Download as pdf or txt
You might also like
- Oral Radiology Principles and Interpretation 7th Ed PDFDocument14 pagesOral Radiology Principles and Interpretation 7th Ed PDFLaura Victoria Alvarez RodriguezNo ratings yet
- Gateway B2 Test 6B 1-3 PDFDocument3 pagesGateway B2 Test 6B 1-3 PDFlourdes67% (3)
- Dawes, A., Keogh, R. Andrillon, T. y Pearson, J. (2020) A Cognitive Profile of Multi-Sensory Imagery, Memory and Dreaming in AphantasiaDocument10 pagesDawes, A., Keogh, R. Andrillon, T. y Pearson, J. (2020) A Cognitive Profile of Multi-Sensory Imagery, Memory and Dreaming in AphantasiaSAMUEL SALAZAR MURILLONo ratings yet
- 3 - Advances in The Diagnosis and Treatment of VasculitisDocument378 pages3 - Advances in The Diagnosis and Treatment of VasculitisAnonymous nGhxGKWXJr100% (1)
- Leukemia ReportDocument5 pagesLeukemia ReportCrisantaCasliNo ratings yet
- Art InglesDocument8 pagesArt Inglesjereyoli360No ratings yet
- Neuroxpsychological Assessment of Psychogeriatric Patients With Limited EducationDocument11 pagesNeuroxpsychological Assessment of Psychogeriatric Patients With Limited Educationmacarena.isebNo ratings yet
- Systematic Review and Meta-Analysis of Performance of Wearable Arti Ficial Intelligence in Detecting and Predicting DepressionDocument16 pagesSystematic Review and Meta-Analysis of Performance of Wearable Arti Ficial Intelligence in Detecting and Predicting DepressionAmith PrasanthNo ratings yet
- Alz Dem Diag Ass Dis Mo - 2020 - Allegri - Prognostic Value of ATN Alzheimer Biomarkers 60 Month Follow Up ResultsDocument8 pagesAlz Dem Diag Ass Dis Mo - 2020 - Allegri - Prognostic Value of ATN Alzheimer Biomarkers 60 Month Follow Up Resultsk6fqcwfczfNo ratings yet
- 3Document10 pages3Gianfranco Isaac Chapilliquen NavarroNo ratings yet
- Home Core DementiaDocument10 pagesHome Core Dementiazainab.21216No ratings yet
- A Real-Time FMRI Neurofeedback System For The Clinical Alleviation of Depression With A Subject-Independent Classification of Brain States A Proof of Principle StudyDocument12 pagesA Real-Time FMRI Neurofeedback System For The Clinical Alleviation of Depression With A Subject-Independent Classification of Brain States A Proof of Principle Studysiowan wongNo ratings yet
- Comparison of The Greek Version of The Quick Mild Cognitive Impairment Screen and Standardised Mini-Mental State ExaminationDocument9 pagesComparison of The Greek Version of The Quick Mild Cognitive Impairment Screen and Standardised Mini-Mental State Examinationmakis000No ratings yet
- Alves, 2022 - AQ Norms BrazilDocument5 pagesAlves, 2022 - AQ Norms BrazilKathleen LimaNo ratings yet
- Human Brain Mapping - 2020 - TaylorDocument13 pagesHuman Brain Mapping - 2020 - TaylorRana RamizNo ratings yet
- Cog Prob en Pac CN DepreDocument8 pagesCog Prob en Pac CN Deprethiagocasetta11No ratings yet
- Cognitive Discernible Factors Between Schizophrenia and Schizoavective DisorderDocument4 pagesCognitive Discernible Factors Between Schizophrenia and Schizoavective DisorderdarkarotNo ratings yet
- Fnins 17 1301214Document19 pagesFnins 17 1301214guischmoNo ratings yet
- Guia Demencia DCLDocument10 pagesGuia Demencia DCLmaricellap31No ratings yet
- Neuroshield BrochureDocument4 pagesNeuroshield Brochuresaketrocks10No ratings yet
- 2022 - Porcaro - Diagnostic Developments in Differentiating Unresponsive Wakefulness Syndrome and The Minimally Conscious StateDocument20 pages2022 - Porcaro - Diagnostic Developments in Differentiating Unresponsive Wakefulness Syndrome and The Minimally Conscious Statediasgs.beatrizNo ratings yet
- Neuropsychological Profile of Alzheimer's Disease Based On Amyloid Biomarker Findings Results From A South American CohortDocument8 pagesNeuropsychological Profile of Alzheimer's Disease Based On Amyloid Biomarker Findings Results From A South American CohortFlorencia CuñaNo ratings yet
- 4Document13 pages4Gianfranco Isaac Chapilliquen NavarroNo ratings yet
- 4Document13 pages4Gianfranco Isaac Chapilliquen NavarroNo ratings yet
- Zucchella Et Al. (2018)Document12 pagesZucchella Et Al. (2018)CagolindaNo ratings yet
- 2014 - Lees R. Et Al - Test Accuracy of Cognitive Screening Tests For Diagnosis of Dementia and Cognitive Impairment in StrokeDocument11 pages2014 - Lees R. Et Al - Test Accuracy of Cognitive Screening Tests For Diagnosis of Dementia and Cognitive Impairment in Strokerichard LemieuxNo ratings yet
- Decisional Capacity To Consent To Treatment and Research in Patients Affected by Mild Cognitive Impairment A Systematic Review and Meta AnalysisDocument14 pagesDecisional Capacity To Consent To Treatment and Research in Patients Affected by Mild Cognitive Impairment A Systematic Review and Meta AnalysisJulio DelgadoNo ratings yet
- Neurological Exam of Critically-Ill PatientDocument12 pagesNeurological Exam of Critically-Ill PatientSimply SamNo ratings yet
- Neuropsychological Rehabilitation: An International JournalDocument20 pagesNeuropsychological Rehabilitation: An International JournalRodrigoNo ratings yet
- Anatomical Brain Images Alone Can Accurately Diagnose Chronic Neuropsychiatric IllnessesDocument21 pagesAnatomical Brain Images Alone Can Accurately Diagnose Chronic Neuropsychiatric IllnessesAsadNo ratings yet
- Instrumental Activities of Daily Living Scale ForDocument15 pagesInstrumental Activities of Daily Living Scale ForASHLY FIORELLA ALEJANDRA ORTIZ PINEDONo ratings yet
- S0016510721013213Document2 pagesS0016510721013213cifha rajesh saldanhaNo ratings yet
- Migraine Classificatio by Machine Learning With Functional Near-Infrared Spectroscopy During The Mental Arithmetic TaskDocument9 pagesMigraine Classificatio by Machine Learning With Functional Near-Infrared Spectroscopy During The Mental Arithmetic TaskIgnacio Godoy FloresNo ratings yet
- Medical ImaginigDocument362 pagesMedical ImaginigGrethi ChiriacNo ratings yet
- Validation of The Argentine Version of The Montreal Cognitive Assessment Test (MOCA)Document8 pagesValidation of The Argentine Version of The Montreal Cognitive Assessment Test (MOCA)msaponaro6ࢮNo ratings yet
- Articuloq 1Document3 pagesArticuloq 1AlejandroNo ratings yet
- Abstracts / Journal of The Neurological Sciences 455 (2023) 121173 94Document2 pagesAbstracts / Journal of The Neurological Sciences 455 (2023) 121173 94Amin AminiNo ratings yet
- The Successful Discrimination of Depression From EEG Could Be Attributed To Proper Feature Extraction and Not To A Particular Classification MethodDocument13 pagesThe Successful Discrimination of Depression From EEG Could Be Attributed To Proper Feature Extraction and Not To A Particular Classification Methodforooz davoodzadehNo ratings yet
- Makalah Jurnal Sensitivity and SpecificitypdfDocument22 pagesMakalah Jurnal Sensitivity and SpecificitypdfKiki Celiana TiffanyNo ratings yet
- Olfaction in Autism Spectrum Disorders: A Systematic Review: Child NeuropsychologyDocument26 pagesOlfaction in Autism Spectrum Disorders: A Systematic Review: Child NeuropsychologySimone LanucaraNo ratings yet
- Ace-R CHDocument15 pagesAce-R CHPsi Mario FloresNo ratings yet
- S. Deutsch Et Al. Autism Spectrum Disorders PDFDocument210 pagesS. Deutsch Et Al. Autism Spectrum Disorders PDFrominchiNo ratings yet
- Journal of Clinical and Experimental Neuropsychology: Merve Çebi, Gülsen Babacan, Öget Öktem Tanör & Hakan GürvitDocument10 pagesJournal of Clinical and Experimental Neuropsychology: Merve Çebi, Gülsen Babacan, Öget Öktem Tanör & Hakan GürvitDR RISKA WAHYUNo ratings yet
- Vladimir - Belov, Doctoral ThesisDocument189 pagesVladimir - Belov, Doctoral ThesisMA MANo ratings yet
- 2015 Book TranslationalApproachesToAutis PDFDocument222 pages2015 Book TranslationalApproachesToAutis PDFCarolina Falcon100% (1)
- Ayuda Al Diagnóstico Del Trastorno de Identidad Disociativo Estudio de Reconocimiento de Patrones de Biomarcadores CerebralesDocument9 pagesAyuda Al Diagnóstico Del Trastorno de Identidad Disociativo Estudio de Reconocimiento de Patrones de Biomarcadores CerebralesValentina RodriguezNo ratings yet
- Falgàs 2019 - Comparison Between Visual and Quantitative Hippocampal Atrophy AssessmentDocument7 pagesFalgàs 2019 - Comparison Between Visual and Quantitative Hippocampal Atrophy AssessmentljdNo ratings yet
- Journal Reading Delirium and DementiaDocument31 pagesJournal Reading Delirium and DementiaIrvin MarcelNo ratings yet
- Ibanez 2014Document20 pagesIbanez 2014LUIS FELIPE CHAGAS CALDEIRA CATAONo ratings yet
- Convolutional Neural Network For Automated FLAIR Lesion Segmentation On Clinical Brain MR ImagingDocument9 pagesConvolutional Neural Network For Automated FLAIR Lesion Segmentation On Clinical Brain MR ImagingTigabu YayaNo ratings yet
- Ntal AtropDocument13 pagesNtal Atrop326449No ratings yet
- Neurodevelopmental Disorders in Children With Severe To Profound Sensorineural Hearing Loss: A Clinical StudyDocument7 pagesNeurodevelopmental Disorders in Children With Severe To Profound Sensorineural Hearing Loss: A Clinical StudySoporte CeffanNo ratings yet
- Santangelo2014 Article ApathyInUntreatedDeNovoPatientDocument10 pagesSantangelo2014 Article ApathyInUntreatedDeNovoPatientketevanNo ratings yet
- Optimistic Stratagems of Machine Based Deep LearningDocument8 pagesOptimistic Stratagems of Machine Based Deep LearningHerald Scholarly Open AccessNo ratings yet
- Neuropsychological Testing PDFDocument27 pagesNeuropsychological Testing PDFHelping OthersNo ratings yet
- ARTÍCULODocument7 pagesARTÍCULOPablo GuillénNo ratings yet
- Fpsyt 11 599099Document7 pagesFpsyt 11 599099Maritsa EngelbrechtNo ratings yet
- The Functional AbilityDocument9 pagesThe Functional AbilityCristina MPNo ratings yet
- Differentiated Performance TaskDocument1 pageDifferentiated Performance TaskCLester MadShadowNo ratings yet
- Evaluation of Cognitive Impairment in Older AdultsDocument7 pagesEvaluation of Cognitive Impairment in Older AdultsnativaoneNo ratings yet
- Changing Everyday Memory Bahaviour in Amnestic Mild Cognitive Impairment TROYERDocument25 pagesChanging Everyday Memory Bahaviour in Amnestic Mild Cognitive Impairment TROYERRegistro psiNo ratings yet
- Toward A Neurocircuit-Based Taxonomy To Guide Treatment of Obsessive - Compulsive DisorderDocument22 pagesToward A Neurocircuit-Based Taxonomy To Guide Treatment of Obsessive - Compulsive DisorderemmanuelNo ratings yet
- Neurometabolic Hereditary Diseases of AdultsFrom EverandNeurometabolic Hereditary Diseases of AdultsAlessandro P. BurlinaNo ratings yet
- KWKSKZBSJNZDocument20 pagesKWKSKZBSJNZYuffaa Ainayyaa0% (1)
- Research Proposal First Draft (Adamu Moti)Document25 pagesResearch Proposal First Draft (Adamu Moti)ODAA TUBENo ratings yet
- Hydatid DiseaseDocument9 pagesHydatid DiseaseAjinkya GaikwadNo ratings yet
- Surgical Ward JournalDocument6 pagesSurgical Ward JournalMa Genille Samporna SabalNo ratings yet
- 501MCQforclinicalpharmacylast IvrtjnDocument119 pages501MCQforclinicalpharmacylast Ivrtjnد.شەماڵ احمد : پزیشکی دەرمانساز100% (1)
- Nursing Research and Clinical Update Post Test (Responses) - Form Responses 1Document6 pagesNursing Research and Clinical Update Post Test (Responses) - Form Responses 1Indah PermatasariNo ratings yet
- Case Report: Management of Pit Viper Envenoming Without AntivenomDocument3 pagesCase Report: Management of Pit Viper Envenoming Without AntivenomNavin BhattNo ratings yet
- Chapter 5 Crystalline Lens - Abdelmonem Hamed EditionDocument16 pagesChapter 5 Crystalline Lens - Abdelmonem Hamed EditionAbdelmonem HamedNo ratings yet
- Journal of Diabetes and Its Complications: 10.1016/j.jdiacomp.2017.11.001Document43 pagesJournal of Diabetes and Its Complications: 10.1016/j.jdiacomp.2017.11.001ClaudiaHerediaNo ratings yet
- 1AA17AT009 - Trauma Centre by Ananya KulkarniDocument43 pages1AA17AT009 - Trauma Centre by Ananya KulkarniSakshi RangnekarNo ratings yet
- Diabetes InsipidusDocument7 pagesDiabetes Insipiduspaul_stefenson10No ratings yet
- Reviewer 116Document5 pagesReviewer 116Mae Arra Gilbao Lecobu-anNo ratings yet
- Collagen Stimulants in Facial Rejuvenation A Systematic Review - Millar-Hume, 2020Document4 pagesCollagen Stimulants in Facial Rejuvenation A Systematic Review - Millar-Hume, 2020Rafael Autran Cavalcante AraújoNo ratings yet
- Do You Have ADHD or OCD Amen Clinics PDFDocument1 pageDo You Have ADHD or OCD Amen Clinics PDFJessica Therese TranNo ratings yet
- Daftar Penyakit Telinga Hidung Tenggorok-Kepala Leher Menurut Icd 10Document10 pagesDaftar Penyakit Telinga Hidung Tenggorok-Kepala Leher Menurut Icd 10kartianiNo ratings yet
- 50-Year-Old Man Overcomes His Battle With Lung Cancer Using Cannabis Oil, Stuns CBS NewsDocument16 pages50-Year-Old Man Overcomes His Battle With Lung Cancer Using Cannabis Oil, Stuns CBS Newstahirmaqpk100% (1)
- Imitrex: (Sumatriptan) Nasal SprayDocument25 pagesImitrex: (Sumatriptan) Nasal Spray58TRONGNo ratings yet
- Instructions For Novel Coronavirus (2019 nCoV) Nucleic Acid Detection Kit RT PCR) - 20210316 (N, S, ORF1ab Gene)Document2 pagesInstructions For Novel Coronavirus (2019 nCoV) Nucleic Acid Detection Kit RT PCR) - 20210316 (N, S, ORF1ab Gene)nazmiNo ratings yet
- 21-CoV10069-Ruslan Bin HashimDocument1 page21-CoV10069-Ruslan Bin HashimHERU EKO PRAYOGONo ratings yet
- HEALTH K 12 Curriculum GuideDocument47 pagesHEALTH K 12 Curriculum GuideMarcia Cristina A. LopezNo ratings yet
- 26071-JO-HSE-020 Random Alcohol & Drug Test Form Rev1Document1 page26071-JO-HSE-020 Random Alcohol & Drug Test Form Rev1medicdaeah pkg3100% (1)
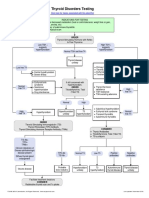
- Thyroid Disorders Testing AlgorithmDocument1 pageThyroid Disorders Testing AlgorithmRezi HelperNo ratings yet
- Bethesda SystemDocument186 pagesBethesda SystemJoyce Pardo FernandezNo ratings yet
- AO Minimally Invasive Plate OsteosynthesisDocument785 pagesAO Minimally Invasive Plate OsteosynthesisDEISYLOPEZ9005100% (1)
- High Intake of Ultra Processed Food Is Associated With Dementia in Adults: A Systematic Review and Meta Analysis of Observational StudiesDocument13 pagesHigh Intake of Ultra Processed Food Is Associated With Dementia in Adults: A Systematic Review and Meta Analysis of Observational Studiesangela.e.sanchezNo ratings yet
- Treatment of Scabies, Comparing The Different Medications: LettersDocument1 pageTreatment of Scabies, Comparing The Different Medications: LettersFi NoNo ratings yet
- Measuring Other Conditions in Oral EpidemiologyDocument7 pagesMeasuring Other Conditions in Oral EpidemiologyAl Azizul HakimNo ratings yet