
Internal Audit Progress Report
Internal Audit Progress Report
You might also like
- Haccp Manual FormatDocument17 pagesHaccp Manual FormatFarhan79% (14)
- Audit Manual Version 7Document276 pagesAudit Manual Version 7Tousief Naqvi50% (2)
- Key Performance Indicators For Internal Audit FunctionDocument10 pagesKey Performance Indicators For Internal Audit FunctionarfianNo ratings yet
- Internal Audit Annual Report PWCDocument21 pagesInternal Audit Annual Report PWCarroshan100% (14)
- Sample of Internal Audit Manual TemplateDocument51 pagesSample of Internal Audit Manual TemplateOlayinka OnimeNo ratings yet
- Real Estate Audit ReportDocument39 pagesReal Estate Audit ReportAbdalla NabagNo ratings yet
- BCM Diagnostic Tool 1Document7 pagesBCM Diagnostic Tool 1JulioIglesiasNo ratings yet
- Risk Based Internal Audit PolicyDocument257 pagesRisk Based Internal Audit PolicyHarath Chakra100% (2)
- CPA Regulation Excel NotesDocument26 pagesCPA Regulation Excel Notesjklein25880% (1)
- Fam Chapter 6 21092005Document15 pagesFam Chapter 6 21092005Humayoun Ahmad FarooqiNo ratings yet
- Hseaud - Hse Audit Program Guide - 2021Document15 pagesHseaud - Hse Audit Program Guide - 2021tharwatNo ratings yet
- Internal Audit and Controls: 9.1 OverviewDocument5 pagesInternal Audit and Controls: 9.1 Overviewhenk sterNo ratings yet
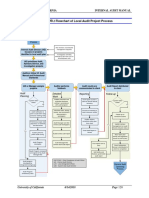
- 6000 Appendix 6000.: 2 Flowchart of Local Audit Project ProcessDocument1 page6000 Appendix 6000.: 2 Flowchart of Local Audit Project ProcessNiken RindasariNo ratings yet
- GNIA TelecomDocument159 pagesGNIA TelecomPeachyNo ratings yet
- Ational Ank of Akistan: Compliance GroupDocument54 pagesAtional Ank of Akistan: Compliance GroupMasood A. RanaNo ratings yet
- Internal Audit Reporting SPDocument45 pagesInternal Audit Reporting SPRajesh Mahesh Bohra100% (1)
- Total Combined File-1Document36 pagesTotal Combined File-1Shefali TailorNo ratings yet
- 5 Audit and Risk Management 14/03/2022 Risk Based Internal Audit Plan 2022/23 1 Purpose / SummaryDocument13 pages5 Audit and Risk Management 14/03/2022 Risk Based Internal Audit Plan 2022/23 1 Purpose / SummaryAmmar AbbasiNo ratings yet
- How To Conduct A Performance AuditDocument22 pagesHow To Conduct A Performance AuditalimeeroNo ratings yet
- 11.2 Appendix B - QAIPDocument15 pages11.2 Appendix B - QAIPQaisNo ratings yet
- Audit Manual Version 5Document247 pagesAudit Manual Version 5Mahedi100% (1)
- Purpose Statement:: IFC - IA Internal Audit Internal Financial Control Assessment Evaluation SheetDocument48 pagesPurpose Statement:: IFC - IA Internal Audit Internal Financial Control Assessment Evaluation SheetnilarolNo ratings yet
- Audit PlaningDocument14 pagesAudit PlaningFarraNo ratings yet
- 171018overview On Internal AuditDocument23 pages171018overview On Internal AuditMourad HACHCHADNo ratings yet
- Internal Audit Standard Operational Procedure Manual: Ministry of Finance and Economic DevelopmentDocument96 pagesInternal Audit Standard Operational Procedure Manual: Ministry of Finance and Economic DevelopmentDarwinNo ratings yet
- Internal Audit Unit: Department of Public Expenditure and ReformDocument8 pagesInternal Audit Unit: Department of Public Expenditure and ReformraghdaNo ratings yet
- Internal Audit Report Types 1707298159Document3 pagesInternal Audit Report Types 1707298159khanjahan1955No ratings yet
- Internal Audit Report 202122 UpdateDocument29 pagesInternal Audit Report 202122 Updateahmed khoudhiryNo ratings yet
- Improve Internal Audit MethodologyDocument48 pagesImprove Internal Audit MethodologyfaisalNo ratings yet
- Manual For Internal Audit On India Railways: Ministry of Railways (Railway Board) Government of IndiaDocument85 pagesManual For Internal Audit On India Railways: Ministry of Railways (Railway Board) Government of IndiaKannan Chakrapani100% (1)
- Audit Process Flowchart MC PDFDocument1 pageAudit Process Flowchart MC PDFDemi BangayanNo ratings yet
- STL PAF Guidelines For Performance Based Bonus FY 2022 0Document8 pagesSTL PAF Guidelines For Performance Based Bonus FY 2022 0HEALTH SERVICE CENTER - CENTRALNo ratings yet
- Appraisals ReportDocument11 pagesAppraisals ReportKevinNo ratings yet
- Internal Quality Audit ProcessDocument4 pagesInternal Quality Audit ProcessJennylyn Favila MagdadaroNo ratings yet
- Iia Whitepaper - Balanced Scorecard ReportingDocument9 pagesIia Whitepaper - Balanced Scorecard ReportingCherylNo ratings yet
- Project Auditing or Evaluation: Chapter # 5Document20 pagesProject Auditing or Evaluation: Chapter # 5Mohammad RafiqNo ratings yet
- Part 2 - 456Document5 pagesPart 2 - 456Nguyễn Hương QuỳnhNo ratings yet
- Internal Audit Annual Report and 2017 Audit Plan (PDFDrive)Document29 pagesInternal Audit Annual Report and 2017 Audit Plan (PDFDrive)samirNo ratings yet
- VMIA Internal Audit Guideline D17 46340Document35 pagesVMIA Internal Audit Guideline D17 46340official.waqaslatifNo ratings yet
- ACCO.710 Audit Process Jose Cintron, Mba: PlanningDocument30 pagesACCO.710 Audit Process Jose Cintron, Mba: Planningganesamoorthy1987No ratings yet
- Internal Audit Quality Assurance and Improvement Programme (QAIP)Document15 pagesInternal Audit Quality Assurance and Improvement Programme (QAIP)Julian McdonaldNo ratings yet
- Income Tax Audit GuidelinesDocument119 pagesIncome Tax Audit Guidelinesranibar100% (1)
- ERT ProcedureDocument7 pagesERT ProcedureHaris RisdianaNo ratings yet
- Audit Plan 6Document20 pagesAudit Plan 6Harold Dan AcebedoNo ratings yet
- KPMG Internal Audit Strategy - App 1Document3 pagesKPMG Internal Audit Strategy - App 1Martine NtebiNo ratings yet
- CIA - Wiley & Vallabhaneni Part 2Document80 pagesCIA - Wiley & Vallabhaneni Part 2Kay Cee TangalinNo ratings yet
- University of CaliforniaDocument28 pagesUniversity of CaliforniaJeenelNo ratings yet
- CIB Internal Audit Guidelines Update May2006Document57 pagesCIB Internal Audit Guidelines Update May2006Toto DushmolNo ratings yet
- QCPR08 - Internal Audit Rev 7Document3 pagesQCPR08 - Internal Audit Rev 7FAIRUZ IZYAN BINTI IBRAHIMNo ratings yet
- Subsidiary Rating Guideline - FVDocument39 pagesSubsidiary Rating Guideline - FVnefassilk branchNo ratings yet
- Audit Process PDFDocument30 pagesAudit Process PDFŘõmęõ Ji100% (2)
- Internal Audit Hand BookDocument158 pagesInternal Audit Hand BookRadhakrushna TripathyNo ratings yet
- National Accreditation Board For Testing and Calibration Laboratories (NABL)Document26 pagesNational Accreditation Board For Testing and Calibration Laboratories (NABL)sagardarbarNo ratings yet
- Quality Assessment Manual Chapter 2Document16 pagesQuality Assessment Manual Chapter 2Shandie SandikaNo ratings yet
- P018 Internal Audit Procedure: ISO 9001:2008 Clause 8.2.2Document9 pagesP018 Internal Audit Procedure: ISO 9001:2008 Clause 8.2.2Álvaro Martínez Fernández100% (1)
- Internal Audit MethadolgyDocument11 pagesInternal Audit MethadolgyAmmad UddinNo ratings yet
- Internal Audit Manual: Ministry of Finance Royal Government of Bhutan 2014Document130 pagesInternal Audit Manual: Ministry of Finance Royal Government of Bhutan 2014Juan Frivaldo100% (1)
- QAIP InternalDocument12 pagesQAIP InternalMaria Rona Silvestre100% (3)
- Audit Process: - Phase 1: Audit Plan - Phase 2: Audit Implementation - Phase 3: Audit CompletionDocument5 pagesAudit Process: - Phase 1: Audit Plan - Phase 2: Audit Implementation - Phase 3: Audit CompletionMai LinhNo ratings yet
- Strategy - PWC - Institutional Development - Performance Improvement On GECOLDocument55 pagesStrategy - PWC - Institutional Development - Performance Improvement On GECOLDavidSeowNo ratings yet
- Influence of Internal Audit and Internal Control System On Quality of The Financial StatementDocument6 pagesInfluence of Internal Audit and Internal Control System On Quality of The Financial StatementMoises PompaNo ratings yet
- Audit Report SampleDocument27 pagesAudit Report SampleshanifNo ratings yet
- IAD - Internal Audit Plan FY14Document7 pagesIAD - Internal Audit Plan FY14Adnan MohammedNo ratings yet
- How to Comply with Sarbanes-Oxley Section 404: Assessing the Effectiveness of Internal ControlFrom EverandHow to Comply with Sarbanes-Oxley Section 404: Assessing the Effectiveness of Internal ControlNo ratings yet
- Talha Abdul RazzaqDocument2 pagesTalha Abdul RazzaqAhmad fayyazNo ratings yet
- 04035720221214121332Document1 page04035720221214121332Ahmad fayyaz100% (1)
- Abdullah Alshaghab - CV - March 2016Document3 pagesAbdullah Alshaghab - CV - March 2016Ahmad fayyazNo ratings yet
- Candidate Affidavit Form (New)Document1 pageCandidate Affidavit Form (New)Ahmad fayyazNo ratings yet
- BTMIQ ProfileDocument21 pagesBTMIQ ProfilealiNo ratings yet
- BS OHSAS 18001 Implementation GuideDocument12 pagesBS OHSAS 18001 Implementation GuideAditya BagrolaNo ratings yet
- Audit of Bank Mcom Part 2Document20 pagesAudit of Bank Mcom Part 2sumi1992No ratings yet
- Vikas TyagiDocument3 pagesVikas TyagiVicki jonesNo ratings yet
- MR KUMARMANGALAM BIRLA REPORTDocument33 pagesMR KUMARMANGALAM BIRLA REPORTUday SethiNo ratings yet
- Fauji Cement: Financial Accounting Project ReportDocument7 pagesFauji Cement: Financial Accounting Project ReportMuhammad SabihNo ratings yet
- Abiola MosesDocument3 pagesAbiola MosesJaclyn ThomasNo ratings yet
- Auditing in CadburyDocument50 pagesAuditing in CadburyRohit YadavNo ratings yet
- ShannonfoynespcDocument53 pagesShannonfoynespcthestorydotieNo ratings yet
- IMS Case PresentationDocument2 pagesIMS Case PresentationLakshyaKumarNo ratings yet
- Training Benchmark Report 2016 Ethics & Compliance: Data and Insights To Get More Value From Your ProgramDocument46 pagesTraining Benchmark Report 2016 Ethics & Compliance: Data and Insights To Get More Value From Your Programlalagabrielle613No ratings yet
- Audit Summary13Document6 pagesAudit Summary13Gerrive OliverosNo ratings yet
- Imran Essani - ACMA, FPFA: ObjectiveDocument4 pagesImran Essani - ACMA, FPFA: ObjectiveRukhshindaNo ratings yet
- Water Ups MPC Internal Control Manual For 2019Document96 pagesWater Ups MPC Internal Control Manual For 2019Dharb Cabahug100% (1)
- 3 Understanding of The Entity and Its EnvironmentDocument36 pages3 Understanding of The Entity and Its EnvironmentJenny JohnNo ratings yet
- Sub Vendor Audit Checklist-PersonnelDocument5 pagesSub Vendor Audit Checklist-PersonnelaszlizaNo ratings yet
- Ghafar Muzanni: PT. Budi Karya Energi Nusantara (Coal and Mining)Document3 pagesGhafar Muzanni: PT. Budi Karya Energi Nusantara (Coal and Mining)Ghafar MuzanniNo ratings yet
- Auditing Theory Finals PDF FreeDocument11 pagesAuditing Theory Finals PDF FreeMichael Brian TorresNo ratings yet
- Internal Auditing Practice A Case Study On Awash International Bank Jimma BranchDocument39 pagesInternal Auditing Practice A Case Study On Awash International Bank Jimma BranchBereket Desalegn100% (4)
- AML Training Preparing Auditors To Adequately Assess AML Programs Jack SonnenscheinDocument11 pagesAML Training Preparing Auditors To Adequately Assess AML Programs Jack SonnenscheinEmin SaftarovNo ratings yet
- Pas 99: 2012 Integreted ManagementDocument8 pagesPas 99: 2012 Integreted ManagementPrisman Cahya NugrahaNo ratings yet
- 05 - ACC653 Questions WK1Document3 pages05 - ACC653 Questions WK1Camilo ToroNo ratings yet
- Acca F8 Lectures PDFDocument143 pagesAcca F8 Lectures PDFBin SaadunNo ratings yet
- National Clearing Company of Pakistan LimitedDocument96 pagesNational Clearing Company of Pakistan LimitedArslan AhmadNo ratings yet
- DNV's Maritime Academy Schedule 2021 (September-December)Document3 pagesDNV's Maritime Academy Schedule 2021 (September-December)Fotini HalouvaNo ratings yet
- Letter Head IASODocument3 pagesLetter Head IASOeubie ardenaNo ratings yet



























































































Download as pdf or txt
You might also like
- Haccp Manual FormatDocument17 pagesHaccp Manual FormatFarhan79% (14)
- Audit Manual Version 7Document276 pagesAudit Manual Version 7Tousief Naqvi50% (2)
- Key Performance Indicators For Internal Audit FunctionDocument10 pagesKey Performance Indicators For Internal Audit FunctionarfianNo ratings yet
- Internal Audit Annual Report PWCDocument21 pagesInternal Audit Annual Report PWCarroshan100% (14)
- Sample of Internal Audit Manual TemplateDocument51 pagesSample of Internal Audit Manual TemplateOlayinka OnimeNo ratings yet
- Real Estate Audit ReportDocument39 pagesReal Estate Audit ReportAbdalla NabagNo ratings yet
- BCM Diagnostic Tool 1Document7 pagesBCM Diagnostic Tool 1JulioIglesiasNo ratings yet
- Risk Based Internal Audit PolicyDocument257 pagesRisk Based Internal Audit PolicyHarath Chakra100% (2)
- CPA Regulation Excel NotesDocument26 pagesCPA Regulation Excel Notesjklein25880% (1)
- Fam Chapter 6 21092005Document15 pagesFam Chapter 6 21092005Humayoun Ahmad FarooqiNo ratings yet
- Hseaud - Hse Audit Program Guide - 2021Document15 pagesHseaud - Hse Audit Program Guide - 2021tharwatNo ratings yet
- Internal Audit and Controls: 9.1 OverviewDocument5 pagesInternal Audit and Controls: 9.1 Overviewhenk sterNo ratings yet
- 6000 Appendix 6000.: 2 Flowchart of Local Audit Project ProcessDocument1 page6000 Appendix 6000.: 2 Flowchart of Local Audit Project ProcessNiken RindasariNo ratings yet
- GNIA TelecomDocument159 pagesGNIA TelecomPeachyNo ratings yet
- Ational Ank of Akistan: Compliance GroupDocument54 pagesAtional Ank of Akistan: Compliance GroupMasood A. RanaNo ratings yet
- Internal Audit Reporting SPDocument45 pagesInternal Audit Reporting SPRajesh Mahesh Bohra100% (1)
- Total Combined File-1Document36 pagesTotal Combined File-1Shefali TailorNo ratings yet
- 5 Audit and Risk Management 14/03/2022 Risk Based Internal Audit Plan 2022/23 1 Purpose / SummaryDocument13 pages5 Audit and Risk Management 14/03/2022 Risk Based Internal Audit Plan 2022/23 1 Purpose / SummaryAmmar AbbasiNo ratings yet
- How To Conduct A Performance AuditDocument22 pagesHow To Conduct A Performance AuditalimeeroNo ratings yet
- 11.2 Appendix B - QAIPDocument15 pages11.2 Appendix B - QAIPQaisNo ratings yet
- Audit Manual Version 5Document247 pagesAudit Manual Version 5Mahedi100% (1)
- Purpose Statement:: IFC - IA Internal Audit Internal Financial Control Assessment Evaluation SheetDocument48 pagesPurpose Statement:: IFC - IA Internal Audit Internal Financial Control Assessment Evaluation SheetnilarolNo ratings yet
- Audit PlaningDocument14 pagesAudit PlaningFarraNo ratings yet
- 171018overview On Internal AuditDocument23 pages171018overview On Internal AuditMourad HACHCHADNo ratings yet
- Internal Audit Standard Operational Procedure Manual: Ministry of Finance and Economic DevelopmentDocument96 pagesInternal Audit Standard Operational Procedure Manual: Ministry of Finance and Economic DevelopmentDarwinNo ratings yet
- Internal Audit Unit: Department of Public Expenditure and ReformDocument8 pagesInternal Audit Unit: Department of Public Expenditure and ReformraghdaNo ratings yet
- Internal Audit Report Types 1707298159Document3 pagesInternal Audit Report Types 1707298159khanjahan1955No ratings yet
- Internal Audit Report 202122 UpdateDocument29 pagesInternal Audit Report 202122 Updateahmed khoudhiryNo ratings yet
- Improve Internal Audit MethodologyDocument48 pagesImprove Internal Audit MethodologyfaisalNo ratings yet
- Manual For Internal Audit On India Railways: Ministry of Railways (Railway Board) Government of IndiaDocument85 pagesManual For Internal Audit On India Railways: Ministry of Railways (Railway Board) Government of IndiaKannan Chakrapani100% (1)
- Audit Process Flowchart MC PDFDocument1 pageAudit Process Flowchart MC PDFDemi BangayanNo ratings yet
- STL PAF Guidelines For Performance Based Bonus FY 2022 0Document8 pagesSTL PAF Guidelines For Performance Based Bonus FY 2022 0HEALTH SERVICE CENTER - CENTRALNo ratings yet
- Appraisals ReportDocument11 pagesAppraisals ReportKevinNo ratings yet
- Internal Quality Audit ProcessDocument4 pagesInternal Quality Audit ProcessJennylyn Favila MagdadaroNo ratings yet
- Iia Whitepaper - Balanced Scorecard ReportingDocument9 pagesIia Whitepaper - Balanced Scorecard ReportingCherylNo ratings yet
- Project Auditing or Evaluation: Chapter # 5Document20 pagesProject Auditing or Evaluation: Chapter # 5Mohammad RafiqNo ratings yet
- Part 2 - 456Document5 pagesPart 2 - 456Nguyễn Hương QuỳnhNo ratings yet
- Internal Audit Annual Report and 2017 Audit Plan (PDFDrive)Document29 pagesInternal Audit Annual Report and 2017 Audit Plan (PDFDrive)samirNo ratings yet
- VMIA Internal Audit Guideline D17 46340Document35 pagesVMIA Internal Audit Guideline D17 46340official.waqaslatifNo ratings yet
- ACCO.710 Audit Process Jose Cintron, Mba: PlanningDocument30 pagesACCO.710 Audit Process Jose Cintron, Mba: Planningganesamoorthy1987No ratings yet
- Internal Audit Quality Assurance and Improvement Programme (QAIP)Document15 pagesInternal Audit Quality Assurance and Improvement Programme (QAIP)Julian McdonaldNo ratings yet
- Income Tax Audit GuidelinesDocument119 pagesIncome Tax Audit Guidelinesranibar100% (1)
- ERT ProcedureDocument7 pagesERT ProcedureHaris RisdianaNo ratings yet
- Audit Plan 6Document20 pagesAudit Plan 6Harold Dan AcebedoNo ratings yet
- KPMG Internal Audit Strategy - App 1Document3 pagesKPMG Internal Audit Strategy - App 1Martine NtebiNo ratings yet
- CIA - Wiley & Vallabhaneni Part 2Document80 pagesCIA - Wiley & Vallabhaneni Part 2Kay Cee TangalinNo ratings yet
- University of CaliforniaDocument28 pagesUniversity of CaliforniaJeenelNo ratings yet
- CIB Internal Audit Guidelines Update May2006Document57 pagesCIB Internal Audit Guidelines Update May2006Toto DushmolNo ratings yet
- QCPR08 - Internal Audit Rev 7Document3 pagesQCPR08 - Internal Audit Rev 7FAIRUZ IZYAN BINTI IBRAHIMNo ratings yet
- Subsidiary Rating Guideline - FVDocument39 pagesSubsidiary Rating Guideline - FVnefassilk branchNo ratings yet
- Audit Process PDFDocument30 pagesAudit Process PDFŘõmęõ Ji100% (2)
- Internal Audit Hand BookDocument158 pagesInternal Audit Hand BookRadhakrushna TripathyNo ratings yet
- National Accreditation Board For Testing and Calibration Laboratories (NABL)Document26 pagesNational Accreditation Board For Testing and Calibration Laboratories (NABL)sagardarbarNo ratings yet
- Quality Assessment Manual Chapter 2Document16 pagesQuality Assessment Manual Chapter 2Shandie SandikaNo ratings yet
- P018 Internal Audit Procedure: ISO 9001:2008 Clause 8.2.2Document9 pagesP018 Internal Audit Procedure: ISO 9001:2008 Clause 8.2.2Álvaro Martínez Fernández100% (1)
- Internal Audit MethadolgyDocument11 pagesInternal Audit MethadolgyAmmad UddinNo ratings yet
- Internal Audit Manual: Ministry of Finance Royal Government of Bhutan 2014Document130 pagesInternal Audit Manual: Ministry of Finance Royal Government of Bhutan 2014Juan Frivaldo100% (1)
- QAIP InternalDocument12 pagesQAIP InternalMaria Rona Silvestre100% (3)
- Audit Process: - Phase 1: Audit Plan - Phase 2: Audit Implementation - Phase 3: Audit CompletionDocument5 pagesAudit Process: - Phase 1: Audit Plan - Phase 2: Audit Implementation - Phase 3: Audit CompletionMai LinhNo ratings yet
- Strategy - PWC - Institutional Development - Performance Improvement On GECOLDocument55 pagesStrategy - PWC - Institutional Development - Performance Improvement On GECOLDavidSeowNo ratings yet
- Influence of Internal Audit and Internal Control System On Quality of The Financial StatementDocument6 pagesInfluence of Internal Audit and Internal Control System On Quality of The Financial StatementMoises PompaNo ratings yet
- Audit Report SampleDocument27 pagesAudit Report SampleshanifNo ratings yet
- IAD - Internal Audit Plan FY14Document7 pagesIAD - Internal Audit Plan FY14Adnan MohammedNo ratings yet
- How to Comply with Sarbanes-Oxley Section 404: Assessing the Effectiveness of Internal ControlFrom EverandHow to Comply with Sarbanes-Oxley Section 404: Assessing the Effectiveness of Internal ControlNo ratings yet
- Talha Abdul RazzaqDocument2 pagesTalha Abdul RazzaqAhmad fayyazNo ratings yet
- 04035720221214121332Document1 page04035720221214121332Ahmad fayyaz100% (1)
- Abdullah Alshaghab - CV - March 2016Document3 pagesAbdullah Alshaghab - CV - March 2016Ahmad fayyazNo ratings yet
- Candidate Affidavit Form (New)Document1 pageCandidate Affidavit Form (New)Ahmad fayyazNo ratings yet
- BTMIQ ProfileDocument21 pagesBTMIQ ProfilealiNo ratings yet
- BS OHSAS 18001 Implementation GuideDocument12 pagesBS OHSAS 18001 Implementation GuideAditya BagrolaNo ratings yet
- Audit of Bank Mcom Part 2Document20 pagesAudit of Bank Mcom Part 2sumi1992No ratings yet
- Vikas TyagiDocument3 pagesVikas TyagiVicki jonesNo ratings yet
- MR KUMARMANGALAM BIRLA REPORTDocument33 pagesMR KUMARMANGALAM BIRLA REPORTUday SethiNo ratings yet
- Fauji Cement: Financial Accounting Project ReportDocument7 pagesFauji Cement: Financial Accounting Project ReportMuhammad SabihNo ratings yet
- Abiola MosesDocument3 pagesAbiola MosesJaclyn ThomasNo ratings yet
- Auditing in CadburyDocument50 pagesAuditing in CadburyRohit YadavNo ratings yet
- ShannonfoynespcDocument53 pagesShannonfoynespcthestorydotieNo ratings yet
- IMS Case PresentationDocument2 pagesIMS Case PresentationLakshyaKumarNo ratings yet
- Training Benchmark Report 2016 Ethics & Compliance: Data and Insights To Get More Value From Your ProgramDocument46 pagesTraining Benchmark Report 2016 Ethics & Compliance: Data and Insights To Get More Value From Your Programlalagabrielle613No ratings yet
- Audit Summary13Document6 pagesAudit Summary13Gerrive OliverosNo ratings yet
- Imran Essani - ACMA, FPFA: ObjectiveDocument4 pagesImran Essani - ACMA, FPFA: ObjectiveRukhshindaNo ratings yet
- Water Ups MPC Internal Control Manual For 2019Document96 pagesWater Ups MPC Internal Control Manual For 2019Dharb Cabahug100% (1)
- 3 Understanding of The Entity and Its EnvironmentDocument36 pages3 Understanding of The Entity and Its EnvironmentJenny JohnNo ratings yet
- Sub Vendor Audit Checklist-PersonnelDocument5 pagesSub Vendor Audit Checklist-PersonnelaszlizaNo ratings yet
- Ghafar Muzanni: PT. Budi Karya Energi Nusantara (Coal and Mining)Document3 pagesGhafar Muzanni: PT. Budi Karya Energi Nusantara (Coal and Mining)Ghafar MuzanniNo ratings yet
- Auditing Theory Finals PDF FreeDocument11 pagesAuditing Theory Finals PDF FreeMichael Brian TorresNo ratings yet
- Internal Auditing Practice A Case Study On Awash International Bank Jimma BranchDocument39 pagesInternal Auditing Practice A Case Study On Awash International Bank Jimma BranchBereket Desalegn100% (4)
- AML Training Preparing Auditors To Adequately Assess AML Programs Jack SonnenscheinDocument11 pagesAML Training Preparing Auditors To Adequately Assess AML Programs Jack SonnenscheinEmin SaftarovNo ratings yet
- Pas 99: 2012 Integreted ManagementDocument8 pagesPas 99: 2012 Integreted ManagementPrisman Cahya NugrahaNo ratings yet
- 05 - ACC653 Questions WK1Document3 pages05 - ACC653 Questions WK1Camilo ToroNo ratings yet
- Acca F8 Lectures PDFDocument143 pagesAcca F8 Lectures PDFBin SaadunNo ratings yet
- National Clearing Company of Pakistan LimitedDocument96 pagesNational Clearing Company of Pakistan LimitedArslan AhmadNo ratings yet
- DNV's Maritime Academy Schedule 2021 (September-December)Document3 pagesDNV's Maritime Academy Schedule 2021 (September-December)Fotini HalouvaNo ratings yet
- Letter Head IASODocument3 pagesLetter Head IASOeubie ardenaNo ratings yet