Download as pdf or txt
You might also like
- Case Report GERDDocument7 pagesCase Report GERDNofilia Citra Candra100% (1)
- Naplex Complete Study Outline A Topic-Wise Approach DiabetesFrom EverandNaplex Complete Study Outline A Topic-Wise Approach DiabetesRating: 4.5 out of 5 stars4.5/5 (3)
- 1 Sec GERD GITDocument85 pages1 Sec GERD GITtyleree3No ratings yet
- Dr. K. Sendhil Kumar Dr. Piyush Patwa Dr. Latif Bagwan Gateway Clinic & Hospitals Coimbatore, INDIADocument62 pagesDr. K. Sendhil Kumar Dr. Piyush Patwa Dr. Latif Bagwan Gateway Clinic & Hospitals Coimbatore, INDIAJOPEARL MAE DELA TORRE100% (1)
- GERD ManagementDocument43 pagesGERD ManagementpashaNo ratings yet
- Gastroesophageal Reflux Disease: Scott Stolte, Pharm.D. Shenandoah UniversityDocument48 pagesGastroesophageal Reflux Disease: Scott Stolte, Pharm.D. Shenandoah UniversitymnmrznNo ratings yet
- Pharmacotherapy 1 GIS Self CarepdfDocument40 pagesPharmacotherapy 1 GIS Self Carepdfelifuygur09No ratings yet
- GerdDocument38 pagesGerdZANo ratings yet
- Chapter 13 Heartburn and DyspepsiaDocument10 pagesChapter 13 Heartburn and DyspepsiaPia Angelica DizonNo ratings yet
- Gastroesophageal Reflux DiseaseDocument36 pagesGastroesophageal Reflux DiseaseAlexNo ratings yet
- GERDDocument38 pagesGERDss33% (3)
- 2 CARE OF CLIENTS GERD HIATAL HERNIA ACHALASIA PUD GI BLEEDING FinalDocument114 pages2 CARE OF CLIENTS GERD HIATAL HERNIA ACHALASIA PUD GI BLEEDING Finalevren yilmazNo ratings yet
- Drugs Affecting The Gastrointestinal TractDocument61 pagesDrugs Affecting The Gastrointestinal TractSameera DahamNo ratings yet
- 01 Esophagus - GerdDocument129 pages01 Esophagus - Gerdacatrinei_daniela_2100% (1)
- 2 - GerdDocument26 pages2 - GerdEslam HamadaNo ratings yet
- Gastroesophagea L of Reflux Disease (GERD)Document34 pagesGastroesophagea L of Reflux Disease (GERD)Alyda Choirunnissa SudiratnaNo ratings yet
- Printed Material Module 7 Gastrointestinal System Drugs - PDFDocument45 pagesPrinted Material Module 7 Gastrointestinal System Drugs - PDFShang MacarayonNo ratings yet
- Esophageal PathologyDocument8 pagesEsophageal PathologyAndra BauerNo ratings yet
- Gi PharmacologyDocument13 pagesGi PharmacologyyeshiwasdagnewNo ratings yet
- Non Steroidal Anti Inflamatory Drugs - Non Steroidal Anti Inflamatory Drugs - Non Steroidal Anti Inflamatory DrugsDocument15 pagesNon Steroidal Anti Inflamatory Drugs - Non Steroidal Anti Inflamatory Drugs - Non Steroidal Anti Inflamatory DrugsChristian SolihinNo ratings yet
- Gastrointestinal DrugsDocument45 pagesGastrointestinal DrugsCindy MaslagNo ratings yet
- Gerd Gastroesophagial Reflux DiseaseDocument8 pagesGerd Gastroesophagial Reflux DiseaseJamie VaughnNo ratings yet
- Anti-Ulcer Drug Report FinallllDocument17 pagesAnti-Ulcer Drug Report FinallllJeloume De GuzmanNo ratings yet
- 5a.ESOPHAGEAL DISORDERSDocument16 pages5a.ESOPHAGEAL DISORDERSHayat AL AKOUMNo ratings yet
- Dyspepsia: Dr. Arif Nur Widodo SP - PDDocument31 pagesDyspepsia: Dr. Arif Nur Widodo SP - PDMonica Kristina HutabaratNo ratings yet
- Gastroesophageal Reflux Disease (GERD)Document37 pagesGastroesophageal Reflux Disease (GERD)CraciunElenaNo ratings yet
- Gastrointestinal DrugDocument29 pagesGastrointestinal DrugJeneyse Ajap BalcenaNo ratings yet
- GERDDocument20 pagesGERDSINDHOOR S MNo ratings yet
- Drugs Used in GIT DisordersDocument46 pagesDrugs Used in GIT Disordersسلطان القلحNo ratings yet
- Acid Peptic Disorder and GerdDocument52 pagesAcid Peptic Disorder and GerdEbuka AniNo ratings yet
- What Is Gastroesophogeal Reflux DiseaseDocument14 pagesWhat Is Gastroesophogeal Reflux DiseaseAhmed SadNo ratings yet
- Gastroesophageal Reflux Disease: SymptomsDocument8 pagesGastroesophageal Reflux Disease: Symptomspragna novaNo ratings yet
- Takvani Pediatric GERD - CME SlidesDocument41 pagesTakvani Pediatric GERD - CME SlidesTakvani Harshad100% (1)
- Rani Ti DineDocument2 pagesRani Ti DineCarl Sagisabal IbascoNo ratings yet
- Gerd - Gastroesophageal Reflux Disease Case PresentationDocument26 pagesGerd - Gastroesophageal Reflux Disease Case PresentationNadzfeeqNo ratings yet
- GastroenterologyDocument94 pagesGastroenterologyAdina RomanNo ratings yet
- Problem 2 GI - VICKA AZWITADocument65 pagesProblem 2 GI - VICKA AZWITARana RickNo ratings yet
- Gerd - NCCP - Kppik 2011 (Hotel Shangri La)Document28 pagesGerd - NCCP - Kppik 2011 (Hotel Shangri La)Fatmala HaningtyasNo ratings yet
- 1) GerdDocument28 pages1) GerdmohamadamirulariffinNo ratings yet
- GERDDocument24 pagesGERDBEVERLY JANE COPADANo ratings yet
- OmeprazoleDocument3 pagesOmeprazoleapi-3797941100% (3)
- Gastroesophageal Reflux Disease (GERD) : Types of HeartburnDocument12 pagesGastroesophageal Reflux Disease (GERD) : Types of HeartburnSara Al-FerkhNo ratings yet
- Drug Indication Action Side Effects and Adverse Reaction Nursing ConsiderationDocument8 pagesDrug Indication Action Side Effects and Adverse Reaction Nursing Considerationkier khierNo ratings yet
- Drug StudyDocument10 pagesDrug Studytamtam_antonioNo ratings yet
- Gastrointestinal Diseases: Clinical Pharmacist Hasan BayashotDocument117 pagesGastrointestinal Diseases: Clinical Pharmacist Hasan BayashotRawabi SalehNo ratings yet
- GerdDocument49 pagesGerdAhmed NourNo ratings yet
- Case-Based Learning (CBL) Module: Gerd in Daily Practice: How To Diagnose and Treat It Effectively ?Document53 pagesCase-Based Learning (CBL) Module: Gerd in Daily Practice: How To Diagnose and Treat It Effectively ?Ditia RahimNo ratings yet
- Gastroesofag RefluxDocument4 pagesGastroesofag RefluxRizaldy KehiNo ratings yet
- GERBDocument24 pagesGERBdevutty 123No ratings yet
- Drugs Affecting Gastrointestinal (GI) Secretions: CUIZON, Ariel GONZALES, Claire Marie PLAZA, GabrielDocument29 pagesDrugs Affecting Gastrointestinal (GI) Secretions: CUIZON, Ariel GONZALES, Claire Marie PLAZA, GabrielKay GonzalesNo ratings yet
- Pharmacotherapy For GERDDocument6 pagesPharmacotherapy For GERDJoon HyungNo ratings yet
- Cimetidine (Drug Study)Document2 pagesCimetidine (Drug Study)Franz.thenurse6888100% (1)
- Digestive SystemDocument55 pagesDigestive SystemPradeep KonduriNo ratings yet
- Functional DyspepsiaDocument17 pagesFunctional DyspepsiaSasoo EmadNo ratings yet
- Peptic Ulcer Disease: Dr. Isbandiyah, SPPDDocument14 pagesPeptic Ulcer Disease: Dr. Isbandiyah, SPPDMohammad SutamiNo ratings yet
- Gastroesophageal Reflux Disease: (GERD)Document23 pagesGastroesophageal Reflux Disease: (GERD)Shinta MayasariNo ratings yet
- FamotidineDocument3 pagesFamotidineapi-3797941No ratings yet
- Garopride ManualDocument16 pagesGaropride Manualsherif_awadNo ratings yet
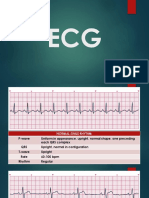
- Ecg HandoutDocument24 pagesEcg HandoutLeah DeeNo ratings yet
- A Twins With Congenital Heart Disease: A Case ReportDocument5 pagesA Twins With Congenital Heart Disease: A Case ReportInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- Oral Cancer ScreeningDocument9 pagesOral Cancer ScreeningenNo ratings yet
- CASE PRESENTATION NEPHROTIC Syndrome-1Document20 pagesCASE PRESENTATION NEPHROTIC Syndrome-1rohankananiNo ratings yet
- International Journal of Radiology and Imaging Technology Ijrit 8 089Document4 pagesInternational Journal of Radiology and Imaging Technology Ijrit 8 089khalizamaulinaNo ratings yet
- Abdomen Macleod - S - Clinical - Examination - 15thDocument28 pagesAbdomen Macleod - S - Clinical - Examination - 15thwxyngtc4n9No ratings yet
- Is Physical Activity and Diet Having A Spot in Periodontal and Respiratory Health A ReviewDocument7 pagesIs Physical Activity and Diet Having A Spot in Periodontal and Respiratory Health A ReviewAthenaeum Scientific PublishersNo ratings yet
- Nasal Polyps (2022)Document13 pagesNasal Polyps (2022)ChinciaNo ratings yet
- Neuro-Muscular Dysfunction in Children (PHN) McqsDocument10 pagesNeuro-Muscular Dysfunction in Children (PHN) McqsHira KhanNo ratings yet
- Adult Full Assessment With MSEDocument7 pagesAdult Full Assessment With MSEmary grace bialenNo ratings yet
- Exercise - Induced AsthmaDocument2 pagesExercise - Induced AsthmaTeoNo ratings yet
- 5 - Harvard Trauma Questionnaire HTQ-R and Hopkins Symptom Checklist HSCL-25Document23 pages5 - Harvard Trauma Questionnaire HTQ-R and Hopkins Symptom Checklist HSCL-25Fatima HassanNo ratings yet
- Zollinger Ellis Wps OfficeDocument15 pagesZollinger Ellis Wps OfficeAbhash MishraNo ratings yet
- DeliriumDocument37 pagesDeliriumalishba iqbal 1112No ratings yet
- Lesson 5. Health and NutritionDocument5 pagesLesson 5. Health and NutritionLoveyysolonNo ratings yet
- Umnl Vs LMNLDocument5 pagesUmnl Vs LMNLBell GatesNo ratings yet
- Usa 2Document6 pagesUsa 2Aiman ArifinNo ratings yet
- 4 Immunizations1Document37 pages4 Immunizations1خالد المعلميNo ratings yet
- Mental Health Awareness - Google SearchDocument1 pageMental Health Awareness - Google SearchMercy DxbbNo ratings yet
- CI-01 - Cancer (Kanser)Document2 pagesCI-01 - Cancer (Kanser)jijiqNo ratings yet
- Unit - I Introduction: Subjects Notes BSC Nursing Part - I Subject: NutritionDocument14 pagesUnit - I Introduction: Subjects Notes BSC Nursing Part - I Subject: NutritionHemant SharmaNo ratings yet
- Summary Hivaids SetDocument747 pagesSummary Hivaids Setv8qwxqb2shNo ratings yet
- Case Scenario 3.editedDocument7 pagesCase Scenario 3.editedPoetic YatchyNo ratings yet
- Rheumatological History Taking OSCE GuideDocument11 pagesRheumatological History Taking OSCE GuideChen BrionesNo ratings yet
- 07 Sepsis - Dr. Sutrisno, M.Kes., SP - OG., Subsp. ONK.Document31 pages07 Sepsis - Dr. Sutrisno, M.Kes., SP - OG., Subsp. ONK.Syahid PutraNo ratings yet
- Case Report A Chinese Patient With Spinocerebellar Ataxia Finally Confirmed As Gerstmann-Sträussler-Scheinker Syndrome With P102L MutationDocument16 pagesCase Report A Chinese Patient With Spinocerebellar Ataxia Finally Confirmed As Gerstmann-Sträussler-Scheinker Syndrome With P102L MutationLídia YoshiharaNo ratings yet
- West Nile VirusDocument1 pageWest Nile VirusBaidawu Weso-amo IbrahimNo ratings yet
- Surveilance Data Summery PresentationDocument14 pagesSurveilance Data Summery PresentationSHILOTANo ratings yet
- Kebt108 PDFDocument16 pagesKebt108 PDFAdrija DasNo ratings yet
- High Blood PressureDocument5 pagesHigh Blood PressureHelena AzevedoNo ratings yet