Download as pdf or txt
You might also like
- 8 - Maxillary Expansion in Nongrowing Patients. Conventional, SurgicalDocument11 pages8 - Maxillary Expansion in Nongrowing Patients. Conventional, SurgicalMariana SantosNo ratings yet
- MTS Vocab 2023Document9 pagesMTS Vocab 2023Rahul Chauhan100% (1)
- VanGogh EbookDocument288 pagesVanGogh EbookDragan Cvetkovic88% (8)
- Rapid Maxillary Expansion. Is It Better in The Mixed or in The Permanent Dentition?Document8 pagesRapid Maxillary Expansion. Is It Better in The Mixed or in The Permanent Dentition?Gustavo AnteparraNo ratings yet
- Z.leaf ExpanderDocument20 pagesZ.leaf ExpanderLima JúniorNo ratings yet
- i1945-7103-92-5-579Document10 pagesi1945-7103-92-5-579RANIK DUTTANo ratings yet
- 017Document9 pages017Lima JúniorNo ratings yet
- Dental Arch Changes Comparison Between Expander With Differential Opening and Fan-Type Expander: A Randomized Controlled TrialDocument9 pagesDental Arch Changes Comparison Between Expander With Differential Opening and Fan-Type Expander: A Randomized Controlled TrialErika NuñezNo ratings yet
- Fixed Versus Removable Orthodontic Appliances To Correct Anterior Crossbite in The Mixed Dentition-A Randomized Controlled Trial PDFDocument6 pagesFixed Versus Removable Orthodontic Appliances To Correct Anterior Crossbite in The Mixed Dentition-A Randomized Controlled Trial PDFJejeNo ratings yet
- A Comparison of Treatment Results of Adult Deep-Bite Cases Treated With Lingual and Labial Fixed AppliancesDocument7 pagesA Comparison of Treatment Results of Adult Deep-Bite Cases Treated With Lingual and Labial Fixed AppliancesScribd AccountNo ratings yet
- Sri Dwi Mutiara - Jurnal Maloklusi 1Document8 pagesSri Dwi Mutiara - Jurnal Maloklusi 1sri dwi mutiaraNo ratings yet
- 1 s2.0 S2212443823000371 MainDocument11 pages1 s2.0 S2212443823000371 MainMirza GlusacNo ratings yet
- Cju 005Document5 pagesCju 005gifar ihsanNo ratings yet
- Comparison of Changes in SkeletalDocument9 pagesComparison of Changes in SkeletalMariana SantosNo ratings yet
- Cambios 2Document10 pagesCambios 2Miguel candelaNo ratings yet
- Annarumma 2021Document13 pagesAnnarumma 2021Dr.Thrivikhraman KothandaramanNo ratings yet
- Treatment Effects After Maxillary Expansion Using Tooth-Borne Vs Tissue-Borne Miniscrew-Assisted Rapid Palatal Expansion ApplianceDocument9 pagesTreatment Effects After Maxillary Expansion Using Tooth-Borne Vs Tissue-Borne Miniscrew-Assisted Rapid Palatal Expansion ApplianceRolando Huaman BravoNo ratings yet
- Angle Orthod. 2022 92 5 589-97Document9 pagesAngle Orthod. 2022 92 5 589-97brookortontiaNo ratings yet
- Artículo OrtopeidiaDocument9 pagesArtículo OrtopeidiaDEICY PATRICIA ORTIZ GUANGANo ratings yet
- Effects of Class II Elastics During Growth On The Functional Occlusal Plane According To Skeletal Pattern and Extraction Vs NonextractionDocument7 pagesEffects of Class II Elastics During Growth On The Functional Occlusal Plane According To Skeletal Pattern and Extraction Vs NonextractionAlejandra NietoNo ratings yet
- Lagravere (2020) retrospectivCBCTDocument9 pagesLagravere (2020) retrospectivCBCTyeny valdivia albornozNo ratings yet
- Evaluation of Orthodontic Treatment After 1 Year of Retention-A Randomized Controlled TrialDocument6 pagesEvaluation of Orthodontic Treatment After 1 Year of Retention-A Randomized Controlled TrialRenan VeigaNo ratings yet
- Current Practice For Transverse Mandibular and Maxillary Discrepancies in The NetherlandsDocument10 pagesCurrent Practice For Transverse Mandibular and Maxillary Discrepancies in The NetherlandsDONGXU LIUNo ratings yet
- Three-Dimensional Evaluation of Forced Unilateral Posterior Crossbite Correction in The Mixed Dentition: A Randomized Controlled TrialDocument11 pagesThree-Dimensional Evaluation of Forced Unilateral Posterior Crossbite Correction in The Mixed Dentition: A Randomized Controlled TrialNICO ARMANDO ORELLANA LUDEÑANo ratings yet
- Stability of Anterior Crossbite CorrectionDocument8 pagesStability of Anterior Crossbite CorrectionannysaNo ratings yet
- 1 s2.0 S2212443814000186 Main 2Document6 pages1 s2.0 S2212443814000186 Main 2Pau ContrerasNo ratings yet
- Miroperforaciones PDFDocument6 pagesMiroperforaciones PDFceci hdeezNo ratings yet
- CrossbowDocument11 pagesCrossbowm.malekiNo ratings yet
- 12903_2021_Article_1628Document4 pages12903_2021_Article_1628Catia PintoNo ratings yet
- Fixed Versus Removable Appliance For Palatal Expansion A 3D Analysis Using The Finite Element MethodDocument11 pagesFixed Versus Removable Appliance For Palatal Expansion A 3D Analysis Using The Finite Element MethodfarahNo ratings yet
- Orthopedic Effects of Splint High-Pull Headgear-A Cephalometric AppraisalDocument10 pagesOrthopedic Effects of Splint High-Pull Headgear-A Cephalometric AppraisalSarath KumarNo ratings yet
- Treatment of Posterior Crossbite Comparing 2 Appliances: A Community-Based TrialDocument8 pagesTreatment of Posterior Crossbite Comparing 2 Appliances: A Community-Based TrialPae Anusorn AmtanonNo ratings yet
- Eross 2015Document9 pagesEross 2015serahNo ratings yet
- Benedict Wimes, Mascara FacialDocument8 pagesBenedict Wimes, Mascara FacialjamilistccNo ratings yet
- Jced 9 E1029Document6 pagesJced 9 E1029Ana Gabriela AlbuquerqueNo ratings yet
- Lip BumperDocument7 pagesLip BumperMiguel JaènNo ratings yet
- DownloadDocument12 pagesDownloadRodrigo PontesNo ratings yet
- 9 - Skeletal and Dentoalveolar Effects of Miniscrew-Assisted Rapid Palatal Expansion Based On The Length of The MiniscrewDocument8 pages9 - Skeletal and Dentoalveolar Effects of Miniscrew-Assisted Rapid Palatal Expansion Based On The Length of The MiniscrewMariana SantosNo ratings yet
- Cone Beam y ExpansionDocument7 pagesCone Beam y ExpansionYorisbeth SanNo ratings yet
- 10 1067@mpr 2000 107113Document7 pages10 1067@mpr 2000 107113gbaez.88No ratings yet
- Ejo 1Document11 pagesEjo 1ayisNo ratings yet
- Occlusal Plane Dictated Skeletal and Dental Malocclusion With Concomitant Postural Diagnostic Findings A Pilot Study Using Functional Positioning OverlaysDocument17 pagesOcclusal Plane Dictated Skeletal and Dental Malocclusion With Concomitant Postural Diagnostic Findings A Pilot Study Using Functional Positioning OverlaysAthenaeum Scientific PublishersNo ratings yet
- 5Document8 pages5ayisNo ratings yet
- Transverse Dentoalveolar Response of Mandibular Arch After Rapid Maxillary Expansion (RME) With Tooth-Borne and Bone-Borne Appliances: A CBCT Retrospective StudyDocument8 pagesTransverse Dentoalveolar Response of Mandibular Arch After Rapid Maxillary Expansion (RME) With Tooth-Borne and Bone-Borne Appliances: A CBCT Retrospective StudyMirza GlusacNo ratings yet
- Early Prevention of Maxillary Canine Impaction: A Randomized Clinical TrialDocument11 pagesEarly Prevention of Maxillary Canine Impaction: A Randomized Clinical TrialrecherchebibliNo ratings yet
- Nonsurgical Miniscrew-Assisted Rapid Maxillary Expansion Results in Acceptable Stability in Young AdultsDocument8 pagesNonsurgical Miniscrew-Assisted Rapid Maxillary Expansion Results in Acceptable Stability in Young AdultsRolando Huaman BravoNo ratings yet
- Orthopedic Outcomes of Hybrid and Conventional Hyrax Expanders Par Daniela Garib Angle Ortho 2021Document9 pagesOrthopedic Outcomes of Hybrid and Conventional Hyrax Expanders Par Daniela Garib Angle Ortho 2021NANA NANA Arnel redonNo ratings yet
- Dentofacial Effects of Two Facemask Therapies For Maxillary Protraction Miniscrew Implants Versus Rapid Maxillary ExpandersDocument9 pagesDentofacial Effects of Two Facemask Therapies For Maxillary Protraction Miniscrew Implants Versus Rapid Maxillary ExpandersMariana SantosNo ratings yet
- IPIntJMedPaediatrOncol 9 2 77 82Document6 pagesIPIntJMedPaediatrOncol 9 2 77 82Laraduta AgustiniNo ratings yet
- Skeletal and Dentoalveolar Changes After Miniscrew-Assisted Rapid Palatal Expansion in Young Adults A Cone-Beam Computed Tomography Study.Document11 pagesSkeletal and Dentoalveolar Changes After Miniscrew-Assisted Rapid Palatal Expansion in Young Adults A Cone-Beam Computed Tomography Study.Natan GussNo ratings yet
- Cjad 024Document13 pagesCjad 024MSHNo ratings yet
- Schropp Et Al (2005) Immediate Vs Delayed IJOMI PDFDocument9 pagesSchropp Et Al (2005) Immediate Vs Delayed IJOMI PDFAlla MushkeyNo ratings yet
- Schropp Et Al (2005) Immediate Vs Delayed IJOMIDocument9 pagesSchropp Et Al (2005) Immediate Vs Delayed IJOMIAlla MushkeyNo ratings yet
- Al-Dumaini - 2018 - A Novel Approach For Treatment of Skeletal Class II Malocclusion - Miniplates-Based Skeletal AnchorageDocument9 pagesAl-Dumaini - 2018 - A Novel Approach For Treatment of Skeletal Class II Malocclusion - Miniplates-Based Skeletal AnchoragefishribbonNo ratings yet
- Journal of Cranio-Maxillo-Facial Surgery: Mohammad Zandi, Amirfarhang Miresmaeili, Ali HeidariDocument6 pagesJournal of Cranio-Maxillo-Facial Surgery: Mohammad Zandi, Amirfarhang Miresmaeili, Ali HeidariYeraldin EspañaNo ratings yet
- 2022 Marpe Vs Paoo BMRI2022-1974467Document7 pages2022 Marpe Vs Paoo BMRI2022-1974467mlnunezNo ratings yet
- Complications in The Use of The Mandibular Body, Ramus and Symphysis As Donor Sites in Bone Graft Surgery. A Systematic ReviewDocument9 pagesComplications in The Use of The Mandibular Body, Ramus and Symphysis As Donor Sites in Bone Graft Surgery. A Systematic ReviewBrenda Carolina Pattigno ForeroNo ratings yet
- Ed Manty Neli Us 2014Document9 pagesEd Manty Neli Us 2014Renan VeigaNo ratings yet
- Skeletal Width Changes After Mini-Implant-Assisted Rapid Maxillary Expansion (MARME) in Young AdultsDocument6 pagesSkeletal Width Changes After Mini-Implant-Assisted Rapid Maxillary Expansion (MARME) in Young AdultsRolando Huaman BravoNo ratings yet
- I0003 3219 87 2 230Document9 pagesI0003 3219 87 2 230salma hasya rahmaniNo ratings yet
- Post treatmentStabilityInOrthoDocument8 pagesPost treatmentStabilityInOrthoSRI RAHMAH GUNAWANNo ratings yet
- Peri-Implant Complications: A Clinical Guide to Diagnosis and TreatmentFrom EverandPeri-Implant Complications: A Clinical Guide to Diagnosis and TreatmentNo ratings yet
- Spontaneous Changes in Mandibular Incisor Crowding From Mixed To Permanent Dentition SRDocument10 pagesSpontaneous Changes in Mandibular Incisor Crowding From Mixed To Permanent Dentition SRtanloonhanNo ratings yet
- Stabilization of Functional Treatment - The Waveney Goal Post ApplianceDocument4 pagesStabilization of Functional Treatment - The Waveney Goal Post AppliancetanloonhanNo ratings yet
- Bms Course & Exam Form 2017-2018Document2 pagesBms Course & Exam Form 2017-2018tanloonhanNo ratings yet
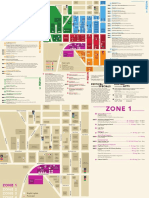
- Singapore Night Festival 2018 E-BrochureDocument7 pagesSingapore Night Festival 2018 E-BrochuretanloonhanNo ratings yet
- Exploring Gunung Gap and Gunung Ulu Semangkok: The TrekDocument25 pagesExploring Gunung Gap and Gunung Ulu Semangkok: The TrektanloonhanNo ratings yet
- Dental Bill 2017Document93 pagesDental Bill 2017tanloonhanNo ratings yet
- Ceph HandoutDocument18 pagesCeph Handoutwaheguru13he13No ratings yet
- Dentistnearby InfoDocument1 pageDentistnearby InfotanloonhanNo ratings yet
- Digital Booklet - All of YouDocument11 pagesDigital Booklet - All of YoutanloonhanNo ratings yet
- Kyon LyricsDocument2 pagesKyon LyricstanloonhanNo ratings yet
- Booklet - Oblivion (Original MotionDocument7 pagesBooklet - Oblivion (Original MotionAmcelo Dade100% (1)
- A New Era of Currency Derivatives Market in India: Dr. E.V.P.A.S.PallaviDocument5 pagesA New Era of Currency Derivatives Market in India: Dr. E.V.P.A.S.PallavirommelNo ratings yet
- Monthly College Expense BudgetDocument4 pagesMonthly College Expense BudgetYaseen Al-QadasiNo ratings yet
- Slugging Load - Riser & Tie-In Spool StressDocument566 pagesSlugging Load - Riser & Tie-In Spool Stressbomxiga100% (3)
- PCS GSM PicoCell Booster Updated R5 PDFDocument3 pagesPCS GSM PicoCell Booster Updated R5 PDFpandavision76No ratings yet
- Chapter I (LPE 409 2021)Document12 pagesChapter I (LPE 409 2021)afia rahmanNo ratings yet
- 7 ChakrasDocument36 pages7 ChakrasmadhulataagiwalNo ratings yet
- Gunner: Class: A Homebrew Class For Use With 5eDocument10 pagesGunner: Class: A Homebrew Class For Use With 5eНикита ТилининNo ratings yet
- Toward A Marxist Thoery of The Labor Process - BurowayDocument67 pagesToward A Marxist Thoery of The Labor Process - BurowayXavi EsviNo ratings yet
- Stirling SC20091029Item18CityParkingDocument26 pagesStirling SC20091029Item18CityParkingparkingeconomicsNo ratings yet
- Jones CaseDocument1 pageJones CaseAlejandra GutierrezNo ratings yet
- How To Write An EssayDocument4 pagesHow To Write An EssayShah BaibrassNo ratings yet
- ArsenalDocument12 pagesArsenaljpkehoe100% (1)
- Chevron Corrective Action OrderDocument8 pagesChevron Corrective Action OrderThe Salt Lake TribuneNo ratings yet
- United States v. Castillo Moronta, 27 F.3d 554, 1st Cir. (1994)Document3 pagesUnited States v. Castillo Moronta, 27 F.3d 554, 1st Cir. (1994)Scribd Government DocsNo ratings yet
- More Than 15,000 Rape Kits Still Sit Untested in North CarolinaDocument52 pagesMore Than 15,000 Rape Kits Still Sit Untested in North CarolinaDevetta BlountNo ratings yet
- Rosselis ColmenaresDocument2 pagesRosselis ColmenaresjosepaticaNo ratings yet
- pmp1000 Pump InstallationDocument7 pagespmp1000 Pump InstallationPitipong SunkhongNo ratings yet
- The National Exam Should Be Deleted Debate ScriptDocument2 pagesThe National Exam Should Be Deleted Debate ScriptPrayoga AryaNo ratings yet
- Climate Change Lesson PlanDocument2 pagesClimate Change Lesson PlanMbagnick Diop100% (1)
- Chapter 3 Lesson 1Document64 pagesChapter 3 Lesson 1Catherine PilipasNo ratings yet
- Musculoskeletal QuestionsDocument4 pagesMusculoskeletal QuestionsJen Del Mundo100% (1)
- Manila Standard Today - Friday (November 23, 2012) IssueDocument28 pagesManila Standard Today - Friday (November 23, 2012) IssueManila Standard TodayNo ratings yet
- Tenses - Active - PassiveDocument1 pageTenses - Active - PassiveAndrovisck AndroBrNo ratings yet
- Fluid Machines Lecture Notes CH-4-Centrifugal CompressorDocument21 pagesFluid Machines Lecture Notes CH-4-Centrifugal CompressorBINNo ratings yet
- Farm Input Marketting System - Arusha PresentationDocument1 pageFarm Input Marketting System - Arusha PresentationFranklin MairuraNo ratings yet
- Nomzamo The Good Wife Part 2Document5 pagesNomzamo The Good Wife Part 2prayerntandwenhleNo ratings yet
- GMS 691 Week 2Document23 pagesGMS 691 Week 2Mit DaveNo ratings yet