Download as pdf or txt
You might also like
- 06 Manus Sedlacek 1 Background Document To en 1991 Part 2 - Traffic Loads For Road BridgesDocument109 pages06 Manus Sedlacek 1 Background Document To en 1991 Part 2 - Traffic Loads For Road Bridgesdimitrios25100% (1)
- Porsche 912E Service InformationDocument47 pagesPorsche 912E Service InformationOscar Hamer100% (1)
- C72 Steel - 2Document4 pagesC72 Steel - 2Bruno Cavalcante0% (1)
- Biomaterials Quick Study SheetDocument2 pagesBiomaterials Quick Study SheetWilliam ChanNo ratings yet
- Effectiveness of Bolus Administration of Continuous Intravenous Lidocaine On Pain Intensity After Mastectomy SurgeryDocument6 pagesEffectiveness of Bolus Administration of Continuous Intravenous Lidocaine On Pain Intensity After Mastectomy SurgeryInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- Analgesic Effects and Adverse Reactions of LidocaiDocument6 pagesAnalgesic Effects and Adverse Reactions of Lidocaibrendastevany23No ratings yet
- Does Intravenous Low Dose Dexmedetomidine Supplementation Has Beneficial Effects On Spinal Anaesthesia?Document4 pagesDoes Intravenous Low Dose Dexmedetomidine Supplementation Has Beneficial Effects On Spinal Anaesthesia?MOHAMMED IQBALNo ratings yet
- 2264-Article Text-5024-4-10-20151024Document6 pages2264-Article Text-5024-4-10-20151024shivamNo ratings yet
- JAMP - Mohamed Ali Edit.Document6 pagesJAMP - Mohamed Ali Edit.Iniya RajendranNo ratings yet
- 1 s2.0 S2468824X17300517 MainDocument5 pages1 s2.0 S2468824X17300517 MainFirah Triple'sNo ratings yet
- High Dose Dexamethasone in Low Pain Responders UndDocument9 pagesHigh Dose Dexamethasone in Low Pain Responders UndBhavani VuppuNo ratings yet
- Use of Dexmedetomidine As A Sedative and Analgesic Agent in Critically Ill Adult Patients: A Meta-AnalysisDocument14 pagesUse of Dexmedetomidine As A Sedative and Analgesic Agent in Critically Ill Adult Patients: A Meta-AnalysisPatty Alarcón ParraNo ratings yet
- Ó Canadian Anesthesiologists' Society 2009Document7 pagesÓ Canadian Anesthesiologists' Society 2009MOHAMMED IQBALNo ratings yet
- Ketamina y Dexmedetomidina en QuemadosDocument6 pagesKetamina y Dexmedetomidina en QuemadosVicky CascorNo ratings yet
- Dolor Postop, Ligamentos Cruzados, AmbulatorioDocument7 pagesDolor Postop, Ligamentos Cruzados, AmbulatorioChurrunchaNo ratings yet
- Journal Homepage: - : Manuscript HistoryDocument50 pagesJournal Homepage: - : Manuscript HistoryIJAR JOURNALNo ratings yet
- Surve Rohini 2016Document7 pagesSurve Rohini 2016Amro MahmoudNo ratings yet
- Comparison Efectiveness of Dexmedetomidine Versus Dexmedetomidine With Ketamine For Tympanoplasty Surgery Done Under Monitoredanaesthesia CareDocument7 pagesComparison Efectiveness of Dexmedetomidine Versus Dexmedetomidine With Ketamine For Tympanoplasty Surgery Done Under Monitoredanaesthesia CareIJAR JOURNALNo ratings yet
- Journal Homepage: - : Manuscript HistoryDocument7 pagesJournal Homepage: - : Manuscript HistoryIJAR JOURNALNo ratings yet
- Efficacy Lidocaine Endoscopic Submucosal DissectionDocument7 pagesEfficacy Lidocaine Endoscopic Submucosal DissectionAnonymous lSWQIQNo ratings yet
- 0 Aet484Document7 pages0 Aet484UsbahNo ratings yet
- Journal Homepage: - : IntroductionDocument6 pagesJournal Homepage: - : IntroductionIJAR JOURNALNo ratings yet
- Role of Dexmedetomidine Infusion After Coronary Artery Bypass GraftingDocument6 pagesRole of Dexmedetomidine Infusion After Coronary Artery Bypass GraftingWidya KusumaNo ratings yet
- Garcia 2021Document9 pagesGarcia 2021Giancarlo Maruri MunarettoNo ratings yet
- Journal Homepage: - : IntroductionDocument5 pagesJournal Homepage: - : IntroductionIJAR JOURNALNo ratings yet
- AnesthEssaysRes11172-7351168 202511Document6 pagesAnesthEssaysRes11172-7351168 202511Tiêgo PiresNo ratings yet
- Effect of Intraoperative Dexmedetomidine On Post-Craniotomy PainDocument9 pagesEffect of Intraoperative Dexmedetomidine On Post-Craniotomy PainIva SantikaNo ratings yet
- KetamineDocument7 pagesKetamineAshiyan IrfanNo ratings yet
- Journal Homepage: - : IntroductionDocument8 pagesJournal Homepage: - : IntroductionIJAR JOURNALNo ratings yet
- Effects of Intravenous Dexmedetomidine On Hyperbaric Bupivacaine Spinal Anesthesia: A Randomized StudyDocument8 pagesEffects of Intravenous Dexmedetomidine On Hyperbaric Bupivacaine Spinal Anesthesia: A Randomized StudyMOHAMMED IQBALNo ratings yet
- Estudio SEDCOMDocument11 pagesEstudio SEDCOMElias Vera RojasNo ratings yet
- Journal Homepage: - : Manuscript HistoryDocument7 pagesJournal Homepage: - : Manuscript HistoryIJAR JOURNALNo ratings yet
- IndianJAnaesth582138-632895 173449Document5 pagesIndianJAnaesth582138-632895 173449xxxvrgntNo ratings yet
- Comparison of Hyperbaric Levobupivacaine/ Bupivacaine For Ceserean SectionDocument6 pagesComparison of Hyperbaric Levobupivacaine/ Bupivacaine For Ceserean SectionIJAR JOURNALNo ratings yet
- Books Binding BodyDocument71 pagesBooks Binding BodyToufique KhanNo ratings yet
- 3959-Article Text-28779-2-10-20210715Document6 pages3959-Article Text-28779-2-10-20210715Mehroze SalmanNo ratings yet
- Jurnal AnestesiDocument7 pagesJurnal AnestesiJessica GraciaNo ratings yet
- Pub 3Document5 pagesPub 3Shreyas KateNo ratings yet
- Ozaki2014 Article SafetyAndEfficacyOfDexmedetomiDocument13 pagesOzaki2014 Article SafetyAndEfficacyOfDexmedetomiidaNo ratings yet
- International Journal of Anesthetics and Anesthesiology Ijaa 7 112Document4 pagesInternational Journal of Anesthetics and Anesthesiology Ijaa 7 112mikoNo ratings yet
- Yurnal 1Document5 pagesYurnal 1Nopriza AidyNo ratings yet
- Dexmedetomidine Vs Clonidine in Bupivacaine Spinal BlockDocument6 pagesDexmedetomidine Vs Clonidine in Bupivacaine Spinal Blockrandomaeiou7273No ratings yet
- 2021 - Dexmed LOSDocument9 pages2021 - Dexmed LOScringlesoreosNo ratings yet
- IJPCR, Vol 15, Issue 9, Article 245Document5 pagesIJPCR, Vol 15, Issue 9, Article 245Jaldeep PatelNo ratings yet
- My Thesis Protocol-4Document15 pagesMy Thesis Protocol-4Rio RockyNo ratings yet
- Journal Homepage: - : IntroductionDocument4 pagesJournal Homepage: - : IntroductionIJAR JOURNALNo ratings yet
- AN4 OA Sidharth-2Document6 pagesAN4 OA Sidharth-2Dede TarunaNo ratings yet
- Non Analgesic BenefitDocument11 pagesNon Analgesic Benefitajay kumarNo ratings yet
- Riker2009 Dexmedetomidine Vs Midazolam For Sedation of Critically Ill Patients, A Randomized TrialDocument11 pagesRiker2009 Dexmedetomidine Vs Midazolam For Sedation of Critically Ill Patients, A Randomized TrialjosefmagnoNo ratings yet
- A Comparative Study of Caudal Block Usinglignocaine Alone and With Ketamine For Adultanorectal SurgeriesDocument8 pagesA Comparative Study of Caudal Block Usinglignocaine Alone and With Ketamine For Adultanorectal SurgeriesIJAR JOURNALNo ratings yet
- The Effect of Intravenously Administered Dexmedetomidine On Haemodynamic Response To Intubation in Patients Undergoing Surgery Under General AnaesthesiaDocument3 pagesThe Effect of Intravenously Administered Dexmedetomidine On Haemodynamic Response To Intubation in Patients Undergoing Surgery Under General AnaesthesiaInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- Effect of Dexamethasone As An Adjuvant To Bupivacaine in Ultrasound Guided Interscalene Brachial Plexus Block in Upper Arm SurgeriesDocument16 pagesEffect of Dexamethasone As An Adjuvant To Bupivacaine in Ultrasound Guided Interscalene Brachial Plexus Block in Upper Arm SurgeriesIJAR JOURNALNo ratings yet
- Clinical Evaluation of A Microablativefractional Carbon Dioxide 2010Document1 pageClinical Evaluation of A Microablativefractional Carbon Dioxide 2010Аркадий ЖивицаNo ratings yet
- A Comparison of The Analgesic Effi Cacy of Transforaminal Methylprednisolone Alone and With Low Doses of Clonidine in Lumbo-Sacral RadiculopathyDocument9 pagesA Comparison of The Analgesic Effi Cacy of Transforaminal Methylprednisolone Alone and With Low Doses of Clonidine in Lumbo-Sacral RadiculopathyJumatun Mona WarahNo ratings yet
- Successful Implementation of A Pediatric Sedation Protocol For Mechanically Ventilated PatientsDocument6 pagesSuccessful Implementation of A Pediatric Sedation Protocol For Mechanically Ventilated PatientsSantosa TandiNo ratings yet
- Obstetrics AnesthesiaDocument31 pagesObstetrics AnesthesiaNorfarhanah ZakariaNo ratings yet
- Musa Shirmohammadie, Alireza Ebrahim Soltani, Shahriar Arbabi, Karim NasseriDocument6 pagesMusa Shirmohammadie, Alireza Ebrahim Soltani, Shahriar Arbabi, Karim Nasseridebby claudiNo ratings yet
- Impact of Postoperative Dexmedetomidine Infusion On Incidence of Delirium in Elderly Patients Undergoing Major Elective Noncardiac Surgery2019Document12 pagesImpact of Postoperative Dexmedetomidine Infusion On Incidence of Delirium in Elderly Patients Undergoing Major Elective Noncardiac Surgery2019Cláudia Regina FernandesNo ratings yet
- 2 Article JCDR FinalDocument4 pages2 Article JCDR FinalMythology KingdomNo ratings yet
- Analgesic Efficacy of Ultrasound-Guided Transversus Abdominis Plane Block in Patients Undergoing Laparoscopic AppendicectomyDocument9 pagesAnalgesic Efficacy of Ultrasound-Guided Transversus Abdominis Plane Block in Patients Undergoing Laparoscopic AppendicectomyIJAR JOURNALNo ratings yet
- Thoracic Segmental Spinal Anaesthesia/ General Anaesthesia For Laproscopy SurgeryDocument8 pagesThoracic Segmental Spinal Anaesthesia/ General Anaesthesia For Laproscopy SurgeryIJAR JOURNALNo ratings yet
- Postoperative Nausea and Vomiting in OpioidFree Anesthesia Versus Opioid Based Anesthesia in Laparoscopic CholecystectomyDocument8 pagesPostoperative Nausea and Vomiting in OpioidFree Anesthesia Versus Opioid Based Anesthesia in Laparoscopic Cholecystectomypepe4dwinNo ratings yet
- Cag La Oz Bak Isak Kurt 2009Document7 pagesCag La Oz Bak Isak Kurt 2009Arturo AlcantaraNo ratings yet
- Top Trials in Gastroenterology & HepatologyFrom EverandTop Trials in Gastroenterology & HepatologyRating: 4.5 out of 5 stars4.5/5 (7)
- Scratch Wound Healing Assay: Simona Martinotti and Elia RanzatoDocument5 pagesScratch Wound Healing Assay: Simona Martinotti and Elia RanzatoNeha MasarkarNo ratings yet
- The Hypoxic Tumor Microenvironment in Vivo Selects The Cancer Stem Cell Fate of Breast Cancer CellsDocument15 pagesThe Hypoxic Tumor Microenvironment in Vivo Selects The Cancer Stem Cell Fate of Breast Cancer CellsNeha MasarkarNo ratings yet
- 152496-Article Text-399697-1-10-20170307Document8 pages152496-Article Text-399697-1-10-20170307Neha MasarkarNo ratings yet
- Dyslipidemia and Cardiovascular Changes in Children: ReviewDocument6 pagesDyslipidemia and Cardiovascular Changes in Children: ReviewNeha MasarkarNo ratings yet
- Cholesterol, Triglycerides, and Associated Lipoproteins - Clinical Methods - NCBI BookshelfDocument30 pagesCholesterol, Triglycerides, and Associated Lipoproteins - Clinical Methods - NCBI BookshelfNeha MasarkarNo ratings yet
- Template Laporan DEDDocument2 pagesTemplate Laporan DEDaminNo ratings yet
- L7CN :connecting LANs, Backbone Networks, and Virtual LANsDocument12 pagesL7CN :connecting LANs, Backbone Networks, and Virtual LANsAhmad Shdifat100% (1)
- Dynamic ProgrammingDocument5 pagesDynamic ProgrammingKrafton GamingNo ratings yet
- Deviser TV Analyser S7000: Multi Norm גוסמ היזיוולט תוא חתנDocument11 pagesDeviser TV Analyser S7000: Multi Norm גוסמ היזיוולט תוא חתנtelesatellitehebrewNo ratings yet
- Earth and Life Science Mock TestDocument7 pagesEarth and Life Science Mock TestFederico Bautista Vacal Jr.No ratings yet
- FUNDAMENTALS OF COMPUTER AssignmentDocument9 pagesFUNDAMENTALS OF COMPUTER AssignmentUrooj KhanNo ratings yet
- Cold Rolled Steel StripDocument40 pagesCold Rolled Steel StripshelarsanjayNo ratings yet
- Lycopodiella Cernua (L.)Document11 pagesLycopodiella Cernua (L.)Nguyen BinhNo ratings yet
- Chapter - 44Document5 pagesChapter - 44tito cuadrosNo ratings yet
- Santiago City, Philippines: University of La Salette Inc College of Engineering and ArchitectureDocument11 pagesSantiago City, Philippines: University of La Salette Inc College of Engineering and ArchitectureDonalyn RnqlloNo ratings yet
- Web Server Log Analysis SysytemDocument3 pagesWeb Server Log Analysis SysytemNexgen TechnologyNo ratings yet
- 2013 Robust Pixel-Based Classification of Obstacles For Robotic Harvesting of Sweet-Pepper PDFDocument15 pages2013 Robust Pixel-Based Classification of Obstacles For Robotic Harvesting of Sweet-Pepper PDFSaNo ratings yet
- Automotive Sumative TestDocument5 pagesAutomotive Sumative TestRAndy rodelas100% (2)
- Communion With The Infinite - The Visual Music of The Shipibo Tribe of The Amazon - AyahuascaDocument6 pagesCommunion With The Infinite - The Visual Music of The Shipibo Tribe of The Amazon - AyahuascaJef BakerNo ratings yet
- Xii - CHEM AKASH - Project - 2023 - 24Document3 pagesXii - CHEM AKASH - Project - 2023 - 24Priyaranjan PattanayakNo ratings yet
- VFP Questions - Test 1Document1 pageVFP Questions - Test 1Rahul JoshiNo ratings yet
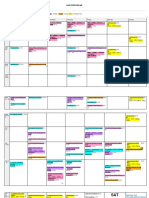
- SAT Study ScheduleDocument3 pagesSAT Study ScheduleDaksh SinghNo ratings yet
- Telephone DirectoryDocument4 pagesTelephone DirectoryDhaniya Karthik33% (3)
- Mental Practice in Chronic StrokeDocument6 pagesMental Practice in Chronic StrokeIsa AbdantauhidNo ratings yet
- V-Wheels (25203-02)Document33 pagesV-Wheels (25203-02)nicopoehlmannNo ratings yet
- Physics 101: Fall 2003 Session - General InformationDocument4 pagesPhysics 101: Fall 2003 Session - General InformationMAnohar KumarNo ratings yet
- Windows ErrosDocument122 pagesWindows ErrosLuiz MoserNo ratings yet
- Inventory Management SystemDocument33 pagesInventory Management SystemSmit Joshi0% (1)
- Wasserdestillierapparate Water Stills 2002 - 2012: Downloaded From Manuals Search EngineDocument19 pagesWasserdestillierapparate Water Stills 2002 - 2012: Downloaded From Manuals Search EngineAnibal PeñaNo ratings yet
- Laboratory Manual Physics of Engineers: Engr. Danielle Joy L. AlcantaraDocument38 pagesLaboratory Manual Physics of Engineers: Engr. Danielle Joy L. AlcantaraSusan LandichoNo ratings yet
- CG Wave Manual 3Document120 pagesCG Wave Manual 3José María Medina Villaverde0% (1)