Download as pdf or txt
You might also like
- Double-V-Weld Consumption Formula in Excel SheetDocument6 pagesDouble-V-Weld Consumption Formula in Excel SheetvinothNo ratings yet
- Journal of Orthopaedic Science and ResearchDocument12 pagesJournal of Orthopaedic Science and ResearchAthenaeum Scientific PublishersNo ratings yet
- Lee 2021 2Document10 pagesLee 2021 2Aaron BNo ratings yet
- Brief Resume of Intended WorkDocument7 pagesBrief Resume of Intended WorkNavin ChandarNo ratings yet
- Tecnica de ChampyDocument7 pagesTecnica de Champyboye022694No ratings yet
- Surgical Treatment of Metastatic Tumors of The FemurDocument6 pagesSurgical Treatment of Metastatic Tumors of The FemurHitham El ShahatNo ratings yet
- Endoscopically Access YANG - TMJ ProsthesisDocument6 pagesEndoscopically Access YANG - TMJ ProsthesisClínica BMFNo ratings yet
- AJODO-2013 Bradley 143 5 599Document3 pagesAJODO-2013 Bradley 143 5 599player osamaNo ratings yet
- Open Surgery Assisted With Arthroscopy To Treat Synovial Chondromatosis of The Temporomandibular Joint 2Document6 pagesOpen Surgery Assisted With Arthroscopy To Treat Synovial Chondromatosis of The Temporomandibular Joint 2Ario LovellyNo ratings yet
- J Odw 2016 11 006Document6 pagesJ Odw 2016 11 006Ahmed ElsharkawyNo ratings yet
- Claus 2019Document8 pagesClaus 2019abhishekjha0082No ratings yet
- 1 UsDocument7 pages1 UsJenny VibsNo ratings yet
- JC10Document43 pagesJC10ananyasrivastava.013No ratings yet
- H.NO 9-4-110/3/56, Virasath Nagar, Tolichowki, HYDERABAD-500008 Andhra Pradesh PHONE NO: 04023562340/04024571530Document8 pagesH.NO 9-4-110/3/56, Virasath Nagar, Tolichowki, HYDERABAD-500008 Andhra Pradesh PHONE NO: 04023562340/04024571530haneefmdfNo ratings yet
- Two Years Outcome of Cemented Austin Moore HemiartDocument7 pagesTwo Years Outcome of Cemented Austin Moore HemiartIkram HussainNo ratings yet
- Modified Gap Arthroplasty and Myrhaugs Incision As A Treatment Option in Management of Temporomandibular Joint Ankylosis A Study of 10 CasesDocument6 pagesModified Gap Arthroplasty and Myrhaugs Incision As A Treatment Option in Management of Temporomandibular Joint Ankylosis A Study of 10 CasesS EllurNo ratings yet
- He 2019Document10 pagesHe 2019Rashif AkmalNo ratings yet
- En V79n2a07Document5 pagesEn V79n2a07susanti bulanNo ratings yet
- Arthroscopic Hip Surgery With A Microfracture Procedure of The Hip: Clinical Outcomes With Two-Year Follow-UpDocument10 pagesArthroscopic Hip Surgery With A Microfracture Procedure of The Hip: Clinical Outcomes With Two-Year Follow-Upmoonwalker2099No ratings yet
- ED-Journal 2015 Vol.61 October: Part VDocument5 pagesED-Journal 2015 Vol.61 October: Part VsalahoveNo ratings yet
- Cantarella2018 DisyunciónDocument9 pagesCantarella2018 DisyunciónFernando Ruiz BorsiniNo ratings yet
- 2019 - Comparison of Bite Force in Patients After Treatment of Mandibular Fractures With 3-Dimensional Locking Miniplate and Standard MiniplatesDocument4 pages2019 - Comparison of Bite Force in Patients After Treatment of Mandibular Fractures With 3-Dimensional Locking Miniplate and Standard MiniplatesLeandro Nascimento Rodrigues dos santosNo ratings yet
- Sarimo 2011Document4 pagesSarimo 2011Pe T. ErNo ratings yet
- Madhusudhan2008 Article ClinicalExaminationMRIAndArthrDocument6 pagesMadhusudhan2008 Article ClinicalExaminationMRIAndArthrMaddy WolsmenNo ratings yet
- IJOS Published ArticleDocument5 pagesIJOS Published ArticleManish ShahNo ratings yet
- Alternative Buccal Fat Pad PDFDocument15 pagesAlternative Buccal Fat Pad PDFjaycgmailNo ratings yet
- PFN PaperDocument7 pagesPFN PaperNisar Ahmed DarNo ratings yet
- Base Segudo Caso ClinicoDocument6 pagesBase Segudo Caso Clinicogatos965669988No ratings yet
- Treatment Strategyfor Irreparable Rotator Cuff TearsDocument16 pagesTreatment Strategyfor Irreparable Rotator Cuff TearshawkjohnNo ratings yet
- Traatment Gonatroza Prin ArthroplastieDocument5 pagesTraatment Gonatroza Prin Arthroplastieandre_moarcasNo ratings yet
- Patient Expectations and Satisfaction Following Orthognathic SurgeryDocument6 pagesPatient Expectations and Satisfaction Following Orthognathic SurgerySooraj SNo ratings yet
- Jurnal PfnaDocument10 pagesJurnal PfnaDhea Amalia WibowoNo ratings yet
- Research ArticleDocument9 pagesResearch ArticleAni LabibahNo ratings yet
- A Study On Management of Bothbones Forearm Fractures With Dynamic Compression PlateDocument5 pagesA Study On Management of Bothbones Forearm Fractures With Dynamic Compression PlateIOSRjournalNo ratings yet
- Effective Use of Viscosupplementation After Knee Arthroscopy: Experience From A Working GroupDocument10 pagesEffective Use of Viscosupplementation After Knee Arthroscopy: Experience From A Working GroupIJAR JOURNALNo ratings yet
- Evaluation of Reused Orthodontic Mini Implants On Stability An inDocument6 pagesEvaluation of Reused Orthodontic Mini Implants On Stability An inSajjad alipourNo ratings yet
- Young KyunDocument6 pagesYoung Kyunodontologia uvNo ratings yet
- Quirurgico PDFDocument10 pagesQuirurgico PDFrosaNo ratings yet
- Paper 38Document6 pagesPaper 38Dr Vineet KumarNo ratings yet
- Atraumatic Cuff TearsDocument7 pagesAtraumatic Cuff Tearschandan noelNo ratings yet
- 20SPIGCDocument3 pages20SPIGCscribullNo ratings yet
- Outcomes of Micro FractureDocument8 pagesOutcomes of Micro FractureTiago SantosNo ratings yet
- The Piezoelectric and Rotatory Osteotomy Technique in Impacted Third Molar Surgery: Comparison Of..Document6 pagesThe Piezoelectric and Rotatory Osteotomy Technique in Impacted Third Molar Surgery: Comparison Of..Hoàng VũNo ratings yet
- Anterior Versus Posterior Surgical Approach For Lumbosacral TuberculosisDocument9 pagesAnterior Versus Posterior Surgical Approach For Lumbosacral TuberculosisI Made Dhita PriantharaNo ratings yet
- The Effect of Mandibular Setback or Two-Jaws Surgery On Pharyngeal Airway Among Different GendersDocument6 pagesThe Effect of Mandibular Setback or Two-Jaws Surgery On Pharyngeal Airway Among Different GenderslalajanNo ratings yet
- Comparison Surgical Lengthening: Clinical of Desired Versus Actual Amount of CrownDocument4 pagesComparison Surgical Lengthening: Clinical of Desired Versus Actual Amount of CrownOana DimaNo ratings yet
- J Neurol Sci (Turk)Document9 pagesJ Neurol Sci (Turk)nulaeli Siti ANo ratings yet
- Comparison-Of-Two-Osteotomy-Techniques-For-Tibial-Lengthening 2004Document3 pagesComparison-Of-Two-Osteotomy-Techniques-For-Tibial-Lengthening 2004aymanNo ratings yet
- External Rotator Sparing W KL in Post Acetab FX Hindawi14Document7 pagesExternal Rotator Sparing W KL in Post Acetab FX Hindawi14Antonio PáezNo ratings yet
- Treatment of Class II Malocclusion With Mandibular Skeletal AnchorageDocument9 pagesTreatment of Class II Malocclusion With Mandibular Skeletal AnchorageAnonymous 9PcFdakHcNo ratings yet
- X Clinically Important Reductions in Physical.32Document14 pagesX Clinically Important Reductions in Physical.32cooperorthopaedicsNo ratings yet
- Degala S.Document8 pagesDegala S.odontologia uvNo ratings yet
- Drughelp - Care 6.22Document10 pagesDrughelp - Care 6.22Joko RifaiNo ratings yet
- Long-Term Changes of The Anterior Palatal Alveolar Bone After Treatment With Bialveolar Protrusion, Evaluated With Computed TomographyDocument10 pagesLong-Term Changes of The Anterior Palatal Alveolar Bone After Treatment With Bialveolar Protrusion, Evaluated With Computed TomographyMonojit DuttaNo ratings yet
- Chen 2019Document8 pagesChen 2019Ahmad AlzawahrehNo ratings yet
- Piezosurgery Versus Rotatory Osteotomy in Mandibular Impacted Third Molar ExtractionDocument17 pagesPiezosurgery Versus Rotatory Osteotomy in Mandibular Impacted Third Molar ExtractionHUYNH TRINHNo ratings yet
- 1753193410377845Document5 pages1753193410377845milenabogojevskaNo ratings yet
- Cel MM Derivadas de Almohadilla de Grasa Infrapatelar para Tto de Osteoartritis de RodillaDocument6 pagesCel MM Derivadas de Almohadilla de Grasa Infrapatelar para Tto de Osteoartritis de RodillaDIEGONo ratings yet
- 1 s2.0 S0266435613004105 MainDocument5 pages1 s2.0 S0266435613004105 MainMr-Ton DrgNo ratings yet
- The SAGES Manual of Biliary SurgeryFrom EverandThe SAGES Manual of Biliary SurgeryHoracio J. AsbunNo ratings yet
- Basic of Economics - NMP - EMPDocument47 pagesBasic of Economics - NMP - EMPsanchaita kohliNo ratings yet
- Microeconomics - Oligopoly-MonoCompetition - NewDocument37 pagesMicroeconomics - Oligopoly-MonoCompetition - Newsanchaita kohliNo ratings yet
- Cysticercosis of The Temporalis MuscleDocument4 pagesCysticercosis of The Temporalis Musclesanchaita kohliNo ratings yet
- Novel Surgical Technique For Clavicle Graft HarvestDocument5 pagesNovel Surgical Technique For Clavicle Graft Harvestsanchaita kohliNo ratings yet
- Fate of The Coronoid ProcessDocument11 pagesFate of The Coronoid Processsanchaita kohliNo ratings yet
- Computer Modelling Group (CMG) TutorialDocument7 pagesComputer Modelling Group (CMG) TutorialMade Ray Yuda SuyatnaNo ratings yet
- Chemical Kinetics: Chemistry: The Molecular Nature of Matter, 6EDocument128 pagesChemical Kinetics: Chemistry: The Molecular Nature of Matter, 6Eamel andiniNo ratings yet
- Europass CV 111004 GalanisDocument2 pagesEuropass CV 111004 GalanisGeorge MastorakisNo ratings yet
- Chapter 3Document39 pagesChapter 3amiranurul50% (2)
- Reproduction of VirusesDocument26 pagesReproduction of VirusesRidham DewalNo ratings yet
- Effects of Grape Seed Oil Nanoemulsion On Physicochemical and Antibacterial Properties of Gelatin Sodium Alginate Film BlendsDocument12 pagesEffects of Grape Seed Oil Nanoemulsion On Physicochemical and Antibacterial Properties of Gelatin Sodium Alginate Film BlendsMohammad Hamayoon Norri100% (1)
- PMTCTDocument14 pagesPMTCTPINANo ratings yet
- Title: Corrosion of Steel Reinforcement in Concrete and The Methods of Protection and MitigationDocument23 pagesTitle: Corrosion of Steel Reinforcement in Concrete and The Methods of Protection and MitigationMohammad AL HaririNo ratings yet
- Agriculture Management Approaches Pankaj Kumar Saraswat Full ChapterDocument51 pagesAgriculture Management Approaches Pankaj Kumar Saraswat Full Chapterhomer.griffin661100% (9)
- Quante CDocument4 pagesQuante CAnonymous faRVVGNNo ratings yet
- Ultra Flash CSFB 10dec2020Document15 pagesUltra Flash CSFB 10dec2020hamadashraf301No ratings yet
- HRDM 11-7 - WEEK 06 To 07 - Activity and Output - Ma. Christine C. MontejoDocument13 pagesHRDM 11-7 - WEEK 06 To 07 - Activity and Output - Ma. Christine C. Montejochristine montejoNo ratings yet
- J - Acid Sulfate Soil Borehole LogsDocument7 pagesJ - Acid Sulfate Soil Borehole LogsRoshan MalhotraNo ratings yet
- Isa Cem: Comparatives and SuperlativesDocument7 pagesIsa Cem: Comparatives and SuperlativesAnonymous 7xhhVAWCXNo ratings yet
- TuberculosisDocument9 pagesTuberculosisIdasari DewiNo ratings yet
- Medieval Iron MakingDocument45 pagesMedieval Iron MakingEdvards Puciriuss100% (1)
- Density Measurement For Ceramics A New SolutionDocument7 pagesDensity Measurement For Ceramics A New Solutionfullagar1No ratings yet
- Flanges: Figure 71 Flange Adapter (ANSI Class 125/150)Document2 pagesFlanges: Figure 71 Flange Adapter (ANSI Class 125/150)Mina MagdyNo ratings yet
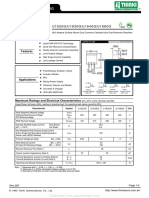
- U1620G Thru U1660G: U1620G/U1630G/U1640G/U1660GDocument2 pagesU1620G Thru U1660G: U1620G/U1630G/U1640G/U1660GTeles SilvaNo ratings yet
- s555qw5w60101011010 Scalloppsnskskdndndn D Scalllpssond Sjsjsns S 3u373636191ir827472y152ta D D. DJDNDJFNFNF Ala. K K J N K nk755555511112727273737 11515152t2cawuwuwu272727 1116263636bllop - 1Document4 pagess555qw5w60101011010 Scalloppsnskskdndndn D Scalllpssond Sjsjsns S 3u373636191ir827472y152ta D D. DJDNDJFNFNF Ala. K K J N K nk755555511112727273737 11515152t2cawuwuwu272727 1116263636bllop - 1Red DiggerNo ratings yet
- Instant Download Psychological Science Modeling Scientific Literacy 1st Edition Krause Test Bank PDF Full ChapterDocument32 pagesInstant Download Psychological Science Modeling Scientific Literacy 1st Edition Krause Test Bank PDF Full ChapterAdrianSmitheqim100% (9)
- Fpsyt 14 1244451Document8 pagesFpsyt 14 1244451Gilvan RangelNo ratings yet
- Kelvion - Ficha TecnicaDocument76 pagesKelvion - Ficha TecnicaRusbel Dominguez AntonioNo ratings yet
- 7 Installation of SilencerDocument8 pages7 Installation of SilencerktsnlNo ratings yet
- Tel: Ashrae Duct Fitting Database Fax: Version # 6. 00.04 08 March 2023Document5 pagesTel: Ashrae Duct Fitting Database Fax: Version # 6. 00.04 08 March 2023pkp indiaNo ratings yet
- Pregnancy TestDocument2 pagesPregnancy TestOsinachi WilsonNo ratings yet
- Human Values & Professional EthicsDocument158 pagesHuman Values & Professional EthicsRaj Kumar67% (9)
- CATALOGODocument54 pagesCATALOGOYineth Escobar ChausaNo ratings yet
- PDFDocument72 pagesPDFAkhmad Ulil AlbabNo ratings yet