Download as pdf or txt
You might also like
- Advance Baking CompilationDocument44 pagesAdvance Baking CompilationCherry Brutas100% (1)
- Global Public Health: Click To Edit Master Title StyleDocument77 pagesGlobal Public Health: Click To Edit Master Title StyleDono WidiatmokoNo ratings yet
- Meta-Analysis of Prednisone For Rheumatoid Arthritis: Am Fam Physician. 1998 Aug 1 58 (2) :554-561Document9 pagesMeta-Analysis of Prednisone For Rheumatoid Arthritis: Am Fam Physician. 1998 Aug 1 58 (2) :554-561Nabila Annisa PraditiaNo ratings yet
- Papadopoulos 2003Document5 pagesPapadopoulos 2003Mia ZahirNo ratings yet
- Simple Clinical Indicators For Early Psoriatic Arthritis Detection.Document3 pagesSimple Clinical Indicators For Early Psoriatic Arthritis Detection.pancholarpancholarNo ratings yet
- Anti-Mutated Citrullinated Vimentin Antibodies in Rheumatoid ArthritisDocument17 pagesAnti-Mutated Citrullinated Vimentin Antibodies in Rheumatoid ArthritisReda RamzyNo ratings yet
- The New ACR/EULAR Criteria For Rheumatoid Arthritis Can Identify Patients With Same Disease Activity But Less Damage by UltrasoundDocument4 pagesThe New ACR/EULAR Criteria For Rheumatoid Arthritis Can Identify Patients With Same Disease Activity But Less Damage by UltrasoundFajri WardiannurNo ratings yet
- Art 1780280905 PDFDocument8 pagesArt 1780280905 PDFIesna NaNo ratings yet
- Brunner Et AlDocument8 pagesBrunner Et AlOla OlaNo ratings yet
- 2 Moduli FULL-2225 - Basic LearningDocument27 pages2 Moduli FULL-2225 - Basic LearningNaziBrola TsivadzeNo ratings yet
- ArtritisDocument131 pagesArtritisricharddocumNo ratings yet
- Systematic Literature Review Rheumatoid ArthritisDocument8 pagesSystematic Literature Review Rheumatoid ArthritisafmzaoahmicfxgNo ratings yet
- Original Article Study of Advanced Rheumatoid ArthritisDocument10 pagesOriginal Article Study of Advanced Rheumatoid ArthritisOcef GrahastamaNo ratings yet
- Wang 2019Document9 pagesWang 2019Maida FitrianiNo ratings yet
- Literature Review On Rheumatoid ArthritisDocument6 pagesLiterature Review On Rheumatoid Arthritispib0b1nisyj2100% (1)
- Key Challenges in Rheumatic and Musculoskeletal Disease Translational ResearchDocument2 pagesKey Challenges in Rheumatic and Musculoskeletal Disease Translational ResearchAzzam KhoirulNo ratings yet
- Management of Rheumatoid Arthritis: Consensus Recommendations From The Hong Kong Society of RheumatologyDocument11 pagesManagement of Rheumatoid Arthritis: Consensus Recommendations From The Hong Kong Society of RheumatologyMakhyan JibrilNo ratings yet
- Diagnostic Performance of The ACR/EULAR 2010 Criteria For Rheumatoid Arthritis and Two Diagnostic Algorithms in An Early Arthritis Clinic (REACH)Document3 pagesDiagnostic Performance of The ACR/EULAR 2010 Criteria For Rheumatoid Arthritis and Two Diagnostic Algorithms in An Early Arthritis Clinic (REACH)Daniel Manay GuadalupeNo ratings yet
- Recuero 2014Document1 pageRecuero 20142dradhtiphonephotosbackupNo ratings yet
- Imaging Modalities For The Classification of Gout Systematic Literature Review and Meta-AnalysisDocument7 pagesImaging Modalities For The Classification of Gout Systematic Literature Review and Meta-Analysisea793wszNo ratings yet
- Classification and Epidemiology of Rheumatoid ArthritisDocument7 pagesClassification and Epidemiology of Rheumatoid ArthritisHebert Aldo SalazarNo ratings yet
- 10.1007@s12028 018 0549 1Document6 pages10.1007@s12028 018 0549 1santpiedra7No ratings yet
- Prevalence of Signs and Symptoms of Temporomandibular Disorders in Patients With Different Rheumatic Diseases 1Document10 pagesPrevalence of Signs and Symptoms of Temporomandibular Disorders in Patients With Different Rheumatic Diseases 1Athenaeum Scientific PublishersNo ratings yet
- 1443 3 FullDocument2 pages1443 3 FullmuamarrayNo ratings yet
- Poster Viewing I Tuesday 1 May 2018 Iii75Document2 pagesPoster Viewing I Tuesday 1 May 2018 Iii75Firdaus Septhy ArdhyanNo ratings yet
- Med Ultrason - 2017 - 19 - 2 - 166 - 171 - ARTICOL RA33Document6 pagesMed Ultrason - 2017 - 19 - 2 - 166 - 171 - ARTICOL RA33Boldeanu MVNo ratings yet
- Izquierdo Et Al-2015-Brain and BehaviorDocument9 pagesIzquierdo Et Al-2015-Brain and Behaviorantonio_ruiz_77No ratings yet
- Real World Effectiveness and Safety of Rituximab in The Treatment of Rheumatoid Arthritis: A Single Center Experience in TaiwanDocument9 pagesReal World Effectiveness and Safety of Rituximab in The Treatment of Rheumatoid Arthritis: A Single Center Experience in TaiwanTengku M Ridho AnharNo ratings yet
- Relationship Between Sleep, Pain and Inflammatory Markers in Patients With Rheumatoid ArthritisDocument7 pagesRelationship Between Sleep, Pain and Inflammatory Markers in Patients With Rheumatoid Arthritisaria tristayanthiNo ratings yet
- Journal of NephropharmacologyDocument8 pagesJournal of NephropharmacologykiranNo ratings yet
- L4. T2.M2 y M6. Predictive Factors For Induction of Remission in Patients With Active ARDocument5 pagesL4. T2.M2 y M6. Predictive Factors For Induction of Remission in Patients With Active ARJhon Andy RamosNo ratings yet
- Diacerein For The Treatment of Rheumatoid Arthritis in Patients With Inadequate Response To Methotrexate A Pilot Randomized, Double-Blind, Placebo-Controlled Add-On Trial - TEM HTMLDocument11 pagesDiacerein For The Treatment of Rheumatoid Arthritis in Patients With Inadequate Response To Methotrexate A Pilot Randomized, Double-Blind, Placebo-Controlled Add-On Trial - TEM HTMLAline Leal CortesNo ratings yet
- 2848-Article Text-5618-1-10-20221227Document7 pages2848-Article Text-5618-1-10-20221227Mahdi AkbariNo ratings yet
- Clinical Impact of External Radiotherapy in Non-Metastatic Esophageal Cancer According To Histopathological SubtypeDocument12 pagesClinical Impact of External Radiotherapy in Non-Metastatic Esophageal Cancer According To Histopathological SubtypesilviailieNo ratings yet
- Anti CCP, FR, VSG PCRDocument6 pagesAnti CCP, FR, VSG PCRjuanabNo ratings yet
- Best Practice & Research Clinical Rheumatology: Diane Van Der Woude, Annette H.M. Van Der Helm-Van MilDocument14 pagesBest Practice & Research Clinical Rheumatology: Diane Van Der Woude, Annette H.M. Van Der Helm-Van MilasmaNo ratings yet
- ARTRITISDocument4 pagesARTRITISmayra26olivaresNo ratings yet
- SBR2018 - AbstractsDocument115 pagesSBR2018 - AbstractsGustavo ResendeNo ratings yet
- The "Trea T To Ta Rge T" (17415)Document18 pagesThe "Trea T To Ta Rge T" (17415)YoaAguilarCastilloNo ratings yet
- 1-Med Familiar 2018 Giannoula Short Course Antibiotic Terapia RS MADocument13 pages1-Med Familiar 2018 Giannoula Short Course Antibiotic Terapia RS MALes DSNo ratings yet
- Meta-Analysis: Psoriatic Arthritis Screening: A Systematic Review and Meta-AnalysisDocument16 pagesMeta-Analysis: Psoriatic Arthritis Screening: A Systematic Review and Meta-AnalysisireneardianiNo ratings yet
- Diagnosing Late Onset Rheumatoid Arthritis, Polymyalgia Rheumatica, and Temporal Arteritis in Patients Presenting With..Document5 pagesDiagnosing Late Onset Rheumatoid Arthritis, Polymyalgia Rheumatica, and Temporal Arteritis in Patients Presenting With..Ronny IswahyudiNo ratings yet
- Early Atherosclerosis in Rheumatoid Arthritis: A Case Control StudyDocument5 pagesEarly Atherosclerosis in Rheumatoid Arthritis: A Case Control StudychandanNo ratings yet
- 2017 TROZAK in IcelandDocument7 pages2017 TROZAK in IcelandmaomaochongNo ratings yet
- Low Skeletal Muscle Is Associatd With ToxicityDocument6 pagesLow Skeletal Muscle Is Associatd With ToxicityAna Leticia RibeiroNo ratings yet
- The Impact of Age On Activity Index and Patient Reported Outcomes in Patients With Sjogren's SyndromeDocument4 pagesThe Impact of Age On Activity Index and Patient Reported Outcomes in Patients With Sjogren's SyndromebijgimNo ratings yet
- The Relationship of Rheumatoid Factor With Disease Activity in Patients With Rheumatoid ArthritisDocument3 pagesThe Relationship of Rheumatoid Factor With Disease Activity in Patients With Rheumatoid ArthritisGusti Ngurah DwiantaraNo ratings yet
- 260-Main Manuscript-1507-1-10-20220620Document5 pages260-Main Manuscript-1507-1-10-20220620hilman lesmanaNo ratings yet
- TOR SEMNAS KARAkTER 4 2018Document6 pagesTOR SEMNAS KARAkTER 4 2018Rosyid PrasetyoNo ratings yet
- Reference 333Document123 pagesReference 333sabrinaNo ratings yet
- Does Ramadan Fasting Increase Acute Upper Gastrointestinal Haemorrhage?Document6 pagesDoes Ramadan Fasting Increase Acute Upper Gastrointestinal Haemorrhage?Circle A 2009No ratings yet
- Work Ability in Healthcare Workers (HCWS) After Breast Cancer: Preliminary Data of A Pilot StudyDocument9 pagesWork Ability in Healthcare Workers (HCWS) After Breast Cancer: Preliminary Data of A Pilot StudyFirdaus BambooNo ratings yet
- 576 Friday, 15 June 2018 Scientific AbstractsDocument2 pages576 Friday, 15 June 2018 Scientific AbstractsDanna Carvajal GaitanNo ratings yet
- Jaundice in Adult Patients Above 50 Years of Age ADocument5 pagesJaundice in Adult Patients Above 50 Years of Age AAndrew RajNo ratings yet
- Head-to-Head Comparison of Subcutaneous Abatacept Versus Adalimumab For Rheumatoid ArthritisDocument11 pagesHead-to-Head Comparison of Subcutaneous Abatacept Versus Adalimumab For Rheumatoid ArthritislilingNo ratings yet
- BMC - GcaDocument7 pagesBMC - GcaMuhammad Imran MirzaNo ratings yet
- Evaluation of 880 Patients Diagnosed With Acute Pancreatitis According To The Revised Atlanta Classification: A Single-Center ExperienceDocument6 pagesEvaluation of 880 Patients Diagnosed With Acute Pancreatitis According To The Revised Atlanta Classification: A Single-Center ExperienceGabriel PessoaNo ratings yet
- Usos Anti TNFDocument7 pagesUsos Anti TNFostosjesus4824No ratings yet
- NASKAH+PUBLIKASI+hipertensi+ (2) Id En+Document8 pagesNASKAH+PUBLIKASI+hipertensi+ (2) Id En+Nawang DpNo ratings yet
- Role of Serum and Synovial Procalcitonin in Differentiating Septic From Non-Septic Arthritis - A Prospective StudyDocument6 pagesRole of Serum and Synovial Procalcitonin in Differentiating Septic From Non-Septic Arthritis - A Prospective StudyAngela Villanueva SocolaNo ratings yet
- Complementary and Alternative Medical Lab Testing Part 3: CardiologyFrom EverandComplementary and Alternative Medical Lab Testing Part 3: CardiologyRating: 1 out of 5 stars1/5 (1)
- OCEANSDocument4 pagesOCEANSamna hamidNo ratings yet
- Dangase Group - Research FinalDocument59 pagesDangase Group - Research FinalGlenda PapelleroNo ratings yet
- TOT Water For Pharmaceutical Use - Part 1Document132 pagesTOT Water For Pharmaceutical Use - Part 1Delly AnakAfternoonyesterdays0% (1)
- Safety Alert 365 Bsee Identified Grating and Open Hole Hazards During Risk Based InspectionsDocument3 pagesSafety Alert 365 Bsee Identified Grating and Open Hole Hazards During Risk Based Inspectionsi.kamalNo ratings yet
- Analysis of Financial StatementsDocument46 pagesAnalysis of Financial StatementsSwaroop Ranjan Baghar25% (4)
- Sepharial - The Science of Foreknowledge Cd13 Id 1928069166 Size603Document114 pagesSepharial - The Science of Foreknowledge Cd13 Id 1928069166 Size603makarandmone100% (9)
- The Seven Types of Yellow Sapphire and Their Stability To Light PDFDocument10 pagesThe Seven Types of Yellow Sapphire and Their Stability To Light PDFdebjeet royNo ratings yet
- The Cost of Goods Sold For The Month of December: Excel Professional Services, IncDocument4 pagesThe Cost of Goods Sold For The Month of December: Excel Professional Services, IncmatildaNo ratings yet
- Dark Energy and Dark MatterDocument26 pagesDark Energy and Dark MattersaphirehaelNo ratings yet
- IP Rating ChartDocument5 pagesIP Rating Charthemant kumarNo ratings yet
- STC1 S2 Slickline I v.2Document165 pagesSTC1 S2 Slickline I v.2Siew Qian100% (1)
- Pumy-P36 48nhmu Tech&Service Oc366c 7-25-08Document100 pagesPumy-P36 48nhmu Tech&Service Oc366c 7-25-08Chris KokkarasNo ratings yet
- Pairing Scheme 1st Year 2024 BY PHYSICS INN ACDEMIA M.A. JAVEDDocument1 pagePairing Scheme 1st Year 2024 BY PHYSICS INN ACDEMIA M.A. JAVEDabdull phyNo ratings yet
- Basic Accounting - Final ExaminationDocument5 pagesBasic Accounting - Final ExaminationLaira Diana RamosNo ratings yet
- Activity 6Document4 pagesActivity 6Junior SmithNo ratings yet
- Shreya Shukla Case Study-2Document41 pagesShreya Shukla Case Study-2Rishabh UpadhyayNo ratings yet
- Market Structure and Market PerformanceDocument22 pagesMarket Structure and Market PerformanceAishwarya SudhirNo ratings yet
- Assembly of PartsDocument29 pagesAssembly of PartsthirumalaikumaranNo ratings yet
- Articulo-Watson Crick PDFDocument2 pagesArticulo-Watson Crick PDFAjedrez ItineranteNo ratings yet
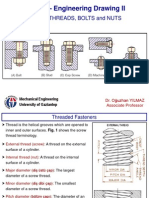
- SCREW THREADS, BOLTS and NUTS PDFDocument10 pagesSCREW THREADS, BOLTS and NUTS PDFhrhgk50% (2)
- BELSummer Training ReportDocument33 pagesBELSummer Training ReportPalak MeenaNo ratings yet
- Spe 199993 MSDocument28 pagesSpe 199993 MSHussam AgabNo ratings yet
- Sony Hcd-Bx6av Dx6avDocument64 pagesSony Hcd-Bx6av Dx6avFrancisco ParedesNo ratings yet
- Materials Science II Chapter 10Document41 pagesMaterials Science II Chapter 10Rebeca CremonezNo ratings yet
- Analysis of Defects in Clean Fabrication Process of Friction Stir WeldingDocument10 pagesAnalysis of Defects in Clean Fabrication Process of Friction Stir WeldingV.v. TaguisNo ratings yet
- 02 - Virtualisation and NetworkingDocument63 pages02 - Virtualisation and Networkingvecanoc954No ratings yet
- Deep Nightly FathomsDocument44 pagesDeep Nightly FathomsMaria Guarneri67% (3)
- Problem SetDocument12 pagesProblem SetJohn Lade Tan NacionalNo ratings yet