Download as pdf or txt
You might also like
- FM Report Download PDFDocument1 pageFM Report Download PDFNitish PonneboyinaNo ratings yet
- Rheumatology Case 1Document6 pagesRheumatology Case 1ALMIRA GUANNo ratings yet
- bsb301 New ProDocument7 pagesbsb301 New ProJasleen SohalNo ratings yet
- Problem Set: The Endocrine SystemDocument6 pagesProblem Set: The Endocrine SystemMyshaM0990% (3)
- 8 Thyroid PatternsDocument6 pages8 Thyroid Patternsmyscribkanji100% (1)
- The Poor Lab's Guide To The RegulationsDocument5 pagesThe Poor Lab's Guide To The RegulationsLeonardo HernandezNo ratings yet
- Mr. BILAL AHMAD / 96319: Test Description Observed Value Biological Reference RangeDocument1 pageMr. BILAL AHMAD / 96319: Test Description Observed Value Biological Reference Rangeusefull videosNo ratings yet
- R3Document1 pageR3Asif ButtNo ratings yet
- Susheeladevi Soni ReportsDocument2 pagesSusheeladevi Soni ReportspriyushhospitallabNo ratings yet
- Laboratory Report: Thyroid Function TestDocument2 pagesLaboratory Report: Thyroid Function Testtafiki4253No ratings yet
- Laboratory Report: Thyroid Function TestDocument2 pagesLaboratory Report: Thyroid Function Testtafiki4253No ratings yet
- Esmail Shaikh1Document1 pageEsmail Shaikh1gaikwadraju336No ratings yet
- Method: (ECLIA) : Page 1 of 1Document1 pageMethod: (ECLIA) : Page 1 of 1ashis10No ratings yet
- PdfText - 2024-05-23T161317.510Document1 pagePdfText - 2024-05-23T161317.510sirajahmad2116No ratings yet
- Laboratory Report: Thyroid Function TestDocument2 pagesLaboratory Report: Thyroid Function Testtafiki4253No ratings yet
- P.ANITHA-Female32 Years-98943Document1 pageP.ANITHA-Female32 Years-98943vijaykumarNo ratings yet
- Labreportnew - 2022-12-17T172351.750Document1 pageLabreportnew - 2022-12-17T172351.750Himanshu MaheshwariNo ratings yet
- Department of Hematology Test Name Result Unit Bio. Ref. IntervalDocument2 pagesDepartment of Hematology Test Name Result Unit Bio. Ref. IntervalRahul PandeyNo ratings yet
- Laboratorium Puskesmas Ngunut Jl. Raya 1 Ngunut Tulungagung: Pemeriksaan Hasil Satuan Nilai N/ RefDocument1 pageLaboratorium Puskesmas Ngunut Jl. Raya 1 Ngunut Tulungagung: Pemeriksaan Hasil Satuan Nilai N/ RefYustiani JasmannNo ratings yet
- Laboratory Report: Immunology Thyroid Function TestDocument1 pageLaboratory Report: Immunology Thyroid Function Testudesh LuitelNo ratings yet
- Department of Hematology Test Name Result Unit Bio. Ref. IntervalDocument5 pagesDepartment of Hematology Test Name Result Unit Bio. Ref. IntervalHarishNo ratings yet
- Roche Elecsys - TSH - FactSheetDocument2 pagesRoche Elecsys - TSH - FactSheetChris ThomasNo ratings yet
- Laboratory Report: Thyroid Function TestDocument2 pagesLaboratory Report: Thyroid Function Testtafiki4253No ratings yet
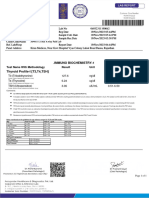
- Thyroid Profile (Total T3, Total T4, TSH), Serum: EcliaDocument3 pagesThyroid Profile (Total T3, Total T4, TSH), Serum: EcliaRoopa gowdaNo ratings yet
- mrs. SEEMA: End of ReportDocument1 pagemrs. SEEMA: End of ReportKulveer JanagalNo ratings yet
- MD1542 1250097Document1 pageMD1542 1250097Srujan SubashNo ratings yet
- Patient ReportDocument7 pagesPatient ReportY2J FilmsNo ratings yet
- Riya Majumder-23Document1 pageRiya Majumder-23Sanjoy DasNo ratings yet
- LabreportnewDocument2 pagesLabreportnewbs8403226No ratings yet
- SL-lalsa3Document3 pagesSL-lalsa3Brajesh kumarNo ratings yet
- Wa0069.Document2 pagesWa0069.mirmirshariqNo ratings yet
- Department of Hematology Test Name Result Unit Bio. Ref. IntervalDocument6 pagesDepartment of Hematology Test Name Result Unit Bio. Ref. IntervalHarishNo ratings yet
- Yjop0 968754Document2 pagesYjop0 968754Aman ThakurNo ratings yet
- CL61Document1 pageCL61ArtiNo ratings yet
- PDF TextDocument1 pagePDF TextADARSH ONLINENo ratings yet
- Harish Kumar Adwani ReportsDocument3 pagesHarish Kumar Adwani ReportspriyushhospitallabNo ratings yet
- Deepika.R:::: Patient Age / Sex 26 Y / Female BranchDocument2 pagesDeepika.R:::: Patient Age / Sex 26 Y / Female BranchkannanNo ratings yet
- Dneerajalaxmi 20220611120615333Document1 pageDneerajalaxmi 20220611120615333Donthula SripathiNo ratings yet
- Laboratory Report: Thyroid Function TestDocument2 pagesLaboratory Report: Thyroid Function Testtafiki4253No ratings yet
- BSFH 12Document9 pagesBSFH 12jinop79764No ratings yet
- Laboratory Report: Thyroid Function TestDocument2 pagesLaboratory Report: Thyroid Function Testtafiki4253No ratings yet
- L30 - Indogulf Janseva Trust Hospital Sultanpur, UTP 227817IN JagdishpurDocument2 pagesL30 - Indogulf Janseva Trust Hospital Sultanpur, UTP 227817IN Jagdishpursnehtripathi22No ratings yet
- Final Report: ArsenazoDocument2 pagesFinal Report: ArsenazoHarshitNo ratings yet
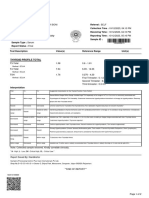
- Thyroid Function Test TotalDocument1 pageThyroid Function Test TotalShaik VeeraNo ratings yet
- Comment:: Department of Immunology Test Name Result Unit Bio. Ref. Range MethodDocument1 pageComment:: Department of Immunology Test Name Result Unit Bio. Ref. Range Methodprakash marimuthuNo ratings yet
- Champa Debnath-30Document1 pageChampa Debnath-30Sanjoy DasNo ratings yet
- Report 8cb535f0Document3 pagesReport 8cb535f0Pratistha SharmaNo ratings yet
- FRM Patient View All ReportDocument3 pagesFRM Patient View All ReportRajeev KumarNo ratings yet
- Laboratory Report: Thyroid Function TestDocument2 pagesLaboratory Report: Thyroid Function Testtafiki4253No ratings yet
- Immunology Thyroid Function TestDocument1 pageImmunology Thyroid Function TestBasanta AryalNo ratings yet
- Lab Report NewDocument2 pagesLab Report Newtyaa7301No ratings yet
- Medibuddy 12385526Document5 pagesMedibuddy 12385526gowthami sirana baluNo ratings yet
- Nazma Banu Salim ShaikhDocument3 pagesNazma Banu Salim ShaikhSHAIKH ABDUL AZIZ salim bashaNo ratings yet
- Labreportnew - 2023-08-15T114659.034Document1 pageLabreportnew - 2023-08-15T114659.034Yashi GuptaNo ratings yet
- Lab Report NewDocument2 pagesLab Report Newnsdh5v5v5sNo ratings yet
- 14 Feb 2024Document2 pages14 Feb 2024Chidambaram ANo ratings yet
- Department of Haematology: Test Name Result Unit Bio. Ref. Range MethodDocument4 pagesDepartment of Haematology: Test Name Result Unit Bio. Ref. Range MethodSiva JabilliNo ratings yet
- DR - Aazam AliDocument21 pagesDR - Aazam Alimaharanapratap1541No ratings yet
- (03241750 - Acta Medica Bulgarica) Angioedema in A Patient With Autoimmune Thyroiditis - A Case ReportDocument4 pages(03241750 - Acta Medica Bulgarica) Angioedema in A Patient With Autoimmune Thyroiditis - A Case ReportTeodorNo ratings yet
- SHAFNA Female34 Years 207392Document2 pagesSHAFNA Female34 Years 207392Muhammed DilshanNo ratings yet
- Labra, Ma. Victoria Caaya 2374003013Document1 pageLabra, Ma. Victoria Caaya 2374003013Ma. Victoria LabraNo ratings yet
- Electro-Chemiluminescence Immunoassay (ECLIA) For The in Vitro Quantitative Determination of Total Triiodothyronine in Serum and PlasmaDocument2 pagesElectro-Chemiluminescence Immunoassay (ECLIA) For The in Vitro Quantitative Determination of Total Triiodothyronine in Serum and PlasmaNkimsearNo ratings yet
- ReportViewer 1Document1 pageReportViewer 1khantula73No ratings yet
- Adult-2, Unit 1, Metabolic and EndocrineDocument157 pagesAdult-2, Unit 1, Metabolic and EndocrineBav VAansoqnuaetzNo ratings yet
- Gamma OryzanolDocument65 pagesGamma OryzanolNaiara CaramuruNo ratings yet
- DR Ananta Thyroid SlideDocument73 pagesDR Ananta Thyroid SlideRoshan Kumar PanditNo ratings yet
- SK Singh Lab Report 09042018Document8 pagesSK Singh Lab Report 09042018Iasam Groups'sNo ratings yet
- Product Preview i-CHROMA Boditech PDFDocument25 pagesProduct Preview i-CHROMA Boditech PDFUMARALEKSANA, CV100% (2)
- Mazindol On MetabolicDocument8 pagesMazindol On MetabolicCINTHYAGQNo ratings yet
- Polly Hattemer Book 4 HormonesDocument80 pagesPolly Hattemer Book 4 Hormonessusilorini100% (2)
- Simranpreet KaurDocument10 pagesSimranpreet KaurSimranpreet KaurNo ratings yet
- Campbell Biology: Concepts & Connections,: Lecture by Edward J. ZaliskoDocument87 pagesCampbell Biology: Concepts & Connections,: Lecture by Edward J. ZaliskoLawiswisNo ratings yet
- How To Interpret Thyroid Function TestDocument5 pagesHow To Interpret Thyroid Function TestSiveshKathirKamarajahNo ratings yet
- Protocols For High-Risk Pregnancies - 2010 - Queenan - Appendix B Laboratory Values in Normal PregnancyDocument9 pagesProtocols For High-Risk Pregnancies - 2010 - Queenan - Appendix B Laboratory Values in Normal PregnancyHenry VillarosaNo ratings yet
- Thyroid DisordersDocument34 pagesThyroid DisordersAbdulhameed Mohamed100% (1)
- Lab MR #: 1835640: Biochemistry Test Name (Methodology) Result Flag Units Biological Reference IntervalDocument2 pagesLab MR #: 1835640: Biochemistry Test Name (Methodology) Result Flag Units Biological Reference Intervalankit. agrawalNo ratings yet
- Graves DiseaseDocument13 pagesGraves DiseaseGerald John PazNo ratings yet
- Endocrine DisordersDocument27 pagesEndocrine Disordersasdfgrttt100% (4)
- ElvisDocument85 pagesElvisPaul SimoneNo ratings yet
- Clinical Chemistry: International Unit KatalDocument11 pagesClinical Chemistry: International Unit KatalAngelica Joy GonzalesNo ratings yet
- Thyroid Gland BasicsDocument25 pagesThyroid Gland BasicsSreekar DevarakondaNo ratings yet
- Chapter 5 WorksheetDocument7 pagesChapter 5 Worksheetapi-372001543No ratings yet
- Evaluation of TSH, T4 and T3 in Human Serum: Standardization On Normal IndividualsDocument6 pagesEvaluation of TSH, T4 and T3 in Human Serum: Standardization On Normal IndividualsTanveerNo ratings yet
- Thyroid Function Tests: A Review: G. Shivaraj, B. Desai Prakash, V. Sonal, K. Shruthi, H. Vinayak, M. AvinashDocument9 pagesThyroid Function Tests: A Review: G. Shivaraj, B. Desai Prakash, V. Sonal, K. Shruthi, H. Vinayak, M. Avinashbelakang rumahNo ratings yet
- Chapter 38 Endocrine System FunctionDocument2 pagesChapter 38 Endocrine System FunctionPaige Nicole GauthreauxNo ratings yet
- Thyroid StormDocument16 pagesThyroid StormRaquid MariaNo ratings yet
- TSH LiaisonDocument6 pagesTSH Liaisonsorayafathi90No ratings yet
- Worksheet 1 - Endocrine - 2022 (11th Ed)Document4 pagesWorksheet 1 - Endocrine - 2022 (11th Ed)ahmadmahdi18mNo ratings yet