Download as pdf or txt
You might also like
- Maintanance and Repairof Shipword MachineryDocument58 pagesMaintanance and Repairof Shipword MachineryBahtera Adi50% (2)
- What Makes Great ArtDocument45 pagesWhat Makes Great Artsaba100% (1)
- Evaluation of Green Light Exposure On Laurent MartinDocument13 pagesEvaluation of Green Light Exposure On Laurent MartinYunita Christiani BiyangNo ratings yet
- Charles 2017Document9 pagesCharles 2017Aldebaran LadoNo ratings yet
- Inbound 1186825581313765270Document16 pagesInbound 1186825581313765270NylNo ratings yet
- 47 Migraine and Its Psychiatric ComorbiditiesDocument9 pages47 Migraine and Its Psychiatric ComorbiditiesElizabeth Mautino CaceresNo ratings yet
- Chronic Migraine Pathophysiology and Treatment: A Review of Current PerspectivesDocument15 pagesChronic Migraine Pathophysiology and Treatment: A Review of Current PerspectivesJorge ZegarraNo ratings yet
- The Combined Effect of AcupuncDocument7 pagesThe Combined Effect of AcupuncnsanbaNo ratings yet
- 9.1 An Approach To Identifying Headache Patients That Require Neuroimaging (Curr, Inst and Pedagogy 2019)Document6 pages9.1 An Approach To Identifying Headache Patients That Require Neuroimaging (Curr, Inst and Pedagogy 2019)Katherine RodríguezNo ratings yet
- VSC Poster ProjectDocument1 pageVSC Poster ProjectluckyNo ratings yet
- Cognitive Effects of Migraine TreatmentDocument27 pagesCognitive Effects of Migraine TreatmentRenju KuriakoseNo ratings yet
- Aapm 08 06 81688Document6 pagesAapm 08 06 81688Asti DwiningsihNo ratings yet
- Arnadottir & Sigurdardottir, 2013 - Is Craniosacral Therapy Effective For Migrane - Tested With HIT - QuestionnaireDocument4 pagesArnadottir & Sigurdardottir, 2013 - Is Craniosacral Therapy Effective For Migrane - Tested With HIT - QuestionnaireFlávio GuimarãesNo ratings yet
- J Pharep 2017 02 019Document8 pagesJ Pharep 2017 02 019Daniel Garcia del PinoNo ratings yet
- The Use of Cannabis For Headache DisordersDocument11 pagesThe Use of Cannabis For Headache DisordersNazmi ZegarraNo ratings yet
- Headache 2: SeriesDocument9 pagesHeadache 2: SeriesAzam alausyNo ratings yet
- PDF 3961Document7 pagesPDF 3961MohammadHossein NazariNo ratings yet
- Klan Et Al 2023 Behavioral Treatment For Migraine Prophylaxis in Adults Moderator Analysis of A Randomized ControlledDocument11 pagesKlan Et Al 2023 Behavioral Treatment For Migraine Prophylaxis in Adults Moderator Analysis of A Randomized ControlledyennyNo ratings yet
- Manejo de La Migraña Crónica. Review 2022Document19 pagesManejo de La Migraña Crónica. Review 2022Edwin Fabian Paz UrbanoNo ratings yet
- MetoclopramideDocument6 pagesMetoclopramideRahmi Nurul HNo ratings yet
- Aian 22 286Document5 pagesAian 22 286gloriaNo ratings yet
- Pharmacogenetics in Primary Headache DisordersDocument27 pagesPharmacogenetics in Primary Headache DisordersJorge ZegarraNo ratings yet
- Diener May 2024 New Migraine Drugs A Critical Appraisal of The Reason Why The Majority of Migraine Patients Do NotDocument8 pagesDiener May 2024 New Migraine Drugs A Critical Appraisal of The Reason Why The Majority of Migraine Patients Do NotrenatoNo ratings yet
- Lasmiditan Migraña PerimenstrualDocument9 pagesLasmiditan Migraña Perimenstrualcepdep orgNo ratings yet
- Jackson2017 Article TricyclicAndTetracyclicAntidepDocument8 pagesJackson2017 Article TricyclicAndTetracyclicAntidepAndreas NatanNo ratings yet
- A Review of Herbal Therapy in Multiple SclerosisDocument16 pagesA Review of Herbal Therapy in Multiple Sclerosissorin.morosan64No ratings yet
- Acm 2009 0376Document10 pagesAcm 2009 0376Dr Tanu GogoiNo ratings yet
- Low-Dose Ketamine Does Not Improve Migraine in The Emergency Department A Randomized Placebo-Controlled TrialDocument9 pagesLow-Dose Ketamine Does Not Improve Migraine in The Emergency Department A Randomized Placebo-Controlled TrialRiza FirdausNo ratings yet
- MigraineDocument6 pagesMigraineNatália CândidoNo ratings yet
- Fneur 14 1160204Document9 pagesFneur 14 1160204tafazzal.eduNo ratings yet
- Altered Functional Connectivity of Amygdala Underlying The Neuromechanism of Migraine PathogenesisDocument8 pagesAltered Functional Connectivity of Amygdala Underlying The Neuromechanism of Migraine PathogenesisRizal Sven VollfiedNo ratings yet
- Primary Headache DisordersDocument12 pagesPrimary Headache DisordersririsNo ratings yet
- 2017 - Millstine Et Al - Complementary and Integrative Medicine in The Management of HeadacheDocument11 pages2017 - Millstine Et Al - Complementary and Integrative Medicine in The Management of HeadacheLélia FigueiredoNo ratings yet
- Fneur 11 570335Document9 pagesFneur 11 570335AudryaNo ratings yet
- Long Term Efficacy of Intranasal - EsketamineDocument14 pagesLong Term Efficacy of Intranasal - EsketamineCasey KaneNo ratings yet
- Characterizing Opioid Use in A US Population With MigraineDocument12 pagesCharacterizing Opioid Use in A US Population With MigraineVagner PinheiroNo ratings yet
- The Association Between Migraine and Physical Exercise: Reviewarticle Open AccessDocument9 pagesThe Association Between Migraine and Physical Exercise: Reviewarticle Open AccessAyashopia AyaNo ratings yet
- Brain Sciences: The Role of Adenosine Signaling in Headache: A ReviewDocument20 pagesBrain Sciences: The Role of Adenosine Signaling in Headache: A ReviewMarlyNationTVNo ratings yet
- Trend Watch: Treatment of Migraine and The Role of Psychiatric MedicationsDocument3 pagesTrend Watch: Treatment of Migraine and The Role of Psychiatric MedicationsCharbel Rodrigo Gonzalez SosaNo ratings yet
- Cannabis Based Medicines and Medical Cannabis For Chronic Neuropathic PainDocument14 pagesCannabis Based Medicines and Medical Cannabis For Chronic Neuropathic PainRocio BeteluNo ratings yet
- Chen 2021Document13 pagesChen 2021Aitor UzkudunNo ratings yet
- Treatment-Resistant Schizophrenia: Genetic and Neuroimaging CorrelatesDocument16 pagesTreatment-Resistant Schizophrenia: Genetic and Neuroimaging CorrelatesBianca CaterinalisendraNo ratings yet
- Intradermal Mesotherapy Versus Intravenous DexketoDocument9 pagesIntradermal Mesotherapy Versus Intravenous DexketoMetin SabuncuNo ratings yet
- Meyers 2019 Treatment Patterns and Characteristics of Patients With Migraine in Japan A Retrospective Analysis of Health Insurance Claims DataDocument17 pagesMeyers 2019 Treatment Patterns and Characteristics of Patients With Migraine in Japan A Retrospective Analysis of Health Insurance Claims DataSatra Azmia HerlandaNo ratings yet
- Cognitive Behavioral Therapy For Chronic Insomnia: A Systematic Review and Meta-AnalysisDocument16 pagesCognitive Behavioral Therapy For Chronic Insomnia: A Systematic Review and Meta-AnalysisLiezer Hernandez PinoNo ratings yet
- Ketamine NNTDocument8 pagesKetamine NNTBrent AllieNo ratings yet
- Eptinezumab in Episodic Migraine: A Randomized, Double-Blind, Placebo-Controlled Study (PROMISE-1)Document14 pagesEptinezumab in Episodic Migraine: A Randomized, Double-Blind, Placebo-Controlled Study (PROMISE-1)JUAN MANUEL CERON ALVARADONo ratings yet
- Role of Magnesium Supplementation in The Treatment of Depression: A Randomized Clinical TrialDocument15 pagesRole of Magnesium Supplementation in The Treatment of Depression: A Randomized Clinical Trialvenkat mechNo ratings yet
- NeurologiaDocument216 pagesNeurologiaPietro BracagliaNo ratings yet
- Gengibre Agudo e Enxaqueca Laís Bhering 2019Document9 pagesGengibre Agudo e Enxaqueca Laís Bhering 2019alicebarcelosbartolskiNo ratings yet
- Treatment of Depression in CADDocument15 pagesTreatment of Depression in CADjordanbadangayonNo ratings yet
- Fibromyalgia and Its New Lessons For Neuropsychiatry (2019) PDFDocument10 pagesFibromyalgia and Its New Lessons For Neuropsychiatry (2019) PDFBecados PsiquiatriaNo ratings yet
- Monti 2020Document8 pagesMonti 2020Ian MannNo ratings yet
- Fnins 13 00038Document21 pagesFnins 13 00038peludosainzNo ratings yet
- Antiseizure Medications For EpilepsyDocument13 pagesAntiseizure Medications For EpilepsyJorge CastilloNo ratings yet
- Abram Hoffer, Linus Pauling, James Greenblatt - Functional Psychiatry For Treatment of Anxiety-Psychiatry Redefined (2024)Document16 pagesAbram Hoffer, Linus Pauling, James Greenblatt - Functional Psychiatry For Treatment of Anxiety-Psychiatry Redefined (2024)Alina BreazuNo ratings yet
- Migraine and The Scope of HomeopathyDocument6 pagesMigraine and The Scope of HomeopathyDiego RodriguezNo ratings yet
- Fpsyt 12 584416Document10 pagesFpsyt 12 584416JuliaNo ratings yet
- Morbid Anxiety As A Risk Factor in Patients With Somatic Diseases A Review of Recent FindingsDocument9 pagesMorbid Anxiety As A Risk Factor in Patients With Somatic Diseases A Review of Recent FindingsAdelina AndritoiNo ratings yet
- British J Pharmacology - 2021 - ZobdehDocument20 pagesBritish J Pharmacology - 2021 - ZobdehRenju KuriakoseNo ratings yet
- Migraine Integrated Approaches To Clinical ManagementDocument14 pagesMigraine Integrated Approaches To Clinical ManagementJOHN ROMERO CEVALLOSNo ratings yet
- Migraine: The Definitive Guide to Understanding and Managing Severe HeadachesFrom EverandMigraine: The Definitive Guide to Understanding and Managing Severe HeadachesNo ratings yet
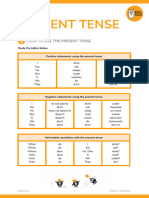
- (TV) Present TenseDocument8 pages(TV) Present TenseDe Aparicio DenisseNo ratings yet
- TUGAS INDIVIDU - 3-01 - 18 - Manajemen Keuangan - Mind Map CH 15Document1 pageTUGAS INDIVIDU - 3-01 - 18 - Manajemen Keuangan - Mind Map CH 15Ni Made Indah MeliawatiNo ratings yet
- EBS Full ReportDocument74 pagesEBS Full ReportEd SalangaNo ratings yet
- Northern SnakeheadDocument2 pagesNorthern SnakeheadrkarlinNo ratings yet
- Reviewer For CriminologyDocument6 pagesReviewer For CriminologyJoemar LucasNo ratings yet
- Embroidery Assistant: User Instruction GuideDocument92 pagesEmbroidery Assistant: User Instruction GuideAhlia Waqas AnjumNo ratings yet
- How Deep Is Your LoveDocument1 pageHow Deep Is Your LoveJanina JaworskiNo ratings yet
- Gravimetric Determination of Barium SulfateDocument3 pagesGravimetric Determination of Barium SulfateArmiee InfiniteNo ratings yet
- Media and Information Literacy Is Defined As An Access To InformationDocument2 pagesMedia and Information Literacy Is Defined As An Access To InformationmarvinNo ratings yet
- DCDC Exam BlueprintDocument2 pagesDCDC Exam BlueprintfarshathNo ratings yet
- Three-Phase Induction MotorsDocument36 pagesThree-Phase Induction MotorsCARMEN DIMITRIUNo ratings yet
- Vine-Vpdc Report As of Feb. 3, 2022Document9 pagesVine-Vpdc Report As of Feb. 3, 2022Elbert Ryan OcampoNo ratings yet
- Ca3 Week1 ModuleDocument16 pagesCa3 Week1 ModuleKate Serrano ManlutacNo ratings yet
- There's No Pill For This - IntroductionDocument4 pagesThere's No Pill For This - IntroductionChelsea Green PublishingNo ratings yet
- Test Report Quadplexer 4in1outDocument8 pagesTest Report Quadplexer 4in1outHagniAryaGunadiNo ratings yet
- DSM Mixing Tower SkyCiv ReportDocument484 pagesDSM Mixing Tower SkyCiv Reportmincho4104No ratings yet
- How The Leopard Got His Spots by Rudyard KiplingDocument4 pagesHow The Leopard Got His Spots by Rudyard KiplingProxten DsilvaNo ratings yet
- Gut DecontaminationDocument17 pagesGut DecontaminationRaju NiraulaNo ratings yet
- Assignment 2Document7 pagesAssignment 2suresh avaduthaNo ratings yet
- Chapter 7 - Cognitive DevelopmentDocument3 pagesChapter 7 - Cognitive DevelopmentmizbigspendaNo ratings yet
- Samsung Brittle Fracture Evaluation - Additional Scope P23-0105-R3Document5 pagesSamsung Brittle Fracture Evaluation - Additional Scope P23-0105-R3Vipin NairNo ratings yet
- Math InterventionDocument6 pagesMath InterventionPAOLO R. ALARDENo ratings yet
- Result Phase III - A, B - Lot (23!03!2024)Document15 pagesResult Phase III - A, B - Lot (23!03!2024)xxxlordimpalerxxxNo ratings yet
- 24 Solar TermsDocument98 pages24 Solar TermsWei Yu LowNo ratings yet
- Bob Fitts - Highest PlaceDocument2 pagesBob Fitts - Highest PlaceJosé Miguel Baute Rosado100% (1)
- Oil Pressure Transmission PT2509Document3 pagesOil Pressure Transmission PT2509Trisna TeaNo ratings yet
- 1 Notes and HW On Even Odd and NeitherDocument3 pages1 Notes and HW On Even Odd and NeitherAlin LyndaNo ratings yet
- Emami Limited: Sales ManagementDocument12 pagesEmami Limited: Sales ManagementSANYUJ ZADGAONKARNo ratings yet