Download as pdf or txt
You might also like
- DragonologyDocument30 pagesDragonologyEce YilmazNo ratings yet
- Research Methods - Revision Lab, Field and Natural StudiesDocument10 pagesResearch Methods - Revision Lab, Field and Natural StudiesSupriyaa Chordia50% (2)
- Project Report On: COVID19 Testing Management SystemDocument43 pagesProject Report On: COVID19 Testing Management Systemhemalatha ravutlaNo ratings yet
- The Gamma Mindset Technique GuidelinesDocument8 pagesThe Gamma Mindset Technique GuidelinesDeepak Rana100% (1)
- Peter Mueller Sintering Lab ReportDocument25 pagesPeter Mueller Sintering Lab Reportharry potterNo ratings yet
- Lazaroni 16Document4 pagesLazaroni 16adiNo ratings yet
- Congenital Absence of A Part of The Fallopian Tube: A Case ReportDocument3 pagesCongenital Absence of A Part of The Fallopian Tube: A Case ReportHarinder SinghNo ratings yet
- Wood 2018Document10 pagesWood 2018dewaprasatyaNo ratings yet
- Sibs With Anencephaly, Anophthalmia, Clefts, Omphalocele, and Polydactyly: Hydrolethalus orDocument4 pagesSibs With Anencephaly, Anophthalmia, Clefts, Omphalocele, and Polydactyly: Hydrolethalus orSarly FebrianaNo ratings yet
- Journal of Pediatric Surgery Case Reports: Moaied A. Hassan, Hasan K. Gatea, Thura K. Ja'afar, Ahmed O. Fahad TDocument3 pagesJournal of Pediatric Surgery Case Reports: Moaied A. Hassan, Hasan K. Gatea, Thura K. Ja'afar, Ahmed O. Fahad TVero MeidyNo ratings yet
- Parurethral CystsDocument3 pagesParurethral CystsIoannis ValioulisNo ratings yet
- Penis: 2.1 Embryology and Penile DevelopmentDocument27 pagesPenis: 2.1 Embryology and Penile DevelopmenteeNo ratings yet
- CTEV A Review of Current ManagementlDocument6 pagesCTEV A Review of Current Managementlvicky174No ratings yet
- Teunis Sen 2007Document2 pagesTeunis Sen 2007Muhammad IqsanNo ratings yet
- Jurnal MAR 2Document10 pagesJurnal MAR 2Taufik HidayatNo ratings yet
- 2014 Body StalkDocument2 pages2014 Body StalkHelena Ribeiro SouzaNo ratings yet
- Neutering Is Not Associated With Early-Onset Urethral Obstruction in CatsDocument7 pagesNeutering Is Not Associated With Early-Onset Urethral Obstruction in CatsRifia FaniNo ratings yet
- First Trimester Sonographic Diagnosis of Limb-Body Wall Defect Associating Both Cephalic and Thoraco-Abdominal Defects - A Case Report and Literature UpdateDocument3 pagesFirst Trimester Sonographic Diagnosis of Limb-Body Wall Defect Associating Both Cephalic and Thoraco-Abdominal Defects - A Case Report and Literature UpdateIvan DavrayNo ratings yet
- Sample (1) Penis PDFDocument28 pagesSample (1) Penis PDFcristian ionut finaruNo ratings yet
- AdminDocument5 pagesAdminFirman adiNo ratings yet
- Couvelaire Uterus: Manju Rathi, Sunil Kumar Rathi, Manju Purohit, Ashish PathakDocument2 pagesCouvelaire Uterus: Manju Rathi, Sunil Kumar Rathi, Manju Purohit, Ashish PathakMDreamerNo ratings yet
- Accessory Urethra, Accessory PhallusDocument7 pagesAccessory Urethra, Accessory PhallusGunduz AgaNo ratings yet
- Acalvaria: Case ReportDocument3 pagesAcalvaria: Case ReportGabriel Del CastilloNo ratings yet
- Amniotic Band Sequence: Consult SeriesDocument2 pagesAmniotic Band Sequence: Consult SeriesRamos Zavala Julio CesarNo ratings yet
- Pene Palmeado Una Nueva ClasificacionDocument9 pagesPene Palmeado Una Nueva ClasificacionJorgy Ayala PinedaNo ratings yet
- Daftar 1 PDFDocument5 pagesDaftar 1 PDFMaleakhi SinagaNo ratings yet
- AUR in ChildrenDocument1 pageAUR in ChildrenStaporn KasemsripitakNo ratings yet
- Trilogy of Foregut Midgut and Hindgut Atresias PreDocument5 pagesTrilogy of Foregut Midgut and Hindgut Atresias PreEriekafebriayana RNo ratings yet
- TAP 20230090 NLM New InddDocument8 pagesTAP 20230090 NLM New InddYusuf HardiNo ratings yet
- Cleidocraneal Dysplasia 2000Document3 pagesCleidocraneal Dysplasia 2000Daniela Paz Valenzuela ColmenaresNo ratings yet
- Surgical Treatment of Anorectal MalformationsDocument8 pagesSurgical Treatment of Anorectal MalformationsGerii Pucllas VillarNo ratings yet
- Encephalocele Prenatal Diagnosis About A CaseDocument3 pagesEncephalocele Prenatal Diagnosis About A CaseInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- Jurnal 2Document7 pagesJurnal 2citra annisa fitriNo ratings yet
- Body-Stalk Anomaly. A Case Report and Review of The LiteratureDocument5 pagesBody-Stalk Anomaly. A Case Report and Review of The LiteratureadiNo ratings yet
- Bilobed Testicle in Children - Diagnosis and ManagementDocument2 pagesBilobed Testicle in Children - Diagnosis and ManagementJad DegheiliNo ratings yet
- Exceptional Fetal Malformation Acardiac Headless TwinDocument2 pagesExceptional Fetal Malformation Acardiac Headless TwinInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- Hydrocephalus in An American Miniature Horse Foal A Case Report and Review 2011 Journal of Equine Veterinary ScienceDocument4 pagesHydrocephalus in An American Miniature Horse Foal A Case Report and Review 2011 Journal of Equine Veterinary SciencealarochaNo ratings yet
- Symptomatic Bochdalek Hernia in An AdultDocument4 pagesSymptomatic Bochdalek Hernia in An Adultika nur utamiNo ratings yet
- Wright 2011Document3 pagesWright 2011diana.miron.mNo ratings yet
- Arias Stella Reaction 40Document16 pagesArias Stella Reaction 40Febry FirmansyahNo ratings yet
- Genetics of Human Heterotaxias: ReviewDocument9 pagesGenetics of Human Heterotaxias: ReviewJacob Trisusilo SaleanNo ratings yet
- Artigo Gravidez EctópicaDocument2 pagesArtigo Gravidez EctópicaKevin UchoaNo ratings yet
- A Multiparity Woman With Pregnancy of Recurrent Anencephaly A Rare Case ReportDocument2 pagesA Multiparity Woman With Pregnancy of Recurrent Anencephaly A Rare Case ReportInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- Schallert 2019Document7 pagesSchallert 2019Dian Putri NingsihNo ratings yet
- Articulo Rotura PrimigestaDocument3 pagesArticulo Rotura PrimigestaYeitzmarNo ratings yet
- A Case of Body Stalk Anomaly Arising After Invitro Fertilization at 26 Week' GestationDocument3 pagesA Case of Body Stalk Anomaly Arising After Invitro Fertilization at 26 Week' GestationasclepiuspdfsNo ratings yet
- Embryofetoscopy A New Old ToolDocument5 pagesEmbryofetoscopy A New Old ToolMiriam ContiNo ratings yet
- Focseneanu2015 PDFDocument3 pagesFocseneanu2015 PDFAniydaNo ratings yet
- Aphallia Associate Fistula RectouretraDocument3 pagesAphallia Associate Fistula Rectouretraeni nadzhifahNo ratings yet
- S - Cervical Ectopic PregnancyDocument8 pagesS - Cervical Ectopic PregnancyCitra Wahyu Tri UtamiNo ratings yet
- Case Report: A Case of Caudal Regression Syndrome: Walking or Sitting?Document5 pagesCase Report: A Case of Caudal Regression Syndrome: Walking or Sitting?LisnainiMuchlisNo ratings yet
- Screenshot 2021-12-09 at 11.53.30Document8 pagesScreenshot 2021-12-09 at 11.53.30mithaNo ratings yet
- Pre-Eclampsia: Pathophysiology and Clinical Implications: State of The Art ReviewDocument15 pagesPre-Eclampsia: Pathophysiology and Clinical Implications: State of The Art ReviewIriawan Indra PutraNo ratings yet
- Preeclampsia Pathophysiology and Clinical ImplicationsDocument15 pagesPreeclampsia Pathophysiology and Clinical ImplicationsKamva DukadaNo ratings yet
- Amnion Rupture SequenceDocument4 pagesAmnion Rupture SequenceashrafmogyNo ratings yet
- Single Umbilical Artery (SUA) - Prenatal Sonography Diagnosis and Vascular Imaging Features Postnatal Cord: A Case ReportDocument3 pagesSingle Umbilical Artery (SUA) - Prenatal Sonography Diagnosis and Vascular Imaging Features Postnatal Cord: A Case ReportSabhina AnseliaNo ratings yet
- Pre-Eclampsia: Pathophysiology and Clinical Implications: State of The Art ReviewDocument15 pagesPre-Eclampsia: Pathophysiology and Clinical Implications: State of The Art ReviewDwi ZirobeNo ratings yet
- Pelvic Organ Prolapse Quantification System (POP-Q) - A New Era in Pelvic Prolapse StagingDocument7 pagesPelvic Organ Prolapse Quantification System (POP-Q) - A New Era in Pelvic Prolapse StagingAnditha NamiraNo ratings yet
- Appendix DuplicationDocument3 pagesAppendix DuplicationMario TrejoNo ratings yet
- Emerg 3 168Document2 pagesEmerg 3 168Randy SaputraNo ratings yet
- Urachal Carcinoma With Liver Lung and Brain MetastDocument5 pagesUrachal Carcinoma With Liver Lung and Brain Metast7fkqx7zh7pNo ratings yet
- A True Complete Diphalliahas Proven To Be A More Complex Case of Caudal Duplication SyndromeDocument4 pagesA True Complete Diphalliahas Proven To Be A More Complex Case of Caudal Duplication SyndromeLuminita PopaNo ratings yet
- A Rare Germ-Cell Tumor Site: Vaginal Endodermal Sinus Tumor: CasereportDocument3 pagesA Rare Germ-Cell Tumor Site: Vaginal Endodermal Sinus Tumor: CasereportmonicamoniccNo ratings yet
- Herman 2012Document20 pagesHerman 2012dewaprasatyaNo ratings yet
- Stroke and Cerebrovascular Disease in ChildhoodFrom EverandStroke and Cerebrovascular Disease in ChildhoodVijeya GanesanNo ratings yet
- ENGLISH Teacher - S Guide-GRADE 3 (2nd Quarter)Document112 pagesENGLISH Teacher - S Guide-GRADE 3 (2nd Quarter)dyancris2567% (3)
- Actual and Potential Gifts: Critique, Shadow Gift Relations and The Virtual Domain of The UngivenDocument22 pagesActual and Potential Gifts: Critique, Shadow Gift Relations and The Virtual Domain of The Ungivenanaid_ortíz_5No ratings yet
- Malala YousafzaiDocument1 pageMalala YousafzaiYu Myat SoeNo ratings yet
- The Lived Experiencesof Lesbian Gayand Bisexual Youth During Their Secondary EducationDocument28 pagesThe Lived Experiencesof Lesbian Gayand Bisexual Youth During Their Secondary EducationFranci CerezaNo ratings yet
- LysineDocument18 pagesLysineYob YnnosNo ratings yet
- The Perennial PhilosophyDocument14 pagesThe Perennial Philosophybrodie21100% (1)
- Drug Study ObDocument6 pagesDrug Study Obednaria100% (1)
- Cath SAP 5Document47 pagesCath SAP 5Angel AliNo ratings yet
- Module 3 - Topic 5 (Retail Inventory Method)Document4 pagesModule 3 - Topic 5 (Retail Inventory Method)Ann BergonioNo ratings yet
- Claudio Monteverdi: BarrioDocument14 pagesClaudio Monteverdi: BarrioNadir BarrioNo ratings yet
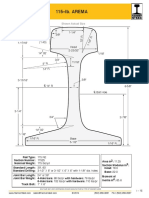
- Arema 115REDocument1 pageArema 115REAntonioNo ratings yet
- Numerical Grid Generation Techniques - NASADocument563 pagesNumerical Grid Generation Techniques - NASAMárioSilva100% (1)
- Plan Implementation and Management - Ii (M.A. E.P.M. 6562)Document22 pagesPlan Implementation and Management - Ii (M.A. E.P.M. 6562)Ahmer KhalilNo ratings yet
- Guid Line Drug TX PDFDocument707 pagesGuid Line Drug TX PDFmaezu100% (1)
- The Hinsberg TestDocument1 pageThe Hinsberg TestPravin Negi50% (2)
- Ebook Handbook of The Psychology of Aging PDF Full Chapter PDFDocument67 pagesEbook Handbook of The Psychology of Aging PDF Full Chapter PDFforest.gertelman418100% (39)
- 9702 m19 Ms 12Document3 pages9702 m19 Ms 12And rewNo ratings yet
- In Re Forchion, B227341 (CA. Ct. App. Aug 31, 2011)Document38 pagesIn Re Forchion, B227341 (CA. Ct. App. Aug 31, 2011)Venkat BalasubramaniNo ratings yet
- A Transcription of Jean Françaix'S L'Horloge de Flore For Solo Oboe and Organ (Four Hands)Document67 pagesA Transcription of Jean Françaix'S L'Horloge de Flore For Solo Oboe and Organ (Four Hands)Juan MendozaNo ratings yet
- M.Sc. Nursing Syllabus and RegulationDocument145 pagesM.Sc. Nursing Syllabus and RegulationSanthosh.S.UNo ratings yet
- LF412Document11 pagesLF412Alexandru CaracosteaNo ratings yet
- Sonny Lo vs. KJS Eco-Formwork System Phil, Inc, GR No. 149420 (2003)Document2 pagesSonny Lo vs. KJS Eco-Formwork System Phil, Inc, GR No. 149420 (2003)Je S BeNo ratings yet
- Jamaica Cultural Immersion Program FINALDocument2 pagesJamaica Cultural Immersion Program FINALLinda zubyNo ratings yet
- Teachers' Self-Efficacy Beliefs, Self-Esteem, and Job Stress As Determinants of Job SatisfactionDocument14 pagesTeachers' Self-Efficacy Beliefs, Self-Esteem, and Job Stress As Determinants of Job SatisfactionEffeNo ratings yet
- Beginning Practicecu EdocDocument128 pagesBeginning Practicecu Edocapi-236393707No ratings yet