining Failed Induction of LaborOktaviani Dewi RatihNo ratings yet
- Ilyas 2019Document10 pagesIlyas 2019FebbyNo ratings yet
- The Effect of Birth Ball Exercises During PregnancDocument8 pagesThe Effect of Birth Ball Exercises During Pregnancmona khosraviNo ratings yet
- Insertion of An Intrauterine Contraceptive Device After Induced or Spontaneous Abortion: A Review of The EvidenceDocument6 pagesInsertion of An Intrauterine Contraceptive Device After Induced or Spontaneous Abortion: A Review of The EvidenceNi Wayan Ana PsNo ratings yet
- Complementary Therapies For Labour and Birth Study: A Randomised Controlled Trial of Antenatal Integrative Medicine For Pain Management in LabourDocument11 pagesComplementary Therapies For Labour and Birth Study: A Randomised Controlled Trial of Antenatal Integrative Medicine For Pain Management in LabourAini HiolaNo ratings yet
- Intrauterine Device Insertion During The Postpartum Period: A Systematic ReviewDocument10 pagesIntrauterine Device Insertion During The Postpartum Period: A Systematic ReviewRonald Ivan WijayaNo ratings yet
- Ijgo 12998Document7 pagesIjgo 12998el_dani_ellNo ratings yet
- Methods of Pushing During Vaginal Delivery and Pelvic Floor and Perineal Outcomes: A ReviewDocument7 pagesMethods of Pushing During Vaginal Delivery and Pelvic Floor and Perineal Outcomes: A ReviewToqa DabbasNo ratings yet
- Pemba GianDocument5 pagesPemba GianVito EtenioNo ratings yet
- Improvement and Effect of Stress Responses and Ovarian Reserve Function in Patients With Ovarian Cysts After Laparoscopic SurgeryDocument11 pagesImprovement and Effect of Stress Responses and Ovarian Reserve Function in Patients With Ovarian Cysts After Laparoscopic SurgerymadilaNo ratings yet
- ACOG 2009 Induction of LaborDocument12 pagesACOG 2009 Induction of LaborRiantiara PutrizaNo ratings yet
- Ijrcog-13090 oDocument4 pagesIjrcog-13090 oLakshmi RjNo ratings yet
- Synopsis For Foley Plus Miso Vs Miso Alone in Induction of LabourDocument5 pagesSynopsis For Foley Plus Miso Vs Miso Alone in Induction of LabourAshish TomarNo ratings yet
- WHO - Um Interventions For Preventing Shoulder DystociaDocument4 pagesWHO - Um Interventions For Preventing Shoulder Dystociavishramki2009No ratings yet
- Caesarean Delivery During Second Stage of Labor - A Study of Fetomaternal Outcome in A Tertiary Care HospitalDocument4 pagesCaesarean Delivery During Second Stage of Labor - A Study of Fetomaternal Outcome in A Tertiary Care HospitalIJAR JOURNALNo ratings yet
- Postpartum Hormonal Contraception in Breastfeeding Women: ReviewDocument6 pagesPostpartum Hormonal Contraception in Breastfeeding Women: ReviewmarialecifuentesbNo ratings yet
- Menopausal Symptoms and Surgical Complications After Opportunistic Bilateral Salpingectomy, A Register-Based Cohort StudyDocument10 pagesMenopausal Symptoms and Surgical Complications After Opportunistic Bilateral Salpingectomy, A Register-Based Cohort StudytriNo ratings yet
- Zipori 2018Document7 pagesZipori 2018Anonymous EmbvvI1ct2No ratings yet
- Ijgo 12687 PDFDocument6 pagesIjgo 12687 PDFDjlatino LatinoNo ratings yet
- Factores Predictores de Weaning de la VMDocument7 pagesFactores Predictores de Weaning de la VMJose NovoaNo ratings yet
- P10 Nejmoa1805489Document10 pagesP10 Nejmoa1805489SEPTIANA SAPUTRINo ratings yet
- Oxytocin Before Vs After Placental Delivery Prevent Postpartum HemorrhageDocument5 pagesOxytocin Before Vs After Placental Delivery Prevent Postpartum HemorrhageRafael MarvinNo ratings yet
- Labor Progression Sys Rev March 2023Document33 pagesLabor Progression Sys Rev March 2023Aníbal Paredes MerinoNo ratings yet
- Guideline For The Use of Antenatal Corticosteroids For Fetal MaturationDocument6 pagesGuideline For The Use of Antenatal Corticosteroids For Fetal MaturationValeria Balderrama ArgoteNo ratings yet
- Safety of The Balloon Catheter For Cervical Ripening in Outpatient Care Complicatios M DiederenDocument10 pagesSafety of The Balloon Catheter For Cervical Ripening in Outpatient Care Complicatios M DiederenMitsury Jacqueline Flores C.No ratings yet
- 1 s2.0 S0020729215003215 MainDocument5 pages1 s2.0 S0020729215003215 MainYudhi AuliaNo ratings yet
- Recent Advances in Endometrial CancerFrom EverandRecent Advances in Endometrial CancerSumita MehtaNo ratings yet
- Translational Research in Breast CancerFrom EverandTranslational Research in Breast CancerDong-Young NohNo ratings yet
- Open Abdomen: A Comprehensive Practical ManualFrom EverandOpen Abdomen: A Comprehensive Practical ManualFederico CoccoliniNo ratings yet
- The Roots of Modern Feminism: Mary Wollstonecraft and The French RevolutionDocument16 pagesThe Roots of Modern Feminism: Mary Wollstonecraft and The French RevolutionShirlya LimaNo ratings yet
- Troy-Bilt 019191 PDFDocument34 pagesTroy-Bilt 019191 PDFSteven W. NinichuckNo ratings yet
- G6 - Year End Exam (2018) - Southern Provincial Department of EducationDocument8 pagesG6 - Year End Exam (2018) - Southern Provincial Department of EducationXiao ShadowlordNo ratings yet
- علم الضحية) مفهوم جديد في العلوم الجنائية (و أين موقع المشرع الجزائري من دلك؟Document20 pagesعلم الضحية) مفهوم جديد في العلوم الجنائية (و أين موقع المشرع الجزائري من دلك؟sife fatahNo ratings yet
- Database Connectivity in PHP: PHP Tutorials by Vineet Kumar SainiDocument3 pagesDatabase Connectivity in PHP: PHP Tutorials by Vineet Kumar SainishamagondalNo ratings yet
- ALMMDocument16 pagesALMMJigar PatelNo ratings yet
- 5.5 CBM Waste Skip Open Top - POWER BearDocument1 page5.5 CBM Waste Skip Open Top - POWER Bearqtia71133No ratings yet
- Ashcroft Dial GaugeDocument1 pageAshcroft Dial GaugeReva Astra DiptaNo ratings yet
- DK Selling StrategiesDocument7 pagesDK Selling StrategiesMilan DzigurskiNo ratings yet
- Environmental Conservation in Bhutan: Organization and PolicyDocument21 pagesEnvironmental Conservation in Bhutan: Organization and PolicyApriele Rose Gaudicos HermogenesNo ratings yet
- Daniel Wahba - Optional Logarithmic AssigmentDocument6 pagesDaniel Wahba - Optional Logarithmic Assigmentdanielwahba2006No ratings yet
- 2014 Elec HD FS CKTruck 100713 ChevroletDocument247 pages2014 Elec HD FS CKTruck 100713 ChevroletREINALDO GONZALEZNo ratings yet
- Vdocuments - MX - Toyota 8fg45n Forklift Service Repair Manual 1608089928 PDFDocument23 pagesVdocuments - MX - Toyota 8fg45n Forklift Service Repair Manual 1608089928 PDFGUILHERME SANTOSNo ratings yet
- Project Product DescriptionDocument5 pagesProject Product Descriptionpruebaproiba12No ratings yet
- Le Wagon FullstackDocument23 pagesLe Wagon FullstackClara VaninaNo ratings yet
- 7SG18 - Solkor N Complete Technical Manual PDFDocument154 pages7SG18 - Solkor N Complete Technical Manual PDFmonikaNo ratings yet
- How To Choose The Right Cable GlandsDocument3 pagesHow To Choose The Right Cable GlandsRoger JohnNo ratings yet
- (Appendix 4A) Teacher Reflection Form For T I-III For RPMS SY 2021-2022Document10 pages(Appendix 4A) Teacher Reflection Form For T I-III For RPMS SY 2021-2022Quia Ferraren UmayaoNo ratings yet
- First Conditional ChainDocument3 pagesFirst Conditional ChainSonia DivileNo ratings yet
- What Are The Benefits of An Intensive Outpatient ProgramDocument1 pageWhat Are The Benefits of An Intensive Outpatient ProgramJack williamNo ratings yet
- Self-Efficacy Mediated Spiritual Leadership On Citizenship Behavior Towards The Environment of Employees at Harapan Keluarga HospitalDocument7 pagesSelf-Efficacy Mediated Spiritual Leadership On Citizenship Behavior Towards The Environment of Employees at Harapan Keluarga HospitalInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- Hindustan Lever: Case 15-4Document11 pagesHindustan Lever: Case 15-4anilnair88100% (1)
- Leading Workplace CommunicationDocument26 pagesLeading Workplace CommunicationEahbm KaduNo ratings yet
- Bert Meulendijk Rig Pack IDocument1 pageBert Meulendijk Rig Pack IMorrisNo ratings yet
- MKT Marunda Center ProfileDocument47 pagesMKT Marunda Center ProfileMuhammad AbidinNo ratings yet
- ASTM Rapid Sugar Test For LimeDocument5 pagesASTM Rapid Sugar Test For LimeJose PerezNo ratings yet
- Philosophy of Educationsample Isms With Answersclue KeywordpdfDocument16 pagesPhilosophy of Educationsample Isms With Answersclue KeywordpdfScribdNo ratings yet
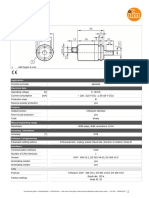
- Multiturn Solid Shaft Encoder: 1 M4 Depth 6 MMDocument2 pagesMultiturn Solid Shaft Encoder: 1 M4 Depth 6 MMSoha EzzaldenNo ratings yet
- CS 123 I2P Assignment 2Document3 pagesCS 123 I2P Assignment 2Hafiz AbdullahNo ratings yet
- Limbo PowerpointDocument10 pagesLimbo Powerpointapi-693306390No ratings yet