
4.1 Pemphigus: Case 38 Pemphigus Vulgaris (Involving The Skin and Oral Mucosa) B
4.1 Pemphigus: Case 38 Pemphigus Vulgaris (Involving The Skin and Oral Mucosa) B
You might also like
- Side Lifter Shop Manual SteelbroDocument743 pagesSide Lifter Shop Manual SteelbroYandier Martínez100% (1)
- Yamaha Owners Manual 40 50 HPDocument88 pagesYamaha Owners Manual 40 50 HPmnbvqwert100% (5)
- Sick VerseDocument503 pagesSick Verselozerface88100% (3)
- 13 Principles of Wiccan BeliefDocument7 pages13 Principles of Wiccan BeliefWayne100% (1)
- Chapter1 Introduction To GrindingDocument5 pagesChapter1 Introduction To GrindingSwati GautamNo ratings yet
- 2.1 Allergic Medicamentosus Stomatitis: History of Present IllnessDocument13 pages2.1 Allergic Medicamentosus Stomatitis: History of Present IllnessIrma NovitasariNo ratings yet
- Ulcerative Lesions of The Oral Mucosa: Yu Zhou, Xiaoying Li, Xin Jin, and Qianming ChenDocument20 pagesUlcerative Lesions of The Oral Mucosa: Yu Zhou, Xiaoying Li, Xin Jin, and Qianming ChenIrma NovitasariNo ratings yet
- LK - Alergi 1Document8 pagesLK - Alergi 1DewiSartikaNo ratings yet
- Crusted (Norwegian) Scabies Following Systemic and Topical Corticosteroid TherapyDocument4 pagesCrusted (Norwegian) Scabies Following Systemic and Topical Corticosteroid TherapysfiahyusnitaNo ratings yet
- General Surgery SEQDocument15 pagesGeneral Surgery SEQFatima Arshad100% (1)
- Sneddon-Wilkinson Disease Treated With Etanercept: Report of Two CasesDocument5 pagesSneddon-Wilkinson Disease Treated With Etanercept: Report of Two CasesLewishoppusNo ratings yet
- Case 50 Oral Lichen Planus (Non-Erosive Type)Document19 pagesCase 50 Oral Lichen Planus (Non-Erosive Type)Irma NovitasariNo ratings yet
- Oral Lichen Planus: A Case SeriesDocument4 pagesOral Lichen Planus: A Case SeriesFebri YolandaNo ratings yet
- Oral Lichen Planus: A Case SeriesDocument4 pagesOral Lichen Planus: A Case SeriesRisa SasmitaNo ratings yet
- Jurnal PruritusDocument4 pagesJurnal Pruritusdvunsrat agt2021No ratings yet
- Acute Parapharyngeal Abscess Secondary To Streptococcal MastoiditisDocument2 pagesAcute Parapharyngeal Abscess Secondary To Streptococcal Mastoiditiswawansiswadi01No ratings yet
- Acad Dermatol Venereol - 2019 - Nowak - Rosacea Fulminans Coincidence of The Disease With Inflammatory Bowel DiseaseDocument2 pagesAcad Dermatol Venereol - 2019 - Nowak - Rosacea Fulminans Coincidence of The Disease With Inflammatory Bowel DiseasecamilabettiomatosNo ratings yet
- Case Report Benign Mucosal Membrane Pemphigoid As A Differential Diagnosis of Necrotizing Periodontal DiseaseDocument4 pagesCase Report Benign Mucosal Membrane Pemphigoid As A Differential Diagnosis of Necrotizing Periodontal DiseaseYeni PuspitasariNo ratings yet
- 2024-Article Text-6560-1-10-20230128Document4 pages2024-Article Text-6560-1-10-20230128Adniana NareswariNo ratings yet
- A Case of Pemphigus Vulgaris Associated With Ulcerative ColitisDocument4 pagesA Case of Pemphigus Vulgaris Associated With Ulcerative ColitisfakhmiyogiiNo ratings yet
- Case Report: Subcorneal Pustular Dermatosis in Childhood: A Case Report and Review of The LiteratureDocument6 pagesCase Report: Subcorneal Pustular Dermatosis in Childhood: A Case Report and Review of The LiteratureIrsalinaHusnaAzwirNo ratings yet
- 86 90 Case Report - Leishmaniasis - Audi - PDF 86 90 PDFDocument5 pages86 90 Case Report - Leishmaniasis - Audi - PDF 86 90 PDFJeddhie MoraNo ratings yet
- Disseminated Tinea Incognita in A Patient With Ichthyosis Vulgaris and EczemaDocument3 pagesDisseminated Tinea Incognita in A Patient With Ichthyosis Vulgaris and EczemaNovia KurniantiNo ratings yet
- Atypical Manifestations of Tinea Corporis: Case ReportsDocument5 pagesAtypical Manifestations of Tinea Corporis: Case ReportsMuhammad HafizuddinNo ratings yet
- Brar (2007) - NS Resemples Lymphoreticular ProcessDocument2 pagesBrar (2007) - NS Resemples Lymphoreticular ProcessIlma ArifaniNo ratings yet
- Nicotine-Induced Bullous Fixed Drug EruptionDocument3 pagesNicotine-Induced Bullous Fixed Drug Eruptionamal amanahNo ratings yet
- BDJ Paper On DentalDocument5 pagesBDJ Paper On DentalZihao WuNo ratings yet
- Acne Conglobata 1Document4 pagesAcne Conglobata 1Ridho ForesNo ratings yet
- Chin Dermatitis in A Cat 8656 ArticleDocument3 pagesChin Dermatitis in A Cat 8656 Articleeleanorcyoung01No ratings yet
- Acute Submandibular Sialadenitis-A Case ReportDocument4 pagesAcute Submandibular Sialadenitis-A Case ReportsurgaNo ratings yet
- Antibiotics CasesDocument39 pagesAntibiotics CasesnistaneNo ratings yet
- نم) corrected 4 marchDocument67 pagesنم) corrected 4 marchAfaf MagedNo ratings yet
- McAlinden Hordeolum PDFDocument3 pagesMcAlinden Hordeolum PDFNur Rakhma AkmaliaNo ratings yet
- BCR 2019 233946Document2 pagesBCR 2019 233946Paola AlcocerNo ratings yet
- Short Communication: Granuloma Faciale Treated Successfully With ColchicineDocument2 pagesShort Communication: Granuloma Faciale Treated Successfully With ColchicinePratama Imanuel RawungNo ratings yet
- 1 DapusDocument4 pages1 DapusLidwina ApyakaNo ratings yet
- Ciclosporin Therapy For Canine Generalized Discoid LupusDocument6 pagesCiclosporin Therapy For Canine Generalized Discoid LupusPatrícia StancuNo ratings yet
- 2007 - Exfoliative Cheilitis A Case ReportDocument5 pages2007 - Exfoliative Cheilitis A Case ReportramaNo ratings yet
- SurgeryDocument8 pagesSurgeryChat GptNo ratings yet
- Sljod v8 p28 29Document2 pagesSljod v8 p28 29Bhagya HettiarachchiNo ratings yet
- Sub Epidermal Blister Formation. Immunofluorescence Reveals Iga Present Within Dermal PapillaeDocument6 pagesSub Epidermal Blister Formation. Immunofluorescence Reveals Iga Present Within Dermal PapillaeRabia RabiaNo ratings yet
- Neutrophilic Sebaceous Adenitis A Challenger Diagnosis With Favorable Response To Dapsone Contribution of Two News CasesDocument6 pagesNeutrophilic Sebaceous Adenitis A Challenger Diagnosis With Favorable Response To Dapsone Contribution of Two News CasesAthenaeum Scientific PublishersNo ratings yet
- Subepidermal Blistering DisorderDocument5 pagesSubepidermal Blistering Disordershanellebandasan17No ratings yet
- Nejmcpc 2107352Document11 pagesNejmcpc 2107352Fábio MenesesNo ratings yet
- CorneaDocument9 pagesCorneafikerteadelleNo ratings yet
- Darier-White Disease: A Rare Genetic DisorderDocument4 pagesDarier-White Disease: A Rare Genetic Disorderanis utamiNo ratings yet
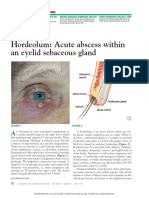
- Hordeolum: Acute Abscess Within An Eyelid Sebaceous Gland: The Clinical PictureDocument3 pagesHordeolum: Acute Abscess Within An Eyelid Sebaceous Gland: The Clinical PictureCamNo ratings yet
- A Case Report On Steroid Induced Acneiform EruptionsDocument3 pagesA Case Report On Steroid Induced Acneiform EruptionsVidini Kusuma AjiNo ratings yet
- Pi Is 2352512617301704Document3 pagesPi Is 2352512617301704qwerty qwerNo ratings yet
- Endo Assignment: Q1 / Write About Weeping CanalsDocument3 pagesEndo Assignment: Q1 / Write About Weeping Canalsعبد الرحمن خالد الزميليNo ratings yet
- V 7 Aop 199Document4 pagesV 7 Aop 199stilahun651No ratings yet
- CC Silva - Rationalization 2022Document35 pagesCC Silva - Rationalization 2022Nicole Xyza JunsayNo ratings yet
- 1028 1782 1 SMDocument4 pages1028 1782 1 SMYeni PuspitasariNo ratings yet
- PASSMEDICINE MCQs-DERMATOLOGYDocument97 pagesPASSMEDICINE MCQs-DERMATOLOGYZohaib AliNo ratings yet
- Herpes Simplex Keratitis: Chief Complaint: History of Present IllnessDocument13 pagesHerpes Simplex Keratitis: Chief Complaint: History of Present IllnessArmando HalauwetNo ratings yet
- Oral Bullous Lichen Planus: Case Report and Review of ManagementDocument5 pagesOral Bullous Lichen Planus: Case Report and Review of ManagementIntan Desi PramitasariNo ratings yet
- 1 FixDocument4 pages1 FixSafa MarwaNo ratings yet
- Aodmr Mishra G Et AlDocument4 pagesAodmr Mishra G Et AlMugdha FrancisNo ratings yet
- Angular Cheilitis YS 3casesDocument6 pagesAngular Cheilitis YS 3casesAngga RanggaNo ratings yet
- 300 DR Anas MCQsDocument235 pages300 DR Anas MCQsmohiNo ratings yet
- Oral Tuberculosis: Case ReportDocument2 pagesOral Tuberculosis: Case ReportMauriceNo ratings yet
- Transient Eosinophilic Nodulomatosis A Report of Two CasesDocument6 pagesTransient Eosinophilic Nodulomatosis A Report of Two CasesAthenaeum Scientific PublishersNo ratings yet
- 1 s2.0 S1027811716300349 MainDocument4 pages1 s2.0 S1027811716300349 Mainbenjieescol86No ratings yet
- BiodataDocument11 pagesBiodatabentubz100% (2)
- Skin Lichen Planus, A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsFrom EverandSkin Lichen Planus, A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsNo ratings yet
- Microbial Production of Scleroglucan and DSPDocument19 pagesMicrobial Production of Scleroglucan and DSPgandurikNo ratings yet
- SF4 - For Love of ChaosDocument24 pagesSF4 - For Love of ChaosNicolai Govoni100% (2)
- Car Modifications - Stage 1, 2 & 3 - TeambhpDocument7 pagesCar Modifications - Stage 1, 2 & 3 - TeambhpMuralidhar0% (1)
- Joint Hearing, 113TH Congress - Addendum To July 26, 2013, Hearing: Does Road Pricing Affect Port Freight Activity: Recent Evidence From The Port of New York and New JerseyDocument25 pagesJoint Hearing, 113TH Congress - Addendum To July 26, 2013, Hearing: Does Road Pricing Affect Port Freight Activity: Recent Evidence From The Port of New York and New JerseyScribd Government DocsNo ratings yet
- Trilogy IT Acetabular System Design Rationale 06.01853.Document14 pagesTrilogy IT Acetabular System Design Rationale 06.01853.CARLOS ENRIQUE ALVAREZ ALFARONo ratings yet
- The Adventurer's Guide To Abusing Monsters PDFDocument41 pagesThe Adventurer's Guide To Abusing Monsters PDFAnonymous 9lC4ZLNo ratings yet
- Mode of Action of ToxicantsDocument12 pagesMode of Action of Toxicantssneha rameshNo ratings yet
- JPC 119022Document2 pagesJPC 119022Juan Pablo EspinosaNo ratings yet
- Answer All Questions. Each Question Is Followed by Four Options, A, B, C and D. For Each Question, Choose One Answer OnlyDocument7 pagesAnswer All Questions. Each Question Is Followed by Four Options, A, B, C and D. For Each Question, Choose One Answer Onlyharshana rajagopalNo ratings yet
- 2130o1921s1d81e1Document26 pages2130o1921s1d81e1Balraj MyakaNo ratings yet
- Biofuels Annual - Kuala Lumpur - Malaysia - MY2022-0008Document15 pagesBiofuels Annual - Kuala Lumpur - Malaysia - MY2022-0008magijNo ratings yet
- Sony Playstation 3 Cecha00 Cecha01 Sm-Ps3-0013e-02Document45 pagesSony Playstation 3 Cecha00 Cecha01 Sm-Ps3-0013e-02naoyakatsu100% (2)
- Intervention ExamDocument10 pagesIntervention ExamGiNo ratings yet
- Passage 1: Mukesh AmbaniDocument4 pagesPassage 1: Mukesh AmbaniThảo VyNo ratings yet
- PipeWeldingHandbook PDFDocument32 pagesPipeWeldingHandbook PDFSid BouhaNo ratings yet
- Fractional Calculus Author(s) : Bertram Ross Source: Mathematics Magazine, Vol. 50, No. 3 (May, 1977), Pp. 115-122 Published By: Stable URL: Accessed: 02/12/2010 23:54Document9 pagesFractional Calculus Author(s) : Bertram Ross Source: Mathematics Magazine, Vol. 50, No. 3 (May, 1977), Pp. 115-122 Published By: Stable URL: Accessed: 02/12/2010 23:54sathish256No ratings yet
- GD Gdpmds Draft1Document24 pagesGD Gdpmds Draft1Syaiful NazwanNo ratings yet
- Camera Calibration in A FlashDocument11 pagesCamera Calibration in A FlashM_D_MendisNo ratings yet
- Numismatic News March 01 2022Document98 pagesNumismatic News March 01 2022Rick Wilson100% (1)
- Operation Guide EL-531V R S PDFDocument30 pagesOperation Guide EL-531V R S PDFlotannaNo ratings yet
- 1365-1370-Oucip905 Ijetsr PDFDocument6 pages1365-1370-Oucip905 Ijetsr PDFYash AgrawalNo ratings yet
- Data Sheet ST ESTABILIZADORDocument3 pagesData Sheet ST ESTABILIZADORJuan Antonio Barco MorenoNo ratings yet
- Seminarul 8Document38 pagesSeminarul 8Alexandra GeantaNo ratings yet
- American MFG Axg FG Axg Parts BookDocument19 pagesAmerican MFG Axg FG Axg Parts BookmarkNo ratings yet
- Chemical Equilibria of Aqueous Solutions: Che 401: Analytical ChemistryDocument31 pagesChemical Equilibria of Aqueous Solutions: Che 401: Analytical ChemistryScrappy WellNo ratings yet
























































































Download as pdf or txt
You might also like
- Side Lifter Shop Manual SteelbroDocument743 pagesSide Lifter Shop Manual SteelbroYandier Martínez100% (1)
- Yamaha Owners Manual 40 50 HPDocument88 pagesYamaha Owners Manual 40 50 HPmnbvqwert100% (5)
- Sick VerseDocument503 pagesSick Verselozerface88100% (3)
- 13 Principles of Wiccan BeliefDocument7 pages13 Principles of Wiccan BeliefWayne100% (1)
- Chapter1 Introduction To GrindingDocument5 pagesChapter1 Introduction To GrindingSwati GautamNo ratings yet
- 2.1 Allergic Medicamentosus Stomatitis: History of Present IllnessDocument13 pages2.1 Allergic Medicamentosus Stomatitis: History of Present IllnessIrma NovitasariNo ratings yet
- Ulcerative Lesions of The Oral Mucosa: Yu Zhou, Xiaoying Li, Xin Jin, and Qianming ChenDocument20 pagesUlcerative Lesions of The Oral Mucosa: Yu Zhou, Xiaoying Li, Xin Jin, and Qianming ChenIrma NovitasariNo ratings yet
- LK - Alergi 1Document8 pagesLK - Alergi 1DewiSartikaNo ratings yet
- Crusted (Norwegian) Scabies Following Systemic and Topical Corticosteroid TherapyDocument4 pagesCrusted (Norwegian) Scabies Following Systemic and Topical Corticosteroid TherapysfiahyusnitaNo ratings yet
- General Surgery SEQDocument15 pagesGeneral Surgery SEQFatima Arshad100% (1)
- Sneddon-Wilkinson Disease Treated With Etanercept: Report of Two CasesDocument5 pagesSneddon-Wilkinson Disease Treated With Etanercept: Report of Two CasesLewishoppusNo ratings yet
- Case 50 Oral Lichen Planus (Non-Erosive Type)Document19 pagesCase 50 Oral Lichen Planus (Non-Erosive Type)Irma NovitasariNo ratings yet
- Oral Lichen Planus: A Case SeriesDocument4 pagesOral Lichen Planus: A Case SeriesFebri YolandaNo ratings yet
- Oral Lichen Planus: A Case SeriesDocument4 pagesOral Lichen Planus: A Case SeriesRisa SasmitaNo ratings yet
- Jurnal PruritusDocument4 pagesJurnal Pruritusdvunsrat agt2021No ratings yet
- Acute Parapharyngeal Abscess Secondary To Streptococcal MastoiditisDocument2 pagesAcute Parapharyngeal Abscess Secondary To Streptococcal Mastoiditiswawansiswadi01No ratings yet
- Acad Dermatol Venereol - 2019 - Nowak - Rosacea Fulminans Coincidence of The Disease With Inflammatory Bowel DiseaseDocument2 pagesAcad Dermatol Venereol - 2019 - Nowak - Rosacea Fulminans Coincidence of The Disease With Inflammatory Bowel DiseasecamilabettiomatosNo ratings yet
- Case Report Benign Mucosal Membrane Pemphigoid As A Differential Diagnosis of Necrotizing Periodontal DiseaseDocument4 pagesCase Report Benign Mucosal Membrane Pemphigoid As A Differential Diagnosis of Necrotizing Periodontal DiseaseYeni PuspitasariNo ratings yet
- 2024-Article Text-6560-1-10-20230128Document4 pages2024-Article Text-6560-1-10-20230128Adniana NareswariNo ratings yet
- A Case of Pemphigus Vulgaris Associated With Ulcerative ColitisDocument4 pagesA Case of Pemphigus Vulgaris Associated With Ulcerative ColitisfakhmiyogiiNo ratings yet
- Case Report: Subcorneal Pustular Dermatosis in Childhood: A Case Report and Review of The LiteratureDocument6 pagesCase Report: Subcorneal Pustular Dermatosis in Childhood: A Case Report and Review of The LiteratureIrsalinaHusnaAzwirNo ratings yet
- 86 90 Case Report - Leishmaniasis - Audi - PDF 86 90 PDFDocument5 pages86 90 Case Report - Leishmaniasis - Audi - PDF 86 90 PDFJeddhie MoraNo ratings yet
- Disseminated Tinea Incognita in A Patient With Ichthyosis Vulgaris and EczemaDocument3 pagesDisseminated Tinea Incognita in A Patient With Ichthyosis Vulgaris and EczemaNovia KurniantiNo ratings yet
- Atypical Manifestations of Tinea Corporis: Case ReportsDocument5 pagesAtypical Manifestations of Tinea Corporis: Case ReportsMuhammad HafizuddinNo ratings yet
- Brar (2007) - NS Resemples Lymphoreticular ProcessDocument2 pagesBrar (2007) - NS Resemples Lymphoreticular ProcessIlma ArifaniNo ratings yet
- Nicotine-Induced Bullous Fixed Drug EruptionDocument3 pagesNicotine-Induced Bullous Fixed Drug Eruptionamal amanahNo ratings yet
- BDJ Paper On DentalDocument5 pagesBDJ Paper On DentalZihao WuNo ratings yet
- Acne Conglobata 1Document4 pagesAcne Conglobata 1Ridho ForesNo ratings yet
- Chin Dermatitis in A Cat 8656 ArticleDocument3 pagesChin Dermatitis in A Cat 8656 Articleeleanorcyoung01No ratings yet
- Acute Submandibular Sialadenitis-A Case ReportDocument4 pagesAcute Submandibular Sialadenitis-A Case ReportsurgaNo ratings yet
- Antibiotics CasesDocument39 pagesAntibiotics CasesnistaneNo ratings yet
- نم) corrected 4 marchDocument67 pagesنم) corrected 4 marchAfaf MagedNo ratings yet
- McAlinden Hordeolum PDFDocument3 pagesMcAlinden Hordeolum PDFNur Rakhma AkmaliaNo ratings yet
- BCR 2019 233946Document2 pagesBCR 2019 233946Paola AlcocerNo ratings yet
- Short Communication: Granuloma Faciale Treated Successfully With ColchicineDocument2 pagesShort Communication: Granuloma Faciale Treated Successfully With ColchicinePratama Imanuel RawungNo ratings yet
- 1 DapusDocument4 pages1 DapusLidwina ApyakaNo ratings yet
- Ciclosporin Therapy For Canine Generalized Discoid LupusDocument6 pagesCiclosporin Therapy For Canine Generalized Discoid LupusPatrícia StancuNo ratings yet
- 2007 - Exfoliative Cheilitis A Case ReportDocument5 pages2007 - Exfoliative Cheilitis A Case ReportramaNo ratings yet
- SurgeryDocument8 pagesSurgeryChat GptNo ratings yet
- Sljod v8 p28 29Document2 pagesSljod v8 p28 29Bhagya HettiarachchiNo ratings yet
- Sub Epidermal Blister Formation. Immunofluorescence Reveals Iga Present Within Dermal PapillaeDocument6 pagesSub Epidermal Blister Formation. Immunofluorescence Reveals Iga Present Within Dermal PapillaeRabia RabiaNo ratings yet
- Neutrophilic Sebaceous Adenitis A Challenger Diagnosis With Favorable Response To Dapsone Contribution of Two News CasesDocument6 pagesNeutrophilic Sebaceous Adenitis A Challenger Diagnosis With Favorable Response To Dapsone Contribution of Two News CasesAthenaeum Scientific PublishersNo ratings yet
- Subepidermal Blistering DisorderDocument5 pagesSubepidermal Blistering Disordershanellebandasan17No ratings yet
- Nejmcpc 2107352Document11 pagesNejmcpc 2107352Fábio MenesesNo ratings yet
- CorneaDocument9 pagesCorneafikerteadelleNo ratings yet
- Darier-White Disease: A Rare Genetic DisorderDocument4 pagesDarier-White Disease: A Rare Genetic Disorderanis utamiNo ratings yet
- Hordeolum: Acute Abscess Within An Eyelid Sebaceous Gland: The Clinical PictureDocument3 pagesHordeolum: Acute Abscess Within An Eyelid Sebaceous Gland: The Clinical PictureCamNo ratings yet
- A Case Report On Steroid Induced Acneiform EruptionsDocument3 pagesA Case Report On Steroid Induced Acneiform EruptionsVidini Kusuma AjiNo ratings yet
- Pi Is 2352512617301704Document3 pagesPi Is 2352512617301704qwerty qwerNo ratings yet
- Endo Assignment: Q1 / Write About Weeping CanalsDocument3 pagesEndo Assignment: Q1 / Write About Weeping Canalsعبد الرحمن خالد الزميليNo ratings yet
- V 7 Aop 199Document4 pagesV 7 Aop 199stilahun651No ratings yet
- CC Silva - Rationalization 2022Document35 pagesCC Silva - Rationalization 2022Nicole Xyza JunsayNo ratings yet
- 1028 1782 1 SMDocument4 pages1028 1782 1 SMYeni PuspitasariNo ratings yet
- PASSMEDICINE MCQs-DERMATOLOGYDocument97 pagesPASSMEDICINE MCQs-DERMATOLOGYZohaib AliNo ratings yet
- Herpes Simplex Keratitis: Chief Complaint: History of Present IllnessDocument13 pagesHerpes Simplex Keratitis: Chief Complaint: History of Present IllnessArmando HalauwetNo ratings yet
- Oral Bullous Lichen Planus: Case Report and Review of ManagementDocument5 pagesOral Bullous Lichen Planus: Case Report and Review of ManagementIntan Desi PramitasariNo ratings yet
- 1 FixDocument4 pages1 FixSafa MarwaNo ratings yet
- Aodmr Mishra G Et AlDocument4 pagesAodmr Mishra G Et AlMugdha FrancisNo ratings yet
- Angular Cheilitis YS 3casesDocument6 pagesAngular Cheilitis YS 3casesAngga RanggaNo ratings yet
- 300 DR Anas MCQsDocument235 pages300 DR Anas MCQsmohiNo ratings yet
- Oral Tuberculosis: Case ReportDocument2 pagesOral Tuberculosis: Case ReportMauriceNo ratings yet
- Transient Eosinophilic Nodulomatosis A Report of Two CasesDocument6 pagesTransient Eosinophilic Nodulomatosis A Report of Two CasesAthenaeum Scientific PublishersNo ratings yet
- 1 s2.0 S1027811716300349 MainDocument4 pages1 s2.0 S1027811716300349 Mainbenjieescol86No ratings yet
- BiodataDocument11 pagesBiodatabentubz100% (2)
- Skin Lichen Planus, A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsFrom EverandSkin Lichen Planus, A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsNo ratings yet
- Microbial Production of Scleroglucan and DSPDocument19 pagesMicrobial Production of Scleroglucan and DSPgandurikNo ratings yet
- SF4 - For Love of ChaosDocument24 pagesSF4 - For Love of ChaosNicolai Govoni100% (2)
- Car Modifications - Stage 1, 2 & 3 - TeambhpDocument7 pagesCar Modifications - Stage 1, 2 & 3 - TeambhpMuralidhar0% (1)
- Joint Hearing, 113TH Congress - Addendum To July 26, 2013, Hearing: Does Road Pricing Affect Port Freight Activity: Recent Evidence From The Port of New York and New JerseyDocument25 pagesJoint Hearing, 113TH Congress - Addendum To July 26, 2013, Hearing: Does Road Pricing Affect Port Freight Activity: Recent Evidence From The Port of New York and New JerseyScribd Government DocsNo ratings yet
- Trilogy IT Acetabular System Design Rationale 06.01853.Document14 pagesTrilogy IT Acetabular System Design Rationale 06.01853.CARLOS ENRIQUE ALVAREZ ALFARONo ratings yet
- The Adventurer's Guide To Abusing Monsters PDFDocument41 pagesThe Adventurer's Guide To Abusing Monsters PDFAnonymous 9lC4ZLNo ratings yet
- Mode of Action of ToxicantsDocument12 pagesMode of Action of Toxicantssneha rameshNo ratings yet
- JPC 119022Document2 pagesJPC 119022Juan Pablo EspinosaNo ratings yet
- Answer All Questions. Each Question Is Followed by Four Options, A, B, C and D. For Each Question, Choose One Answer OnlyDocument7 pagesAnswer All Questions. Each Question Is Followed by Four Options, A, B, C and D. For Each Question, Choose One Answer Onlyharshana rajagopalNo ratings yet
- 2130o1921s1d81e1Document26 pages2130o1921s1d81e1Balraj MyakaNo ratings yet
- Biofuels Annual - Kuala Lumpur - Malaysia - MY2022-0008Document15 pagesBiofuels Annual - Kuala Lumpur - Malaysia - MY2022-0008magijNo ratings yet
- Sony Playstation 3 Cecha00 Cecha01 Sm-Ps3-0013e-02Document45 pagesSony Playstation 3 Cecha00 Cecha01 Sm-Ps3-0013e-02naoyakatsu100% (2)
- Intervention ExamDocument10 pagesIntervention ExamGiNo ratings yet
- Passage 1: Mukesh AmbaniDocument4 pagesPassage 1: Mukesh AmbaniThảo VyNo ratings yet
- PipeWeldingHandbook PDFDocument32 pagesPipeWeldingHandbook PDFSid BouhaNo ratings yet
- Fractional Calculus Author(s) : Bertram Ross Source: Mathematics Magazine, Vol. 50, No. 3 (May, 1977), Pp. 115-122 Published By: Stable URL: Accessed: 02/12/2010 23:54Document9 pagesFractional Calculus Author(s) : Bertram Ross Source: Mathematics Magazine, Vol. 50, No. 3 (May, 1977), Pp. 115-122 Published By: Stable URL: Accessed: 02/12/2010 23:54sathish256No ratings yet
- GD Gdpmds Draft1Document24 pagesGD Gdpmds Draft1Syaiful NazwanNo ratings yet
- Camera Calibration in A FlashDocument11 pagesCamera Calibration in A FlashM_D_MendisNo ratings yet
- Numismatic News March 01 2022Document98 pagesNumismatic News March 01 2022Rick Wilson100% (1)
- Operation Guide EL-531V R S PDFDocument30 pagesOperation Guide EL-531V R S PDFlotannaNo ratings yet
- 1365-1370-Oucip905 Ijetsr PDFDocument6 pages1365-1370-Oucip905 Ijetsr PDFYash AgrawalNo ratings yet
- Data Sheet ST ESTABILIZADORDocument3 pagesData Sheet ST ESTABILIZADORJuan Antonio Barco MorenoNo ratings yet
- Seminarul 8Document38 pagesSeminarul 8Alexandra GeantaNo ratings yet
- American MFG Axg FG Axg Parts BookDocument19 pagesAmerican MFG Axg FG Axg Parts BookmarkNo ratings yet
- Chemical Equilibria of Aqueous Solutions: Che 401: Analytical ChemistryDocument31 pagesChemical Equilibria of Aqueous Solutions: Che 401: Analytical ChemistryScrappy WellNo ratings yet