Download as pdf or txt
You might also like
- Fiona Apple All LyricsDocument74 pagesFiona Apple All Lyricsscarlett_merino0% (1)
- PerDev - Q2 - Module 3Document45 pagesPerDev - Q2 - Module 3jeysel calumbaNo ratings yet
- Urinary Tract InfectionDocument10 pagesUrinary Tract InfectionMira Mariana UlfahNo ratings yet
- TuberculosisDocument5 pagesTuberculosiscecil100% (6)
- Urinary Tract InfectionDocument23 pagesUrinary Tract InfectionAs SyarifNo ratings yet
- MK-Ultra - The Monarch ProjectDocument2 pagesMK-Ultra - The Monarch ProjectRyanADNo ratings yet
- Eci Ip Over DWDM White PaperDocument8 pagesEci Ip Over DWDM White PaperranjitNo ratings yet
- Notes On UtiDocument15 pagesNotes On UtiSaleh Mohammad ShoaibNo ratings yet
- Canuuc - Uti May 2017Document31 pagesCanuuc - Uti May 2017Praluki HerliawanNo ratings yet
- Chapter 36 The Urinary System in GynaecologyDocument19 pagesChapter 36 The Urinary System in Gynaecologypmj050gpNo ratings yet
- M1 - Urinary DisordersDocument2 pagesM1 - Urinary DisordersjuiceNo ratings yet
- Urological InfectionsDocument21 pagesUrological Infections<_>No ratings yet
- UTI Treatment Algorithm - Sharp Mesa Vista 2Document3 pagesUTI Treatment Algorithm - Sharp Mesa Vista 2Fitri 1997No ratings yet
- Drug Study NicoleDocument6 pagesDrug Study NicoleFrancheska Nicole Delos SantosNo ratings yet
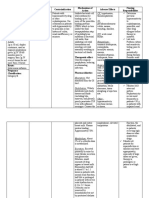
- Drug Study: Drug/Classification Dose/Route Mechanism of Action Common Side Effects Nursing ResponsibilitiesDocument4 pagesDrug Study: Drug/Classification Dose/Route Mechanism of Action Common Side Effects Nursing ResponsibilitiesLiiza G-GsprNo ratings yet
- Causes of Acute PeritonitisDocument6 pagesCauses of Acute PeritonitisYalin AbouhassiraNo ratings yet
- By. Dr. Wondifraw ADocument30 pagesBy. Dr. Wondifraw ASebliNo ratings yet
- mmahfileSOC 10-11-7 PDFDocument4 pagesmmahfileSOC 10-11-7 PDFbaongantran2122002No ratings yet
- 8.urinary Tract Infections-1Document82 pages8.urinary Tract Infections-1fikirjohn8No ratings yet
- Referat - Syifa Firza UtiDocument28 pagesReferat - Syifa Firza Utimiir ikbalNo ratings yet
- Cefoxitin Drug StudyDocument3 pagesCefoxitin Drug StudyBea Dela Cena100% (2)
- Name of Drug Dosage, Route, Frequency and Timing Mechanism of Action Indication Adverse Reactions Special Precautions Nursing ResponsibilitiesDocument3 pagesName of Drug Dosage, Route, Frequency and Timing Mechanism of Action Indication Adverse Reactions Special Precautions Nursing ResponsibilitiesKaren Kaye CordovaNo ratings yet
- UTI in Pregnancy (Diagnosis + Management)Document3 pagesUTI in Pregnancy (Diagnosis + Management)fatoom2022No ratings yet
- Approach To A Patient With Urinary Tract Infection UTI-2Document53 pagesApproach To A Patient With Urinary Tract Infection UTI-2maruf47774No ratings yet
- Urinary Tract InfectionDocument42 pagesUrinary Tract InfectionhaniNo ratings yet
- G 8 - ProstatitisDocument22 pagesG 8 - Prostatitisntwali danNo ratings yet
- Genitourinary Infections For ClassDocument74 pagesGenitourinary Infections For ClassKashif BurkiNo ratings yet
- Vrebsc 180521172503Document16 pagesVrebsc 180521172503D. Melba S.S ChinnaNo ratings yet
- Paediatric UTIDocument24 pagesPaediatric UTIIlobun Faithful IziengbeNo ratings yet
- BAHAN KULIAH - Urinary Tract InfectionDocument24 pagesBAHAN KULIAH - Urinary Tract Infectionevi_kkITNo ratings yet
- PYELONEPHRITISDocument1 pagePYELONEPHRITISgreskpremium8No ratings yet
- SHC Intra Abdominal GuidelinesDocument13 pagesSHC Intra Abdominal GuidelinesNguyễn Mạnh CườngNo ratings yet
- Evropski Univerzitet "Kallos" Fakultet Zdravstvenih Nauka Sestrinstvo Predmet: HirurgijaDocument24 pagesEvropski Univerzitet "Kallos" Fakultet Zdravstvenih Nauka Sestrinstvo Predmet: HirurgijaEnisaBilalicNo ratings yet
- PeritonitisDocument15 pagesPeritonitiscgqphqdrytNo ratings yet
- Antibiotic Case StudiesDocument28 pagesAntibiotic Case StudieskylietanglsNo ratings yet
- EAU Pocket Guidelines Urological - Infections 2012 PDFDocument18 pagesEAU Pocket Guidelines Urological - Infections 2012 PDFbrukner30No ratings yet
- Urinary Tract Infection: Prof DR DR Jazanul Anwar SPFKDocument32 pagesUrinary Tract Infection: Prof DR DR Jazanul Anwar SPFKdouce3No ratings yet
- Infections of The Upper & Lower Genital Tract: Teresita R. Tablizo Fpogs, FpsuogDocument76 pagesInfections of The Upper & Lower Genital Tract: Teresita R. Tablizo Fpogs, FpsuogPrincess Aira Bucag CarbonelNo ratings yet
- Drug Mechanism of Action/side Effects Indication/ Contraindication Nursing ResponsibilitiesDocument2 pagesDrug Mechanism of Action/side Effects Indication/ Contraindication Nursing ResponsibilitiesSheryhan Tahir BayleNo ratings yet
- Acute Pyelonephritis: Diagnostic Test ResultsDocument2 pagesAcute Pyelonephritis: Diagnostic Test ResultschoobiNo ratings yet
- Sti 2018 LseDocument67 pagesSti 2018 LsespinosumNo ratings yet
- Urinary Tract Infection - KULIAH MAHASISWADocument27 pagesUrinary Tract Infection - KULIAH MAHASISWAradhiinathahirNo ratings yet
- Acterial Yelonephritis: Jennifer Good, DVM Mark P. Rondeau, DVM, DACVIM (SAIM)Document5 pagesActerial Yelonephritis: Jennifer Good, DVM Mark P. Rondeau, DVM, DACVIM (SAIM)Phương Liên Nguyễn ThịNo ratings yet
- Pharmacotherapy of Infectious Disease:: 6. Urinary Tract Infections and ProstatitisDocument26 pagesPharmacotherapy of Infectious Disease:: 6. Urinary Tract Infections and ProstatitisDigafe TolaNo ratings yet
- Infeksionet e Traktit Urinar 4Document23 pagesInfeksionet e Traktit Urinar 4Lindrit AliuNo ratings yet
- Neurogenic Bladder UrethritisDocument2 pagesNeurogenic Bladder UrethritisOlivia LowellNo ratings yet
- Comprehension of Acute PyelonephritisDocument23 pagesComprehension of Acute PyelonephritisAmeliaNo ratings yet
- Comprehension of Acute PyelonephritisDocument23 pagesComprehension of Acute PyelonephritisAmeliaNo ratings yet
- 2018 COMPARATIVE MICRO MeningoencephalitisDocument6 pages2018 COMPARATIVE MICRO MeningoencephalitisMarianneTee-ruhNo ratings yet
- Urinary Tract InfectionDocument50 pagesUrinary Tract InfectionAhmad SobihNo ratings yet
- PyelonephritisDocument34 pagesPyelonephritisdc9skhsvbbNo ratings yet
- Omep, Ceftriaxone, FurosemideDocument3 pagesOmep, Ceftriaxone, FurosemideThyataira chuaNo ratings yet
- Infection Antimicrobial Medication CardsDocument16 pagesInfection Antimicrobial Medication Cards方郝建No ratings yet
- Urinary Tract Infections (UTI) in Older Adults WWW - Rxfiles.caDocument7 pagesUrinary Tract Infections (UTI) in Older Adults WWW - Rxfiles.caAwais KhanNo ratings yet
- 2 тема Книгавко URINARY TRACT INFECTIONSDocument62 pages2 тема Книгавко URINARY TRACT INFECTIONSSoumya Ranjan PandaNo ratings yet
- PyelonephritisDocument10 pagesPyelonephritisalina abu rumi100% (1)
- Drug StudyDocument22 pagesDrug StudySierraSiwaNo ratings yet
- Drug StudyDocument22 pagesDrug StudySierraSiwaNo ratings yet
- Urinary Tract Infection: Tbilisi Referral Hospital, Tbilisi, Georgia Nephrologist Nino MaglakelidzeDocument50 pagesUrinary Tract Infection: Tbilisi Referral Hospital, Tbilisi, Georgia Nephrologist Nino MaglakelidzePayal bhagatNo ratings yet
- Urinary Tract Infections Definition: ClassificationDocument3 pagesUrinary Tract Infections Definition: Classificationjishu baruaNo ratings yet
- Urinary Tract Infections (UTI)Document58 pagesUrinary Tract Infections (UTI)afdaliaNo ratings yet
- Antibiotic Policy JIPMER UTIDocument6 pagesAntibiotic Policy JIPMER UTIRpmhouseNo ratings yet
- Amoebic DysenteryDocument11 pagesAmoebic DysenterymadelynmasNo ratings yet
- Female Urinary Tract Infections in Clinical PracticeFrom EverandFemale Urinary Tract Infections in Clinical PracticeBob YangNo ratings yet
- A 40-Year-Old Man With Behavioural AbnormalitiesDocument30 pagesA 40-Year-Old Man With Behavioural AbnormalitiesSaleh Mohammad ShoaibNo ratings yet
- Latest Dr. Saleh Facial Nerve Applied 16.5.23Document85 pagesLatest Dr. Saleh Facial Nerve Applied 16.5.23Saleh Mohammad ShoaibNo ratings yet
- Personal Notes On Scabies IllustratedDocument15 pagesPersonal Notes On Scabies IllustratedSaleh Mohammad ShoaibNo ratings yet
- Peripheral Atherosclerotic DiseaseDocument22 pagesPeripheral Atherosclerotic DiseaseSaleh Mohammad ShoaibNo ratings yet
- Notes On BPHDocument7 pagesNotes On BPHSaleh Mohammad ShoaibNo ratings yet
- National Epilepsy Consensus Guideline of BangladeshDocument130 pagesNational Epilepsy Consensus Guideline of BangladeshSaleh Mohammad ShoaibNo ratings yet
- Canadian Open Mathematics Challenge: The Canadian Mathematical SocietyDocument3 pagesCanadian Open Mathematics Challenge: The Canadian Mathematical Societyสฮาบูดีน สาและNo ratings yet
- LiteratureDocument8 pagesLiteratureHasna Elle SalendabNo ratings yet
- A Novel Temporary Anchorage Device Aided SectionalDocument8 pagesA Novel Temporary Anchorage Device Aided Sectionalhector rinconNo ratings yet
- Joao Baptista Lukombo Nzatuzola-2 PDFDocument4 pagesJoao Baptista Lukombo Nzatuzola-2 PDFMadaleno Sita António DiasNo ratings yet
- Jacques Derrida, The Ontolo-Theology of National HumanismDocument22 pagesJacques Derrida, The Ontolo-Theology of National Humanismmikey litwackNo ratings yet
- Gabriel by Adrienne RichDocument5 pagesGabriel by Adrienne RichZahid ImranNo ratings yet
- Esteban v. Prince William Cnty, 4th Cir. (2001)Document2 pagesEsteban v. Prince William Cnty, 4th Cir. (2001)Scribd Government DocsNo ratings yet
- Topic 2: Entrepreneurial ManagementDocument9 pagesTopic 2: Entrepreneurial ManagementAmrezaa IskandarNo ratings yet
- Implicit DifferentiationDocument12 pagesImplicit DifferentiationNaitsirc UluputipanNo ratings yet
- MOdern ToolsDocument6 pagesMOdern ToolsingesbiemarinoNo ratings yet
- 1Document47 pages1Lehleh HiiNo ratings yet
- 90.FT. Salvatierra v. Garlitos, 103 Phil. 757 (1958)Document3 pages90.FT. Salvatierra v. Garlitos, 103 Phil. 757 (1958)IamIvy Donna PondocNo ratings yet
- 9 EeeDocument82 pages9 EeeRiya AgrawalNo ratings yet
- Let Water Burn: SUMMARY (Expounded Perchapter)Document10 pagesLet Water Burn: SUMMARY (Expounded Perchapter)Johndale DimayugaNo ratings yet
- Contracting From East To West Bridging The CulturalDocument8 pagesContracting From East To West Bridging The CulturalNiketa JaiswalNo ratings yet
- "Noah Webster" 1. Who Was Noah Webster?Document9 pages"Noah Webster" 1. Who Was Noah Webster?Yo A SecasNo ratings yet
- 1.1 The Role of Imagination in Narrative Construction-2Document21 pages1.1 The Role of Imagination in Narrative Construction-2RainforestLeadership MccaNo ratings yet
- 20752-Reservoir Management Training An Lntegrated ApproachDocument6 pages20752-Reservoir Management Training An Lntegrated ApproachdanonninoNo ratings yet
- Saba Final Book For EdittingDocument643 pagesSaba Final Book For Edittingfaresjohnson4No ratings yet
- Meaning and Evolution of EntrepreneurshipDocument5 pagesMeaning and Evolution of EntrepreneurshipAnurag AllaNo ratings yet
- Branding Decisions: - Submitted byDocument8 pagesBranding Decisions: - Submitted byDiksha VashishthNo ratings yet
- Guide Investigator HandbookDocument45 pagesGuide Investigator HandbookCompaq Presario0% (1)
- Support Material Learning Activity 1: Aspects Vocabulary ExamplesDocument9 pagesSupport Material Learning Activity 1: Aspects Vocabulary ExamplesEmmanuel Campos OsorioNo ratings yet
- 32 Vaporization TNDocument4 pages32 Vaporization TNAjeng FadillahNo ratings yet
- Anatomi CT Scan ThoraxDocument23 pagesAnatomi CT Scan ThoraxMaria WahyuningsihNo ratings yet
- 20 Castillo vs. Republic, GR. No. 214064, Feb. 6, 2017Document2 pages20 Castillo vs. Republic, GR. No. 214064, Feb. 6, 2017Gloria, Melica Ina V.No ratings yet