Download as docx, pdf, or txt
You might also like
- Readers Theater Life FlightDocument5 pagesReaders Theater Life FlightCaurrine Monsalud93% (14)
- Anterior Triangle of The Neck: James Taclin C. Banez, MD, FPSGS, FPCSDocument40 pagesAnterior Triangle of The Neck: James Taclin C. Banez, MD, FPSGS, FPCSPrecious MedinaNo ratings yet
- I Ching Acupuncture The Balance MethodDocument14 pagesI Ching Acupuncture The Balance MethodMaria Agustina Flores de Seguela100% (2)
- Ear AntomyDocument19 pagesEar Antomyhadeelnazar12No ratings yet
- Laughing Is Also Good For Your Respiratory System!Document5 pagesLaughing Is Also Good For Your Respiratory System!A-Naeem To'mah Al-sawaieNo ratings yet
- (9-2) THT - KL Anatomi 2020Document88 pages(9-2) THT - KL Anatomi 2020ayurhrdiniNo ratings yet
- Respiratory System: I. Olfactory CellsDocument10 pagesRespiratory System: I. Olfactory CellsTJ HarrisNo ratings yet
- Anatomy and Embryology of The Pharynx1Document27 pagesAnatomy and Embryology of The Pharynx1daw022No ratings yet
- Anatomy of Ear FinalDocument61 pagesAnatomy of Ear FinalRavi KushwahaNo ratings yet
- Lab Module Activity Respiratory SystemDocument8 pagesLab Module Activity Respiratory SystemJecel LazarraNo ratings yet
- Anatomy and Embryology of The Pharynx1Document27 pagesAnatomy and Embryology of The Pharynx1Немосјановић ЋудмилаNo ratings yet
- Anatomy and Embryology of The Pharynx1.ppsDocument27 pagesAnatomy and Embryology of The Pharynx1.ppsНемосјановић ЋудмилаNo ratings yet
- 1 RHINOLOGY NoseDocument116 pages1 RHINOLOGY NoseWai Kwong ChiuNo ratings yet
- Airway Mngt. Module 1.Document11 pagesAirway Mngt. Module 1.marc gorospeNo ratings yet
- Pharynx NotesDocument8 pagesPharynx Notesm0rat0r1umNo ratings yet
- Larynx (Anatomy, Laryngomalacia, Laryngeal Web)Document12 pagesLarynx (Anatomy, Laryngomalacia, Laryngeal Web)Saya MenangNo ratings yet
- Anatomy and Physiology of Respiratory SystemDocument21 pagesAnatomy and Physiology of Respiratory Systemsameeha semiNo ratings yet
- Respiratory System-2cgf2Document42 pagesRespiratory System-2cgf2Nzenwa Jedidiah KimizuNo ratings yet
- Compendium 4Document13 pagesCompendium 4Samha MahboubNo ratings yet
- Sensory Organs - NoseDocument24 pagesSensory Organs - Noseapi-324160601No ratings yet
- Respiratory SystemDocument55 pagesRespiratory SystemSitotaye DinkuNo ratings yet
- Modul Anatomi Blok 11Document40 pagesModul Anatomi Blok 11AyuNo ratings yet
- Week 3 Respiratory SystemDocument10 pagesWeek 3 Respiratory SystemangeliaNo ratings yet
- Anatomy of Respiratory System: Moderator: Dr. Aruna Speaker:Dr - Vipin KR - SinghDocument69 pagesAnatomy of Respiratory System: Moderator: Dr. Aruna Speaker:Dr - Vipin KR - SinghAnshul JainNo ratings yet
- Prof. Hamiadji - Ear, Nose, Throat PDFDocument28 pagesProf. Hamiadji - Ear, Nose, Throat PDFSANDA NABILAH FATINNo ratings yet
- 11 Respiratory Pharma PrintDocument53 pages11 Respiratory Pharma Printabenezer isayasNo ratings yet
- DR - Rimpy Bhuyan Trihms.Document63 pagesDR - Rimpy Bhuyan Trihms.DIKSHA RANI DEKANo ratings yet
- Anatomy and Physiology THT - Dr. AriefDocument88 pagesAnatomy and Physiology THT - Dr. AriefGilbert Sterling OctaviusNo ratings yet
- PharyngitisDocument76 pagesPharyngitisAhmed ZakiNo ratings yet
- Lecture 1structure & Function of Respiratory System Nose & Paranasal SinusesDocument7 pagesLecture 1structure & Function of Respiratory System Nose & Paranasal Sinusesadham bani younesNo ratings yet
- Human Ear PPTDocument10 pagesHuman Ear PPTsuman.sk3299No ratings yet
- Head Features: SkullDocument41 pagesHead Features: SkullAnne-Sophie BeduNo ratings yet
- 6theear 100505202518 Phpapp01Document30 pages6theear 100505202518 Phpapp01Marjan MarolovNo ratings yet
- Repiratory System Concept Rna NotesDocument21 pagesRepiratory System Concept Rna NotesArpan BhadrawalNo ratings yet
- Parts of The Respiratory System & Their FunctionsDocument38 pagesParts of The Respiratory System & Their FunctionsSaajid AmraNo ratings yet
- Krishna Reddy Anatomy of PharynxDocument20 pagesKrishna Reddy Anatomy of PharynxSiva ramaNo ratings yet
- 1.anatomy of Respiratory SystemDocument73 pages1.anatomy of Respiratory Systemokoti.omutanyi22No ratings yet
- Airway and Its Maintenance Hand Out2Document49 pagesAirway and Its Maintenance Hand Out2agatakassaNo ratings yet
- Anatomy of Larynx Lecture 7Document21 pagesAnatomy of Larynx Lecture 7sallykamareddine100% (1)
- NCM 112 LEC Topic 1 Respiratory System Anatomy PhysiologyDocument7 pagesNCM 112 LEC Topic 1 Respiratory System Anatomy PhysiologyViviene Faye FombuenaNo ratings yet
- LarynxDocument28 pagesLarynxwfvtdpngdtNo ratings yet
- The Pharyngeal Arches - Clefts - Pouches - Embryology - TeachMeAnatomyDocument4 pagesThe Pharyngeal Arches - Clefts - Pouches - Embryology - TeachMeAnatomypinkrawpineappleNo ratings yet
- Anatomy EarDocument20 pagesAnatomy EarRod HilalNo ratings yet
- Chapter 22 Notes Respiratory SystemDocument36 pagesChapter 22 Notes Respiratory SystemMarilia BonorinoNo ratings yet
- Anatomy - Lecture 1Document9 pagesAnatomy - Lecture 1Ana AbuladzeNo ratings yet
- Telinga Hidung TenggorokanDocument111 pagesTelinga Hidung Tenggorokanharyo wiryantoNo ratings yet
- SST Paper FinalDocument7 pagesSST Paper FinalCarla Vestal- LassoNo ratings yet
- Respiratory SystemDocument54 pagesRespiratory SystemEndin Nokik StujannaNo ratings yet
- Lecture 11 PDFDocument5 pagesLecture 11 PDFA-Naeem To'mah Al-sawaieNo ratings yet
- Anatomy and Physiology of NoseDocument29 pagesAnatomy and Physiology of NoseNur100% (1)
- Respiratory SystemDocument12 pagesRespiratory SystemshreyacrkNo ratings yet
- Anatomy of The Throat DR Oscar PresentasiDocument53 pagesAnatomy of The Throat DR Oscar Presentasiharyo wiryantoNo ratings yet
- Daphne Ganancial Janine Villas John Rev Lorenzo DDM Iii-BDocument57 pagesDaphne Ganancial Janine Villas John Rev Lorenzo DDM Iii-BDaphne GanancialNo ratings yet
- LBM 5 THT SGD 15Document42 pagesLBM 5 THT SGD 15Akhmad Ulil AlbabNo ratings yet
- Respiratory System5Document24 pagesRespiratory System5api-19641337No ratings yet
- Sensory Organs - EarsDocument37 pagesSensory Organs - Earsapi-324160601No ratings yet
- EMB5, PDFDocument7 pagesEMB5, PDFSafura IjazNo ratings yet
- LO SSS Week 5Document8 pagesLO SSS Week 5Tony StarkNo ratings yet
- Respiratory System 1 1Document24 pagesRespiratory System 1 1mmaccidobadamasiNo ratings yet
- RT 105 Prefinal NotesDocument24 pagesRT 105 Prefinal NotesLouiseNo ratings yet
- Exterior and Middle EarDocument26 pagesExterior and Middle EarAndra BauerNo ratings yet
- Greenhouse Manual2Document106 pagesGreenhouse Manual2Amit ShresthaNo ratings yet
- Mark Scheme (Results) : Summer 2018 Pearson Edexcel International GCSE in Further Pure Mathematics (4PM0) Paper 01Document26 pagesMark Scheme (Results) : Summer 2018 Pearson Edexcel International GCSE in Further Pure Mathematics (4PM0) Paper 01Newton JohnNo ratings yet
- The Expanding Universe - Sir Arthur Stanley Eddington - Cambridge University Press - 1987Document153 pagesThe Expanding Universe - Sir Arthur Stanley Eddington - Cambridge University Press - 1987cramerps2084No ratings yet
- Consolidated Company List December 2018Document478 pagesConsolidated Company List December 2018Rishabh GhaiNo ratings yet
- The Pisces Sagittarius SquareDocument3 pagesThe Pisces Sagittarius SquarejakilaNo ratings yet
- OfficialRules-BritneySpearsNYE CRDocument9 pagesOfficialRules-BritneySpearsNYE CRAbelardo Ch.No ratings yet
- UP Evidence PrimerDocument25 pagesUP Evidence PrimerSuiNo ratings yet
- Decisions (IELTS Speaking Part 2-3)Document3 pagesDecisions (IELTS Speaking Part 2-3)Yassine MafraxNo ratings yet
- West Indies Cricket BibliographyDocument20 pagesWest Indies Cricket BibliographyAminaNo ratings yet
- CDHA Infection ControlDocument2 pagesCDHA Infection ControlAliaa El WakeelNo ratings yet
- Banking Law On Secrecy of Bank DepositsDocument29 pagesBanking Law On Secrecy of Bank DepositsbrendamanganaanNo ratings yet
- Annexure 6.0 Candidate InstructionsDocument8 pagesAnnexure 6.0 Candidate Instructionschiluverushivaprasad02No ratings yet
- Rekayasa IdeDocument21 pagesRekayasa IdelilyNo ratings yet
- MYCOBIT Control Objective Assessment FormsDocument5 pagesMYCOBIT Control Objective Assessment FormsRafasaxNo ratings yet
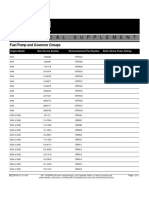
- FuelPump&GovernorGroups SELD0135 11Document11 pagesFuelPump&GovernorGroups SELD0135 11narit00007No ratings yet
- Purchase Order: NPWP: 03.343.037.2-047.000 12208599Document2 pagesPurchase Order: NPWP: 03.343.037.2-047.000 12208599Oscar OkkyNo ratings yet
- (With Script) June 2021 Saturday WSF Teaching GuideDocument3 pages(With Script) June 2021 Saturday WSF Teaching GuideMichael T. BelloNo ratings yet
- Britannica Childrens Encyclopedia 2007Document1 pageBritannica Childrens Encyclopedia 2007Marius AndreiNo ratings yet
- Reflective Competency Statement IIIDocument4 pagesReflective Competency Statement IIIapi-534821343No ratings yet
- Classroom ArrangementsDocument5 pagesClassroom Arrangementsapi-427868008No ratings yet
- Mole Concept DPP-2 - 501352Document1 pageMole Concept DPP-2 - 501352Vatsal BhargavaNo ratings yet
- Book of Abstracts-ArushaDocument250 pagesBook of Abstracts-ArushaBassam Yahay IbraheemNo ratings yet
- Shark ClassificationDocument44 pagesShark ClassificationSheeka TareyamaNo ratings yet
- Mumbai Construction Circle, Chembur D.S.R. FOR THE YEAR 2012-2013 NotesDocument3 pagesMumbai Construction Circle, Chembur D.S.R. FOR THE YEAR 2012-2013 Notesshantanu kulkarniNo ratings yet
- Angles and Directions SurveyingDocument23 pagesAngles and Directions SurveyingAbel AmmoNo ratings yet
- 17 Artikel Analisis Komponen Produk Wisata Di Kabupaten KarawangDocument10 pages17 Artikel Analisis Komponen Produk Wisata Di Kabupaten KarawangPutri NurkarimahNo ratings yet
- Floyd Edwrads Memorial Scholarship Terms of Reference 2017Document3 pagesFloyd Edwrads Memorial Scholarship Terms of Reference 2017Aswin HarishNo ratings yet
- Laurie Baker: (The Brick Master of Kerala)Document8 pagesLaurie Baker: (The Brick Master of Kerala)Malik MussaNo ratings yet