Download as pdf or txt
You might also like
- 1000 Drug CardsDocument33 pages1000 Drug CardsJelly Bean100% (1)
- Test Bank Medical Terminology A Short Course 6th Edition ChabnerDocument12 pagesTest Bank Medical Terminology A Short Course 6th Edition ChabnerDawn Fischer100% (36)
- NBME 1 BLOCK 1-4 (With Answers)Document206 pagesNBME 1 BLOCK 1-4 (With Answers)Avanca Louis100% (4)
- Nephritic Syndrome - ScienceDirectDocument5 pagesNephritic Syndrome - ScienceDirectraul.villarrealNo ratings yet
- Kev 433Document10 pagesKev 433popescu roxanaNo ratings yet
- The Fi Rst Report Of Myeloma With Igd Κ And Free Κ In IndonesiaDocument5 pagesThe Fi Rst Report Of Myeloma With Igd Κ And Free Κ In Indonesiamuhammad gufronNo ratings yet
- Anti-Glomerular Basement Membrane VasculitisDocument8 pagesAnti-Glomerular Basement Membrane VasculitisDra Daphne Rivero GallegosNo ratings yet
- Renal BiopsiesDocument7 pagesRenal BiopsiesDenise CssNo ratings yet
- Wegener SDocument7 pagesWegener SJeffrey Ian M. KoNo ratings yet
- Diagnostic Algorithms in Renal Biopsy PDFDocument27 pagesDiagnostic Algorithms in Renal Biopsy PDFRajeev Pareek100% (1)
- Oedematous Swelling With Scanty, Dark and at Times Totally Suppressed Urine"Document7 pagesOedematous Swelling With Scanty, Dark and at Times Totally Suppressed Urine"Omar MohammedNo ratings yet
- 1757 1626 1 333Document5 pages1757 1626 1 333Ade CandraNo ratings yet
- Old and New Therapeutic Strategies in Systemic SclerosisDocument6 pagesOld and New Therapeutic Strategies in Systemic SclerosisJosé Javier Morales NúñezNo ratings yet
- Chronic Spontaneous Urticaria-Status Quo and Future: Susanne Melchers Jan P. NicolayDocument11 pagesChronic Spontaneous Urticaria-Status Quo and Future: Susanne Melchers Jan P. NicolayRizka ZulaikhaNo ratings yet
- Crioglobulinemia Glomerular DiseasesDocument13 pagesCrioglobulinemia Glomerular DiseasesBeto RgNo ratings yet
- Kidney Research and Clinical Practice: Jürgen FloegeDocument8 pagesKidney Research and Clinical Practice: Jürgen FloegeAnita PrastiwiNo ratings yet
- Galectin-3 Binding Protein Links Circulating Microparticles With Electron Dense Glomerular Deposits in Lupus NephritisDocument11 pagesGalectin-3 Binding Protein Links Circulating Microparticles With Electron Dense Glomerular Deposits in Lupus NephritisRina kriswiastinyNo ratings yet
- Respiratory and Pulmonary Medicine: ClinmedDocument3 pagesRespiratory and Pulmonary Medicine: ClinmedGrace Yuni Soesanti MhNo ratings yet
- Nejm 2013 Nefropatía IgaDocument13 pagesNejm 2013 Nefropatía Igacesar gonzalezNo ratings yet
- A Diagnostic Dilemma in A Child With Macroscopic Hematuria, Nephrotic Syndrome and Hypocomplementemia: AnswersDocument4 pagesA Diagnostic Dilemma in A Child With Macroscopic Hematuria, Nephrotic Syndrome and Hypocomplementemia: AnswersRiszki_03No ratings yet
- In - Vivo 38 954Document4 pagesIn - Vivo 38 954Tibor SzénásiNo ratings yet
- Mon-023 Hypokalemic Nephropathy in Nephrotic SyndrDocument2 pagesMon-023 Hypokalemic Nephropathy in Nephrotic SyndrJose Fernando OrdosgoitiaNo ratings yet
- Molecular Pathobiology of Scleritis and Its Therapeutic ImplicationsDocument13 pagesMolecular Pathobiology of Scleritis and Its Therapeutic ImplicationsApriansyah Arfandy AzisNo ratings yet
- Diagnostic Challenge of Tuberculosis in Systemic Lupus ErythematosusDocument9 pagesDiagnostic Challenge of Tuberculosis in Systemic Lupus ErythematosusBelinda Putri agustiaNo ratings yet
- Seminars in Diagnostic Pathology: Jared R. Hassler TDocument5 pagesSeminars in Diagnostic Pathology: Jared R. Hassler TYamil FernandezNo ratings yet
- Neuromyelitisoptica: Sarah L. Patterson,, Sarah E. GoglinDocument13 pagesNeuromyelitisoptica: Sarah L. Patterson,, Sarah E. GoglinErji K.No ratings yet
- 6137 20449 1 PB PDFDocument6 pages6137 20449 1 PB PDFNaima TariqNo ratings yet
- New Diagnosis Criteria For Common Variable Immunodeficiency Exploration Systematic Review and Current PerspectivesDocument8 pagesNew Diagnosis Criteria For Common Variable Immunodeficiency Exploration Systematic Review and Current PerspectivesInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- Meningoencephalitis of Unknown Origin in Dogs CR - 881Document6 pagesMeningoencephalitis of Unknown Origin in Dogs CR - 881Ezequiel Davi Dos SantosNo ratings yet
- Poststreptococcal Glomerulonephritis - UpToDateDocument21 pagesPoststreptococcal Glomerulonephritis - UpToDateHandre Putra100% (1)
- Chapter 25 - Plasma Cell DisordersDocument47 pagesChapter 25 - Plasma Cell DisordersSantiago ForeroNo ratings yet
- Gfad 090Document42 pagesGfad 090Maria Eduarda CardosoNo ratings yet
- Tuberculous Meningitis - A Case ReportDocument4 pagesTuberculous Meningitis - A Case ReportyayaNo ratings yet
- 13 CR Lethal MidlineDocument3 pages13 CR Lethal MidlineSudhir BayyaNo ratings yet
- Ecthyma Gangrenosum - StatPearls - NCBI BookshelfDocument5 pagesEcthyma Gangrenosum - StatPearls - NCBI BookshelfSyafira Laila NurulitaNo ratings yet
- Optic Neuritis in The Era of BiomarkersDocument6 pagesOptic Neuritis in The Era of BiomarkersMargaretha SweetyNo ratings yet
- Advanced Glycation Endproducts in Peripheral Nerve in Type 2 Diabetes With NeuropathyDocument10 pagesAdvanced Glycation Endproducts in Peripheral Nerve in Type 2 Diabetes With NeuropathyGABYZTNo ratings yet
- Ocular Myasthenia Gravis: A Review Review Article: Epidemiology and DemographicsDocument8 pagesOcular Myasthenia Gravis: A Review Review Article: Epidemiology and DemographicsMunteanu AlexandruNo ratings yet
- International Journal of Pathology and Clinical Research Ijpcr 8 125Document5 pagesInternational Journal of Pathology and Clinical Research Ijpcr 8 125Shila SahaNo ratings yet
- Systemic SclerodermaDocument10 pagesSystemic SclerodermaFafy AitNo ratings yet
- Acute Myeloid LeukemiaDocument33 pagesAcute Myeloid LeukemiardLuis1No ratings yet
- Immunity Inflam Disease - 2022 - LianDocument11 pagesImmunity Inflam Disease - 2022 - LianNguyễn Nhựt MinhNo ratings yet
- MEningitis TBDocument4 pagesMEningitis TBAlexander TegarNo ratings yet
- Understanding The Radiologist's Role in Evaluating Multiple Sclerosis - A Review of The Tip of The IcebergDocument30 pagesUnderstanding The Radiologist's Role in Evaluating Multiple Sclerosis - A Review of The Tip of The IcebergAnkita ShahNo ratings yet
- Art:10.1007/s00595 009 4134 2Document6 pagesArt:10.1007/s00595 009 4134 2Helen SobczykNo ratings yet
- glomerular-diseasesDocument74 pagesglomerular-diseasesdtettamantiNo ratings yet
- Jurding Tia Tamara Stase SyarafDocument8 pagesJurding Tia Tamara Stase Syaraftia tamaraNo ratings yet
- J of Clinical Apheresis - 2023 - Salazar - Therapeutic Plasma Exchange in Refractory Susac S Syndrome A Brief ReportDocument3 pagesJ of Clinical Apheresis - 2023 - Salazar - Therapeutic Plasma Exchange in Refractory Susac S Syndrome A Brief Reportrdsalazar22No ratings yet
- Glomerulonefritis ComplementoDocument10 pagesGlomerulonefritis ComplementoPaola ZuluagaNo ratings yet
- Seminario 2 Inmunologia Clinica 2023-IIDocument9 pagesSeminario 2 Inmunologia Clinica 2023-IImiguel angel ascoy saucedoNo ratings yet
- Editorial Immune Dysfunction in Nephrotic Syndrome - Recent Advances and New Roads AheadDocument5 pagesEditorial Immune Dysfunction in Nephrotic Syndrome - Recent Advances and New Roads AheadBeatri AyuzaNo ratings yet
- 03-Md-Vol 3 No2 ZaprianovaDocument3 pages03-Md-Vol 3 No2 ZaprianovaSibinoskiNo ratings yet
- Jurnal PasteurisasiDocument29 pagesJurnal PasteurisasiEzza noerNo ratings yet
- Sjogren ReviewDocument11 pagesSjogren ReviewMariano AlbertalNo ratings yet
- Review Article Ocular Myasthenia Gravis: A Review: Epidemiology and DemographicsDocument7 pagesReview Article Ocular Myasthenia Gravis: A Review: Epidemiology and DemographicsMaxend Arselino SilooyNo ratings yet
- Cronion2018 Vírus e SíndromeDocument1 pageCronion2018 Vírus e Síndromebeatriceandrade97No ratings yet
- CE Update: Wegener's Granulomatosis: A Review of The Clinical Implications, Diagnosis, and TreatmentDocument3 pagesCE Update: Wegener's Granulomatosis: A Review of The Clinical Implications, Diagnosis, and TreatmentAfif FaiziNo ratings yet
- Case Report: Non Secretory Multiple MyelomaDocument4 pagesCase Report: Non Secretory Multiple MyelomaJeremy HalimNo ratings yet
- Case Report: Wouter Meersseman, Patrick Verschueren, Thomas Tousseyn, Rita de Vos, David CassimanDocument1 pageCase Report: Wouter Meersseman, Patrick Verschueren, Thomas Tousseyn, Rita de Vos, David Cassimanmafe alvarezNo ratings yet
- 10.1515 - Almed 2021 0087Document6 pages10.1515 - Almed 2021 0087Miguel Ángel Martínez MartínNo ratings yet
- Caso Clínico InmunologiaDocument4 pagesCaso Clínico InmunologiaAna EmiliaNo ratings yet
- Lucas 2014Document8 pagesLucas 2014Prima YosiNo ratings yet
- Neuroimmunology: Multiple Sclerosis, Autoimmune Neurology and Related DiseasesFrom EverandNeuroimmunology: Multiple Sclerosis, Autoimmune Neurology and Related DiseasesAmanda L. PiquetNo ratings yet
- Wjarr 2023 1265Document7 pagesWjarr 2023 1265Delavemia RNo ratings yet
- EJ1286551Document9 pagesEJ1286551Delavemia RNo ratings yet
- Journal of Children's Literature: January 2009Document12 pagesJournal of Children's Literature: January 2009Delavemia RNo ratings yet
- Cover PBL 4Document1 pageCover PBL 4Delavemia RNo ratings yet
- Prickly Heat and Heat Rash (Miliaria)Document3 pagesPrickly Heat and Heat Rash (Miliaria)Delavemia RNo ratings yet
- Effects of Short-And Long-Term REM Sleep Deprivation On Sexual Behavior in Male RatsDocument5 pagesEffects of Short-And Long-Term REM Sleep Deprivation On Sexual Behavior in Male RatsDelavemia RNo ratings yet
- Developmental Human Leydig CellDocument9 pagesDevelopmental Human Leydig CellDelavemia RNo ratings yet
- Craft Card: Cake Greeting Card Set A: Part A Part B Part CDocument9 pagesCraft Card: Cake Greeting Card Set A: Part A Part B Part CDelavemia RNo ratings yet
- Contact Dermatitis - 2006Document38 pagesContact Dermatitis - 2006Delavemia RNo ratings yet
- Mca 25 510Document6 pagesMca 25 510Delavemia RNo ratings yet
- The Pathogenesis of Coronavirus Disease 2019 (COVID-19) - Evaluation and PreventionDocument8 pagesThe Pathogenesis of Coronavirus Disease 2019 (COVID-19) - Evaluation and PreventionRizki Ananda AladinNo ratings yet
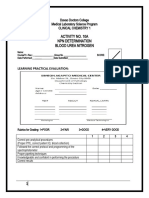
- CC1 Lab Manual FinalDocument14 pagesCC1 Lab Manual FinalMelody PardilloNo ratings yet
- Group 8Document14 pagesGroup 8HrishavNo ratings yet
- Pre AnestesiDocument64 pagesPre AnestesiKevin YonathanNo ratings yet
- Hematology 1 Format For Liyang Conference 2023 Reflection PaperDocument6 pagesHematology 1 Format For Liyang Conference 2023 Reflection PaperJean Calubag CatalanNo ratings yet
- Vaastu in 21 Days Eng by Vastu Maha Utsav PDFDocument75 pagesVaastu in 21 Days Eng by Vastu Maha Utsav PDFM.S. HiremathNo ratings yet
- Susan Sontag AIDS and Its Metaphors 1989 PDFDocument46 pagesSusan Sontag AIDS and Its Metaphors 1989 PDFFernanda Carvalho100% (1)
- Summary of Renal Disorders - 9.11.19Document4 pagesSummary of Renal Disorders - 9.11.19Nicole Juliette CCNo ratings yet
- Cardiovascular Hypertensive Crisis Recent EvidenceDocument6 pagesCardiovascular Hypertensive Crisis Recent Evidenceagustinaw1981No ratings yet
- Osmosis Esophageal Disease PDF Amm DR NotesDocument13 pagesOsmosis Esophageal Disease PDF Amm DR NotestajammalNo ratings yet
- Aminoglycosides: Dr. Amit ShahDocument29 pagesAminoglycosides: Dr. Amit ShahAmit ShahNo ratings yet
- Daftar PustakaDocument4 pagesDaftar Pustakamramadhan_702536No ratings yet
- Diabetes (6. Metas Glucémicas - Estándares de Atención Médica en Diabetes-2022)Document14 pagesDiabetes (6. Metas Glucémicas - Estándares de Atención Médica en Diabetes-2022)Antony Yamid Bolaños VillarrealNo ratings yet
- Finding The Main Idea: Where Are Main Ideas Found?Document85 pagesFinding The Main Idea: Where Are Main Ideas Found?Jemuel CastilloNo ratings yet
- Chd. AmiDocument4 pagesChd. AmiDead shotNo ratings yet
- What Is in ParacetamolDocument5 pagesWhat Is in Paracetamolloremhel barrogaNo ratings yet
- Eyehance MTFDocument6 pagesEyehance MTFanandprasad244No ratings yet
- Reference Ranges Thyroid 6 en 1145213Document52 pagesReference Ranges Thyroid 6 en 1145213SaraZivkovicNo ratings yet
- Summary of Intestinal and Luminal ProtozoaDocument3 pagesSummary of Intestinal and Luminal ProtozoaMegh Raj BhattNo ratings yet
- Correlation Between C - Reactive Protein and Lipid Abnormalities in Subjects With Ischemic StrokeDocument2 pagesCorrelation Between C - Reactive Protein and Lipid Abnormalities in Subjects With Ischemic StrokeIJAR JOURNALNo ratings yet
- Impact of COVID 19 On Psychology of Nurses Working in The EmergencyDocument19 pagesImpact of COVID 19 On Psychology of Nurses Working in The EmergencyEden LacsonNo ratings yet
- HBs Ag Q2Document8 pagesHBs Ag Q2Naveen Kumar MNo ratings yet
- Genacol Instant: The Most Complete Reference Booklet About CollagenDocument28 pagesGenacol Instant: The Most Complete Reference Booklet About CollagendiosesatomicsNo ratings yet
- Anatomical Variations in The Human Paranasal Sinus Region Studied by CTDocument7 pagesAnatomical Variations in The Human Paranasal Sinus Region Studied by CTkhanhlinhNo ratings yet
- WHO Global Pandemic Phases and The Stages For Federal Government ResponseDocument4 pagesWHO Global Pandemic Phases and The Stages For Federal Government ResponseMara Luisa PanopioNo ratings yet
- Thesis On Functional Endoscopic Sinus SurgeryDocument5 pagesThesis On Functional Endoscopic Sinus SurgeryBuyAPaperTulsa100% (2)
- Iron Deficiency Anemia: DiagnosisDocument59 pagesIron Deficiency Anemia: DiagnosisKarlyn Fraiza LahoyNo ratings yet