Download as pdf or txt
You might also like
- Doors Closed Doors OpenDocument3 pagesDoors Closed Doors OpenElleNo ratings yet
- 0 - 16 03 24 Provincial PEWS Nursing Power Point MarchDocument30 pages0 - 16 03 24 Provincial PEWS Nursing Power Point MarchfannyNo ratings yet
- Pre/Post-Assessment Answers: Food Safety in SchoolsDocument6 pagesPre/Post-Assessment Answers: Food Safety in SchoolsFlankzyNo ratings yet
- Multiple Pregnancy LectureDocument33 pagesMultiple Pregnancy Lecturefarid_nchep100% (1)
- Infectious Disease I - 14 (1) - Severe Sepsis and Septic Shock (Courses in Therapeutics and Disease State Management)Document35 pagesInfectious Disease I - 14 (1) - Severe Sepsis and Septic Shock (Courses in Therapeutics and Disease State Management)Ali AlyahawiNo ratings yet
- Prof Djoko - SepsisDocument31 pagesProf Djoko - SepsisfaradillasuciNo ratings yet
- Sjams 34a1645 1648 PDFDocument5 pagesSjams 34a1645 1648 PDFkukyNo ratings yet
- Antivenom Reactions IntroductionDocument14 pagesAntivenom Reactions IntroductionppgpcsNo ratings yet
- COPD Guideline Ver 1.8Document9 pagesCOPD Guideline Ver 1.8Dina AyupnNo ratings yet
- Health Checkup CampDocument24 pagesHealth Checkup CampPravin NamokarNo ratings yet
- Early Warning Scoring System (Unit 9) - 1Document6 pagesEarly Warning Scoring System (Unit 9) - 1Zharlene PadillaNo ratings yet
- KDIGO Clinical Practice Guideline For Acute Kidney Injury.Document18 pagesKDIGO Clinical Practice Guideline For Acute Kidney Injury.Madalina TalpauNo ratings yet
- JCI Accreditation Presentation 3Document77 pagesJCI Accreditation Presentation 3Osama MarzoukNo ratings yet
- Aminoglycoside Dosage Adjustment - Group 4Document27 pagesAminoglycoside Dosage Adjustment - Group 4katrinNo ratings yet
- Parkinsons - Management PlanDocument3 pagesParkinsons - Management Planapi-19753815No ratings yet
- Anticoag Reversal GuidelineDocument24 pagesAnticoag Reversal GuidelineIwanNo ratings yet
- NABH FAQ'sDocument16 pagesNABH FAQ'sarun8591100% (1)
- Palliative and End of Life Care Guidelines 2021Document36 pagesPalliative and End of Life Care Guidelines 2021IKA SYAMSUL HUDA MZNo ratings yet
- Binu Babu 52702942023 01 29 08 32 35 977 1 6 114 133194762170938998 PDFDocument2 pagesBinu Babu 52702942023 01 29 08 32 35 977 1 6 114 133194762170938998 PDFSagar SavantNo ratings yet
- HF HHC-risk-assessment-template BP 19jul21Document4 pagesHF HHC-risk-assessment-template BP 19jul21shazia kaziNo ratings yet
- Sequential (Sepsis-Related) Organ Failure Assessment ScoreDocument1 pageSequential (Sepsis-Related) Organ Failure Assessment ScoreElfira SutantoNo ratings yet
- The DIC Score Is of Prognostic Value in COVID-19 PneumoniaDocument2 pagesThe DIC Score Is of Prognostic Value in COVID-19 PneumoniaaninditaNo ratings yet
- Lembar Jawaban Skill Lab Evidence Based Medicine (Ebm) Nama: Muhammad Fadill Akbar NIM: 04011281621080Document20 pagesLembar Jawaban Skill Lab Evidence Based Medicine (Ebm) Nama: Muhammad Fadill Akbar NIM: 04011281621080Ya'kubNo ratings yet
- COVID-19 Protocol For Non-Invasive Ventilation Using The GO2Vent®Document4 pagesCOVID-19 Protocol For Non-Invasive Ventilation Using The GO2Vent®Diego VenegasNo ratings yet
- DLMP Critical ValueDocument3 pagesDLMP Critical ValueekasyamputraNo ratings yet
- 2019 LAMA For COPDDocument25 pages2019 LAMA For COPDdonnyNo ratings yet
- Interpretation: A06 - Raj Hospital - Cash (Cghs - 20) Main Road Ranchi Jharkhand 834001Document4 pagesInterpretation: A06 - Raj Hospital - Cash (Cghs - 20) Main Road Ranchi Jharkhand 834001AlokNo ratings yet
- Aspr Tracie Sofa Score Fact Sheet PDFDocument3 pagesAspr Tracie Sofa Score Fact Sheet PDFTieti IsaniniNo ratings yet
- Pharmacokinetic of Simvastatin Study in Malaysian SubjectsDocument6 pagesPharmacokinetic of Simvastatin Study in Malaysian SubjectsNur Ilham SaputraNo ratings yet
- Recent Updates To Clinical Practice Guidelines For Diabetes MellituDocument12 pagesRecent Updates To Clinical Practice Guidelines For Diabetes Mellitujimmy HerreraNo ratings yet
- L2 Hypertension in Special GroupsDocument44 pagesL2 Hypertension in Special GroupsMustaquim YusopNo ratings yet
- Eras Bps Sept16Document28 pagesEras Bps Sept16Muhaimin EfendiNo ratings yet
- Weaning ProtocolDocument6 pagesWeaning ProtocolerwanNo ratings yet
- Dyslipidaemia GuidelinesDocument28 pagesDyslipidaemia GuidelinesEllieNo ratings yet
- Lab D0688604 2411031085Document7 pagesLab D0688604 2411031085Antonio Carlos VargasNo ratings yet
- Antibiotik For Renal FailureDocument6 pagesAntibiotik For Renal FailureWidhy Joss BangetzNo ratings yet
- Dr. Sudarto Sppd's FileDocument22 pagesDr. Sudarto Sppd's FileVindy CesarianaNo ratings yet
- Calupad, Rolando Camama 1922061664Document3 pagesCalupad, Rolando Camama 1922061664Chanel RamosNo ratings yet
- Bilas, Remedios Maloloy-On 2485027317Document5 pagesBilas, Remedios Maloloy-On 2485027317mjdigitalprint18No ratings yet
- A4 GentamicinUsageGuide V12 A-1Document12 pagesA4 GentamicinUsageGuide V12 A-1vasquezdario29No ratings yet
- Adriano, Ma. Niña Inocencio 2123035954Document2 pagesAdriano, Ma. Niña Inocencio 2123035954Nina NinzNo ratings yet
- Psych Stat 4Document3 pagesPsych Stat 4Jerald GayloaNo ratings yet
- How To Perform and Interpret An Exercise TestDocument48 pagesHow To Perform and Interpret An Exercise TestBilal AfridiNo ratings yet
- HTA Guide ISH What is New 2021Document6 pagesHTA Guide ISH What is New 2021Osvaldo VillarNo ratings yet
- DOAC VTE Treatment April2020Document4 pagesDOAC VTE Treatment April2020Ahmed MohammedNo ratings yet
- Digoxin Dosing: o o o o oDocument4 pagesDigoxin Dosing: o o o o oLindaNo ratings yet
- WIMJ2017 Vol 4, Issue 1 Complete PDFDocument76 pagesWIMJ2017 Vol 4, Issue 1 Complete PDFarvind YadavNo ratings yet
- Department of Clinical Biochemistry: Investigation Name Result Bio. Ref. Range MethodDocument8 pagesDepartment of Clinical Biochemistry: Investigation Name Result Bio. Ref. Range MethodarupNo ratings yet
- PGDT Protocol Summary ReferenceDocument32 pagesPGDT Protocol Summary Referenceghg sddNo ratings yet
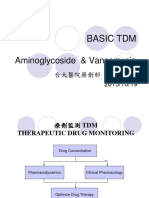
- Aminoglycoside & Vancomycin: Basic TDMDocument57 pagesAminoglycoside & Vancomycin: Basic TDMft84nzzc92No ratings yet
- 2020 ESC Guidelines For The Diagnosis and Management of Atrial FibrillationDocument22 pages2020 ESC Guidelines For The Diagnosis and Management of Atrial FibrillationFerry KrisnamurtiNo ratings yet
- CPG Dyslipidemia 2017 PPT SummaryDocument25 pagesCPG Dyslipidemia 2017 PPT SummaryhakimahsNo ratings yet
- Role of PRP in Diabetic Foot UlcerDocument4 pagesRole of PRP in Diabetic Foot UlcerIJAR JOURNALNo ratings yet
- Pulmonary Rehab - ECarroll PDFDocument26 pagesPulmonary Rehab - ECarroll PDFSulabh ShresthaNo ratings yet
- Evaluasi Nilai KritisDocument10 pagesEvaluasi Nilai KritisLaboratorium RSUD KEMAYORANNo ratings yet
- DKA Adults Management Protocol - DR Anwar Ul HaqDocument3 pagesDKA Adults Management Protocol - DR Anwar Ul HaqAnwar ul HaqNo ratings yet
- Journal Homepage: - : IntroductionDocument5 pagesJournal Homepage: - : IntroductionIJAR JOURNALNo ratings yet
- HDL PresipitantDocument2 pagesHDL PresipitantDidik PrasetyaNo ratings yet
- 2022 Lipids Gui PG ENDocument28 pages2022 Lipids Gui PG ENHerrera MiguelNo ratings yet
- Estrada, Susievill Villareal 1720031402Document2 pagesEstrada, Susievill Villareal 1720031402Susievill EstradaNo ratings yet
- Case Study On Pemphigus Vulgaris (PharmD)Document18 pagesCase Study On Pemphigus Vulgaris (PharmD)kezia15rebeccaNo ratings yet
- Name Ref. by Test Asked: Ankit Gupta (30Y/M) : Self: Hemogram - 6 Part (Diff) Sample Collected atDocument3 pagesName Ref. by Test Asked: Ankit Gupta (30Y/M) : Self: Hemogram - 6 Part (Diff) Sample Collected atDenise CssNo ratings yet
- Obstetric Job List - 2Document2 pagesObstetric Job List - 2ElleNo ratings yet
- Approach To Renal Failure-2Document25 pagesApproach To Renal Failure-2ElleNo ratings yet
- Antipsychotics Risks and BenefitsDocument38 pagesAntipsychotics Risks and BenefitsElleNo ratings yet
- Dhul Hijjah PlannerDocument15 pagesDhul Hijjah PlannerElleNo ratings yet
- Backflip Exercisemanual PDFDocument4 pagesBackflip Exercisemanual PDFArun KarthikNo ratings yet
- Science and Technology Grade 7 ContentDocument1 pageScience and Technology Grade 7 ContentNorjana Otto Medal-Madale67% (3)
- CELL OxigenoDocument1 pageCELL OxigenopedrogutizNo ratings yet
- 7 Day Ruqyah Detox Programme - Shaykh 'Adil Ibn Tahir Al-Muqbil - FacebookDocument2 pages7 Day Ruqyah Detox Programme - Shaykh 'Adil Ibn Tahir Al-Muqbil - FacebookR.RNo ratings yet
- Week 7 ActivityDocument3 pagesWeek 7 ActivityARVIN CRUZNo ratings yet
- Organizational Development & Change Of: Presented By: Kamal Lochan BeheraDocument17 pagesOrganizational Development & Change Of: Presented By: Kamal Lochan BeheraKamalLochanBehera0% (1)
- Volume 22 Issue 4 Mediccine SocietyDocument6 pagesVolume 22 Issue 4 Mediccine SocietyRjRajoraNo ratings yet
- Atmospheric Water GeneratorDocument10 pagesAtmospheric Water GeneratorAbu Anas ShuvomNo ratings yet
- Padampur ReportDocument16 pagesPadampur ReportSaudagar BiswalNo ratings yet
- Diagnostics: Speed Bumps Ahead Prefer Hospitals Over DiagnosticsDocument33 pagesDiagnostics: Speed Bumps Ahead Prefer Hospitals Over DiagnosticsD BasavarajaNo ratings yet
- CAD - Model of DiscDocument5 pagesCAD - Model of DiscAshokkumar VelloreNo ratings yet
- ĐỀ SỐ 33 - DEDocument4 pagesĐỀ SỐ 33 - DE27. Minh PhươngNo ratings yet
- Castrol Activ Scooter 10W-40 4-ATDocument2 pagesCastrol Activ Scooter 10W-40 4-ATDitha KiranaNo ratings yet
- House BhavasDocument3 pagesHouse BhavasBiswajit BeheraNo ratings yet
- Autism at Home BookletDocument32 pagesAutism at Home BookletmonicamarquesNo ratings yet
- Switches and Controls: CatalogDocument257 pagesSwitches and Controls: CatalogRob BrabantNo ratings yet
- Pharmacogenetics Lecture NotesDocument5 pagesPharmacogenetics Lecture NotesMark Russel Sean LealNo ratings yet
- 2022 Audit Form 2B - PCMsDocument7 pages2022 Audit Form 2B - PCMsJAMIL ASUMNo ratings yet
- FDSS CARES Meals Assistance Gift Card Application FormDocument1 pageFDSS CARES Meals Assistance Gift Card Application FormFauquier NowNo ratings yet
- Ap Stat 1-7 NotesDocument12 pagesAp Stat 1-7 NotesCooper BarthNo ratings yet
- Read Online Textbook Applications in Design and Simulation of Sustainable Chemical Processes 1St Edition Dimian A Ebook All Chapter PDFDocument22 pagesRead Online Textbook Applications in Design and Simulation of Sustainable Chemical Processes 1St Edition Dimian A Ebook All Chapter PDFandrew.kraemer929100% (4)
- Falsafah Betty NeumanDocument23 pagesFalsafah Betty NeumanmaheswariNo ratings yet
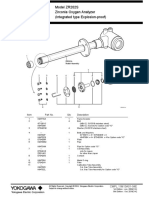
- Documents - Module&file MC1000 - MC1001 Air - EnglishDocument19 pagesDocuments - Module&file MC1000 - MC1001 Air - EnglishEmma ScullyNo ratings yet
- đề 6Document20 pagesđề 6Lê ĐạtNo ratings yet
- Solar DryingDocument15 pagesSolar DryinggetsweetNo ratings yet
- 10 Types of Plants AlbumDocument11 pages10 Types of Plants AlbumMateo GarciaNo ratings yet
- Structure of Human Eye DipiyDocument10 pagesStructure of Human Eye Dipiyvineet_knwrNo ratings yet
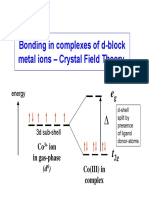
- ABC mg7 (1) - Bonding in Complexes - CrystalfieldtheoryDocument50 pagesABC mg7 (1) - Bonding in Complexes - CrystalfieldtheoryAdistaNo ratings yet