Download as pdf or txt
You might also like
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5823)
- Alexander's Care of The Patient in Surgery by Rothrock (17th Edition)Document1,217 pagesAlexander's Care of The Patient in Surgery by Rothrock (17th Edition)ezinne obinna-uma100% (1)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1093)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (852)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (590)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (898)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (541)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (349)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (823)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (122)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (403)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- Ashcraft's Pediatric Surgery 6Document1,161 pagesAshcraft's Pediatric Surgery 6Ismail Muhammad95% (19)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (74)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- LST 2009 Surgical Safety Check List (Australia and New Zealand) PDFDocument1 pageLST 2009 Surgical Safety Check List (Australia and New Zealand) PDFaskjhwiuehNo ratings yet
- Medical Terminology STUDY GUIDE J23Document99 pagesMedical Terminology STUDY GUIDE J23Waikiki FisherNo ratings yet
- Dex in Tap BlockDocument12 pagesDex in Tap Blockamostafa.betaNo ratings yet
- MAE 82: Mathematics of Engineering: Prof. Tyler ClitesDocument31 pagesMAE 82: Mathematics of Engineering: Prof. Tyler ClitesshivaNo ratings yet
- Or Tour: Front DeskDocument4 pagesOr Tour: Front DeskTomato MenudoNo ratings yet
- Position and Competency ProfileDocument9 pagesPosition and Competency Profilejay jayNo ratings yet
- Multiple Choice Question Examination Specifications: Australian Medical Council Limited December 2020Document26 pagesMultiple Choice Question Examination Specifications: Australian Medical Council Limited December 2020TSZ-SHAN MYRA FUNG100% (1)
- Implant Placement Procedure - One Stage VS Two StageDocument6 pagesImplant Placement Procedure - One Stage VS Two StageMirela BurciuNo ratings yet
- (Craig Liebenson) Rehabilitation of The SpineDocument428 pages(Craig Liebenson) Rehabilitation of The SpineGeorge Ciuca82% (11)
- A5 Brochure - Revise - Centre Pinning - With IndoscopeDocument32 pagesA5 Brochure - Revise - Centre Pinning - With IndoscopeGerman DrumsNo ratings yet
- Straumann Dental System Map BoneLevelProstheticsDocument1 pageStraumann Dental System Map BoneLevelProstheticscarla1315No ratings yet
- Generic Root FormDocument9 pagesGeneric Root FormLAKSHMI ARORANo ratings yet
- MSC - Medical Surgical Sub Specialty Cardiovascular Thoracic Nursing PDFDocument44 pagesMSC - Medical Surgical Sub Specialty Cardiovascular Thoracic Nursing PDFAlma Susan100% (4)
- Brigham & Women's Hospital - Elbow & Hand Rehabilitation PT ProtocolsDocument25 pagesBrigham & Women's Hospital - Elbow & Hand Rehabilitation PT ProtocolsShrutiNo ratings yet
- Insurance IdDocument1 pageInsurance IdEstrella Cotrina RojasNo ratings yet
- Kardex: Mental Status: Activities: Diet: Tubes: Special InfoDocument3 pagesKardex: Mental Status: Activities: Diet: Tubes: Special InfoRyrey Abraham PacamanaNo ratings yet
- Local Anesthetic Systemic ToxicityDocument1 pageLocal Anesthetic Systemic Toxicitylaurad.benavidesNo ratings yet
- Dermatology FinalDocument16 pagesDermatology FinalMelinda100% (2)
- Hamstring Muscle Injuries - OrthoInfo - AAOSDocument8 pagesHamstring Muscle Injuries - OrthoInfo - AAOSAndy Delos ReyesNo ratings yet
- Lung Cancer Treatment GuidelinesDocument6 pagesLung Cancer Treatment GuidelinesPeterpan NguyenNo ratings yet
- Hospital in Whitefield, BangaloreDocument6 pagesHospital in Whitefield, BangaloreColumbia Asia Hospitals in IndiaNo ratings yet
- Principles of Surgery: The Two Principal Requirements (1) Adequate Visibility (2) AssistanceDocument16 pagesPrinciples of Surgery: The Two Principal Requirements (1) Adequate Visibility (2) AssistanceVijay K PatelNo ratings yet
- Bupa CarePro Consolidated 2017Document30 pagesBupa CarePro Consolidated 2017SSNo ratings yet
- Leanne Ard Mader RN, BSN, CCRNDocument3 pagesLeanne Ard Mader RN, BSN, CCRNapi-268353097No ratings yet
- Vascular TraumaDocument16 pagesVascular TraumaAndi Suchy Qumala SarieNo ratings yet
- 2015parathyroid Carcinoma Challenges in Diagnosis and TreatmentDocument9 pages2015parathyroid Carcinoma Challenges in Diagnosis and TreatmentCharley WangNo ratings yet
- Intestinal Obstruction AditiDocument67 pagesIntestinal Obstruction Aditiaditi BahugunaNo ratings yet
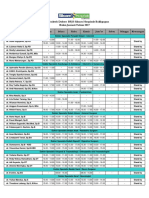
- Januari 2017 - Jadwal Praktek Klinik BPJS Kesehatan PDFDocument2 pagesJanuari 2017 - Jadwal Praktek Klinik BPJS Kesehatan PDFVirly EffendiNo ratings yet