
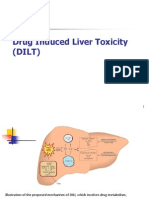
DIBD
DIBD
You might also like
- Hiroshima NotesDocument3 pagesHiroshima NotesKaitlin WendelNo ratings yet
- Persuasive Analytical Essays: Nguyen Khanh Huy EAP1119.5BDocument3 pagesPersuasive Analytical Essays: Nguyen Khanh Huy EAP1119.5BKhánh Huy NguyễnNo ratings yet
- Bone Marrow Failure VoiceoverDocument18 pagesBone Marrow Failure Voiceoverياسر كوثر هانيNo ratings yet
- Assignment 1 Pathology Aplastic Anemia: Supervisor: DR - Ramez Al-KeelaniDocument6 pagesAssignment 1 Pathology Aplastic Anemia: Supervisor: DR - Ramez Al-Keelaniameer mousaNo ratings yet
- Drugs Induce Hematologic DisordersDocument3 pagesDrugs Induce Hematologic DisorderspaymanmatinNo ratings yet
- Drug Induced Hematological Disorders-A Review: June 2019Document8 pagesDrug Induced Hematological Disorders-A Review: June 2019AbiNo ratings yet
- Toxic Responses of The BloodDocument10 pagesToxic Responses of The BloodM. Joyce100% (2)
- Bone Marrow Failure 2008-09Document15 pagesBone Marrow Failure 2008-09Karan BhattNo ratings yet
- Aplastic Anemia: Review of Etiology and TreatmentDocument7 pagesAplastic Anemia: Review of Etiology and TreatmentCleber MaiaNo ratings yet
- Bone Marrow Failure and Severe Aplastic Anemia Revision 1.1Document3 pagesBone Marrow Failure and Severe Aplastic Anemia Revision 1.1Rasha Al MousaNo ratings yet
- Aplastic Anemia - Pathogenesis, Clinical Manifestations, and Diagnosis - UpToDate PDFDocument21 pagesAplastic Anemia - Pathogenesis, Clinical Manifestations, and Diagnosis - UpToDate PDFWahyu Dwi NugrohoNo ratings yet
- Blood DiseasesDocument49 pagesBlood DiseasesAnoosha FarooquiNo ratings yet
- The Term Aplastic Anemia Indicates: Pancytopenia in The PresenceDocument34 pagesThe Term Aplastic Anemia Indicates: Pancytopenia in The PresenceKhadar mohamedNo ratings yet
- Ojim 2016091213324550Document10 pagesOjim 2016091213324550rianmg21No ratings yet
- Anemi Aplastik Dan MielodisplasiaDocument34 pagesAnemi Aplastik Dan MielodisplasiaRoby KieranNo ratings yet
- Aplastic AnemiaDocument29 pagesAplastic AnemiaGurkamal SinghNo ratings yet
- Drug Induced Liver Toxicity (DILD)Document39 pagesDrug Induced Liver Toxicity (DILD)Surya Pratama100% (1)
- Aplastic Anemia (Dr. Kadek)Document41 pagesAplastic Anemia (Dr. Kadek)galuh dharmapatniNo ratings yet
- Anemia: Differential DiagnosisDocument7 pagesAnemia: Differential DiagnosisZaman MigozaradNo ratings yet
- INTRO in AnemiaDocument3 pagesINTRO in AnemiaJeraiza Mendoza-LizarondoNo ratings yet
- Normocytic AnemiaDocument16 pagesNormocytic AnemiaPaula ArayaNo ratings yet
- Hematology Physiology 1Document6 pagesHematology Physiology 1Kyoheirwe vanessaNo ratings yet
- Bone Marrow FailureDocument4 pagesBone Marrow Failuremedicomauro2No ratings yet
- Case Study Output Aplastic AnemiaDocument7 pagesCase Study Output Aplastic AnemiaColeen Angelique MontenegroNo ratings yet
- Hemostasis Disorders in LeukemiaDocument14 pagesHemostasis Disorders in LeukemiaNurul HidayahNo ratings yet
- Anemias Aplastic Anemia Is A Condition Where Bone Marrow Does Not Produce Sufficient NewDocument15 pagesAnemias Aplastic Anemia Is A Condition Where Bone Marrow Does Not Produce Sufficient NewZoreyca RiveraNo ratings yet
- Iatrogenic Diseases: "First Do No Harm"-HippocratesDocument21 pagesIatrogenic Diseases: "First Do No Harm"-HippocratesPHARMACY 2021No ratings yet
- Aplastic AnemiaDocument11 pagesAplastic Anemiaquidditch07No ratings yet
- Aplastic Anemia: A Case Study OnDocument10 pagesAplastic Anemia: A Case Study OnVidge GrospeNo ratings yet
- Aplastic AnemiaDocument29 pagesAplastic AnemiaAshish SoniNo ratings yet
- Approach To Patient With Cytopenias: H. Atilla Özkan, MDDocument48 pagesApproach To Patient With Cytopenias: H. Atilla Özkan, MDYabetsNo ratings yet
- Case Report Pediatric Von&JepDocument23 pagesCase Report Pediatric Von&JepFarizan NurmushoffaNo ratings yet
- Clinical Manifestations, Pathologic Features, and Diagnosis of Acute Promyelocytic Leukemia in AdultsDocument10 pagesClinical Manifestations, Pathologic Features, and Diagnosis of Acute Promyelocytic Leukemia in AdultsANDREEA-CORNELIA NECULCEANo ratings yet
- Aplastic Anemia - An Overview: DR Aniruddh Shrivastava Guided By: DR S.H. Talib SIRDocument42 pagesAplastic Anemia - An Overview: DR Aniruddh Shrivastava Guided By: DR S.H. Talib SIRdoctoranswerit_84161No ratings yet
- Hematology 2 Lecture Notes Platelet Quantitative DisordersDocument10 pagesHematology 2 Lecture Notes Platelet Quantitative DisorderscccomayogNo ratings yet
- Aplastic AnemiaDocument26 pagesAplastic AnemiaIrina Moldovan100% (1)
- Aplastic AnemiaDocument6 pagesAplastic AnemiaChukwu Henry ParadiseNo ratings yet
- CBC 150106153749 Conversion Gate02Document44 pagesCBC 150106153749 Conversion Gate02KhetanNo ratings yet
- Blood DisordersDocument8 pagesBlood DisordersDeevashwer Rathee100% (1)
- Drugs Causing Throm Drugs Causing Thrombocytopenia or Low Platelet CountDocument4 pagesDrugs Causing Throm Drugs Causing Thrombocytopenia or Low Platelet CountDejan OgnjanovicNo ratings yet
- Kappler 2017Document23 pagesKappler 2017Alex CroNo ratings yet
- 6myelophthisic Anemia - StatPearls - NCBI BookshelfDocument5 pages6myelophthisic Anemia - StatPearls - NCBI BookshelfFernandoVignoloNo ratings yet
- Pathology of AnemiaDocument3 pagesPathology of AnemiaNesma AdelNo ratings yet
- Trombositopenia Dan TrombositosisDocument33 pagesTrombositopenia Dan TrombositosisAim AimmaNo ratings yet
- Anemia of InflammationDocument47 pagesAnemia of InflammationGebruNo ratings yet
- Aplastic Anemia Is A NormocyticDocument17 pagesAplastic Anemia Is A NormocyticAfrio ArismanNo ratings yet
- C B C I: Omplete Lood Ount NterpretationsDocument44 pagesC B C I: Omplete Lood Ount NterpretationsridhoniNo ratings yet
- Thrombotic Thrombocytopenic Purpura PDFDocument6 pagesThrombotic Thrombocytopenic Purpura PDFDany EdyNo ratings yet
- Kuliah Kelainan Leukosit & RES - ZIADocument114 pagesKuliah Kelainan Leukosit & RES - ZIAannnisaNo ratings yet
- Aplastic Anemia and Approach To Diagnosis in A Case of AnemiaDocument19 pagesAplastic Anemia and Approach To Diagnosis in A Case of Anemia2006suzainNo ratings yet
- Hematology Topics 16-20Document20 pagesHematology Topics 16-20Angelo Jude CobachaNo ratings yet
- Bone Marrow Hypoplasia 2023Document34 pagesBone Marrow Hypoplasia 2023Dafne LunaNo ratings yet
- Bone Marrow Hypoplasia 2022Document34 pagesBone Marrow Hypoplasia 2022Jose Angel Cobian GaliciaNo ratings yet
- Hema 2 5th Ed SummaryDocument9 pagesHema 2 5th Ed Summarymonzon.mika1801No ratings yet
- Haematological Manifestationsin SLE PDFDocument21 pagesHaematological Manifestationsin SLE PDFLe DungNo ratings yet
- MRCPass Notes For MRCP 1 - HEMATOLOGYDocument9 pagesMRCPass Notes For MRCP 1 - HEMATOLOGYsabdali100% (1)
- Physiology Group 2Document58 pagesPhysiology Group 2Akinmade AyobamiNo ratings yet
- Multiple Myeloma OverviewDocument52 pagesMultiple Myeloma OverviewanmegpraNo ratings yet
- Aplastic Anemia and HomoeopathyDocument3 pagesAplastic Anemia and HomoeopathyDr. Rajneesh Kumar Sharma MD Hom100% (1)
- The Complete Guide on Anemia: Learn Anemia Symptoms, Anemia Causes, and Anemia Treatments. Anemia types covered in full details: Iron-deficiency, Microcytic, Autoimmune Hemolytic, Sideroblastic, and Normocytic AnemiaFrom EverandThe Complete Guide on Anemia: Learn Anemia Symptoms, Anemia Causes, and Anemia Treatments. Anemia types covered in full details: Iron-deficiency, Microcytic, Autoimmune Hemolytic, Sideroblastic, and Normocytic AnemiaRating: 3.5 out of 5 stars3.5/5 (10)
- Comprehensive Insights into AA Amyloidosis: Understanding, Managing, and ThrivingFrom EverandComprehensive Insights into AA Amyloidosis: Understanding, Managing, and ThrivingNo ratings yet
- GLP Assessment WorksheetDocument24 pagesGLP Assessment WorksheetKabirNo ratings yet
- ANDA SubmissionsDocument15 pagesANDA SubmissionsKabirNo ratings yet
- Https Jmpas - Com Abstract 1132Document9 pagesHttps Jmpas - Com Abstract 1132KabirNo ratings yet
- SchizophreniaDocument11 pagesSchizophreniaKabirNo ratings yet
- SET 21 General (X)Document16 pagesSET 21 General (X)KabirNo ratings yet
- RAM TypesDocument11 pagesRAM TypesKabirNo ratings yet
- Reviewing The Requirements of ISO 9000Document3 pagesReviewing The Requirements of ISO 9000KabirNo ratings yet
- Antimicrobial 013502Document6 pagesAntimicrobial 013502KabirNo ratings yet
- Pharmacognosy 11250071Document124 pagesPharmacognosy 11250071KabirNo ratings yet
- AnticancerDocument19 pagesAnticancerKabirNo ratings yet
- Pharmaceutical ContaminationDocument3 pagesPharmaceutical ContaminationKabirNo ratings yet
- Pharmacuetics 11250072Document113 pagesPharmacuetics 11250072KabirNo ratings yet
- Inflammatory Bowel Disease: EpidemiologyDocument9 pagesInflammatory Bowel Disease: EpidemiologyKabirNo ratings yet
- EpilepsyDocument8 pagesEpilepsyKabirNo ratings yet
- Anxiety DisordersDocument8 pagesAnxiety DisordersKabirNo ratings yet
- He DacheDocument8 pagesHe DacheKabirNo ratings yet
- Drug Induced Liver DisordersDocument15 pagesDrug Induced Liver DisordersKabirNo ratings yet
- AnemiaDocument7 pagesAnemiaKabirNo ratings yet
- Venous ThromboembolismDocument10 pagesVenous ThromboembolismKabirNo ratings yet
- Evidence Based Medicine: Jan Baptist Van HelmontDocument4 pagesEvidence Based Medicine: Jan Baptist Van HelmontKabirNo ratings yet
- Pharmacology Terms & DefinitionDocument10 pagesPharmacology Terms & DefinitionKabirNo ratings yet
- EMA VICH Implementation Draft GuideDocument41 pagesEMA VICH Implementation Draft GuideKabirNo ratings yet
- Alzheimer DiseaseDocument6 pagesAlzheimer DiseaseKabirNo ratings yet
- Covid-19 Management: FAQs by HCWsDocument31 pagesCovid-19 Management: FAQs by HCWsKabirNo ratings yet
- Short Catalog 160719 HRDocument30 pagesShort Catalog 160719 HRtuanudinNo ratings yet
- School Orientation Narrative Report 1Document2 pagesSchool Orientation Narrative Report 1Marry Joy Molina100% (5)
- Di MCB DB Pricelist01!07!2018Document1 pageDi MCB DB Pricelist01!07!2018saurabhjerps231221No ratings yet
- EE - exam.PowerSystem - Feb 2 2015-2Document3 pagesEE - exam.PowerSystem - Feb 2 2015-2giophilipNo ratings yet
- NCP ConstipationDocument3 pagesNCP Constipationjlucando50% (2)
- MSDS Citronela OilDocument9 pagesMSDS Citronela OilIndra SanjayaNo ratings yet
- Supply Chain Management - Pgfa1941Document9 pagesSupply Chain Management - Pgfa1941Ravina SinghNo ratings yet
- Lysosome PresentationDocument5 pagesLysosome Presentationapi-241502402No ratings yet
- S Listing Ui Group Eae26ab3f22c4787 2603 125516 DefaultDocument16 pagesS Listing Ui Group Eae26ab3f22c4787 2603 125516 DefaulthcghealthcureNo ratings yet
- Gas Oil: Section 1 - Chemical Product and Company IdentificationDocument10 pagesGas Oil: Section 1 - Chemical Product and Company Identificationasep supriyadiNo ratings yet
- Oil Tank BylawDocument1 pageOil Tank BylawDec DmcNo ratings yet
- Design, Calculation and Simulation 3 Dof Capacitive Force SensorDocument5 pagesDesign, Calculation and Simulation 3 Dof Capacitive Force SensorLaNo ratings yet
- Osteological ReproductionsDocument88 pagesOsteological ReproductionsAntonioNo ratings yet
- Relationship Between Mortar and Early Age StrengthDocument24 pagesRelationship Between Mortar and Early Age StrengthMuhammadWazimAkramNo ratings yet
- Batch 3 UnescoDocument27 pagesBatch 3 UnescoHeaven Diaz100% (1)
- Magnum Ms - Pae DatasheetDocument1 pageMagnum Ms - Pae DatasheetGissell Del CastilloNo ratings yet
- E-STOP Relays, Safety Gate Monitors: Pnoz S5Document10 pagesE-STOP Relays, Safety Gate Monitors: Pnoz S5KAMRAN AHMEDNo ratings yet
- Ari Bag LocationDocument4 pagesAri Bag LocationIkram UlNo ratings yet
- 8 Sports Injury ManagementDocument21 pages8 Sports Injury ManagementPatch04No ratings yet
- IFIF@: Ehicle Request Form & Rigging PlanDocument1 pageIFIF@: Ehicle Request Form & Rigging PlanfahadullahNo ratings yet
- FOMAR-QTN-2019-20-117 Kamat PDFDocument1 pageFOMAR-QTN-2019-20-117 Kamat PDFPriyesh KamatNo ratings yet
- 3 Reasons Homework Should Be BannedDocument8 pages3 Reasons Homework Should Be Bannedersanb3k100% (1)
- CycloneDocument25 pagesCycloneAna Marie AllamNo ratings yet
- Design and Fabrication of Hybrid VehicleDocument4 pagesDesign and Fabrication of Hybrid VehicleRagbt CNo ratings yet
- Draka Power and InstrumentationDocument33 pagesDraka Power and Instrumentationnokaraju100% (1)
- Global Vaccine Action Plan: Tetanus & Difteri (TD/DPT)Document6 pagesGlobal Vaccine Action Plan: Tetanus & Difteri (TD/DPT)Gusti IndrakusumaNo ratings yet
- Pre-Extraction Records in Edentulous Patients - A Literature ReviewDocument6 pagesPre-Extraction Records in Edentulous Patients - A Literature ReviewMaywiNo ratings yet
- Datasheet Luxor 530W LX 530M 144 Bifacial HalfCell PERCDocument2 pagesDatasheet Luxor 530W LX 530M 144 Bifacial HalfCell PERCDimitarNo ratings yet
















































































































Download as docx, pdf, or txt
You might also like
- Hiroshima NotesDocument3 pagesHiroshima NotesKaitlin WendelNo ratings yet
- Persuasive Analytical Essays: Nguyen Khanh Huy EAP1119.5BDocument3 pagesPersuasive Analytical Essays: Nguyen Khanh Huy EAP1119.5BKhánh Huy NguyễnNo ratings yet
- Bone Marrow Failure VoiceoverDocument18 pagesBone Marrow Failure Voiceoverياسر كوثر هانيNo ratings yet
- Assignment 1 Pathology Aplastic Anemia: Supervisor: DR - Ramez Al-KeelaniDocument6 pagesAssignment 1 Pathology Aplastic Anemia: Supervisor: DR - Ramez Al-Keelaniameer mousaNo ratings yet
- Drugs Induce Hematologic DisordersDocument3 pagesDrugs Induce Hematologic DisorderspaymanmatinNo ratings yet
- Drug Induced Hematological Disorders-A Review: June 2019Document8 pagesDrug Induced Hematological Disorders-A Review: June 2019AbiNo ratings yet
- Toxic Responses of The BloodDocument10 pagesToxic Responses of The BloodM. Joyce100% (2)
- Bone Marrow Failure 2008-09Document15 pagesBone Marrow Failure 2008-09Karan BhattNo ratings yet
- Aplastic Anemia: Review of Etiology and TreatmentDocument7 pagesAplastic Anemia: Review of Etiology and TreatmentCleber MaiaNo ratings yet
- Bone Marrow Failure and Severe Aplastic Anemia Revision 1.1Document3 pagesBone Marrow Failure and Severe Aplastic Anemia Revision 1.1Rasha Al MousaNo ratings yet
- Aplastic Anemia - Pathogenesis, Clinical Manifestations, and Diagnosis - UpToDate PDFDocument21 pagesAplastic Anemia - Pathogenesis, Clinical Manifestations, and Diagnosis - UpToDate PDFWahyu Dwi NugrohoNo ratings yet
- Blood DiseasesDocument49 pagesBlood DiseasesAnoosha FarooquiNo ratings yet
- The Term Aplastic Anemia Indicates: Pancytopenia in The PresenceDocument34 pagesThe Term Aplastic Anemia Indicates: Pancytopenia in The PresenceKhadar mohamedNo ratings yet
- Ojim 2016091213324550Document10 pagesOjim 2016091213324550rianmg21No ratings yet
- Anemi Aplastik Dan MielodisplasiaDocument34 pagesAnemi Aplastik Dan MielodisplasiaRoby KieranNo ratings yet
- Aplastic AnemiaDocument29 pagesAplastic AnemiaGurkamal SinghNo ratings yet
- Drug Induced Liver Toxicity (DILD)Document39 pagesDrug Induced Liver Toxicity (DILD)Surya Pratama100% (1)
- Aplastic Anemia (Dr. Kadek)Document41 pagesAplastic Anemia (Dr. Kadek)galuh dharmapatniNo ratings yet
- Anemia: Differential DiagnosisDocument7 pagesAnemia: Differential DiagnosisZaman MigozaradNo ratings yet
- INTRO in AnemiaDocument3 pagesINTRO in AnemiaJeraiza Mendoza-LizarondoNo ratings yet
- Normocytic AnemiaDocument16 pagesNormocytic AnemiaPaula ArayaNo ratings yet
- Hematology Physiology 1Document6 pagesHematology Physiology 1Kyoheirwe vanessaNo ratings yet
- Bone Marrow FailureDocument4 pagesBone Marrow Failuremedicomauro2No ratings yet
- Case Study Output Aplastic AnemiaDocument7 pagesCase Study Output Aplastic AnemiaColeen Angelique MontenegroNo ratings yet
- Hemostasis Disorders in LeukemiaDocument14 pagesHemostasis Disorders in LeukemiaNurul HidayahNo ratings yet
- Anemias Aplastic Anemia Is A Condition Where Bone Marrow Does Not Produce Sufficient NewDocument15 pagesAnemias Aplastic Anemia Is A Condition Where Bone Marrow Does Not Produce Sufficient NewZoreyca RiveraNo ratings yet
- Iatrogenic Diseases: "First Do No Harm"-HippocratesDocument21 pagesIatrogenic Diseases: "First Do No Harm"-HippocratesPHARMACY 2021No ratings yet
- Aplastic AnemiaDocument11 pagesAplastic Anemiaquidditch07No ratings yet
- Aplastic Anemia: A Case Study OnDocument10 pagesAplastic Anemia: A Case Study OnVidge GrospeNo ratings yet
- Aplastic AnemiaDocument29 pagesAplastic AnemiaAshish SoniNo ratings yet
- Approach To Patient With Cytopenias: H. Atilla Özkan, MDDocument48 pagesApproach To Patient With Cytopenias: H. Atilla Özkan, MDYabetsNo ratings yet
- Case Report Pediatric Von&JepDocument23 pagesCase Report Pediatric Von&JepFarizan NurmushoffaNo ratings yet
- Clinical Manifestations, Pathologic Features, and Diagnosis of Acute Promyelocytic Leukemia in AdultsDocument10 pagesClinical Manifestations, Pathologic Features, and Diagnosis of Acute Promyelocytic Leukemia in AdultsANDREEA-CORNELIA NECULCEANo ratings yet
- Aplastic Anemia - An Overview: DR Aniruddh Shrivastava Guided By: DR S.H. Talib SIRDocument42 pagesAplastic Anemia - An Overview: DR Aniruddh Shrivastava Guided By: DR S.H. Talib SIRdoctoranswerit_84161No ratings yet
- Hematology 2 Lecture Notes Platelet Quantitative DisordersDocument10 pagesHematology 2 Lecture Notes Platelet Quantitative DisorderscccomayogNo ratings yet
- Aplastic AnemiaDocument26 pagesAplastic AnemiaIrina Moldovan100% (1)
- Aplastic AnemiaDocument6 pagesAplastic AnemiaChukwu Henry ParadiseNo ratings yet
- CBC 150106153749 Conversion Gate02Document44 pagesCBC 150106153749 Conversion Gate02KhetanNo ratings yet
- Blood DisordersDocument8 pagesBlood DisordersDeevashwer Rathee100% (1)
- Drugs Causing Throm Drugs Causing Thrombocytopenia or Low Platelet CountDocument4 pagesDrugs Causing Throm Drugs Causing Thrombocytopenia or Low Platelet CountDejan OgnjanovicNo ratings yet
- Kappler 2017Document23 pagesKappler 2017Alex CroNo ratings yet
- 6myelophthisic Anemia - StatPearls - NCBI BookshelfDocument5 pages6myelophthisic Anemia - StatPearls - NCBI BookshelfFernandoVignoloNo ratings yet
- Pathology of AnemiaDocument3 pagesPathology of AnemiaNesma AdelNo ratings yet
- Trombositopenia Dan TrombositosisDocument33 pagesTrombositopenia Dan TrombositosisAim AimmaNo ratings yet
- Anemia of InflammationDocument47 pagesAnemia of InflammationGebruNo ratings yet
- Aplastic Anemia Is A NormocyticDocument17 pagesAplastic Anemia Is A NormocyticAfrio ArismanNo ratings yet
- C B C I: Omplete Lood Ount NterpretationsDocument44 pagesC B C I: Omplete Lood Ount NterpretationsridhoniNo ratings yet
- Thrombotic Thrombocytopenic Purpura PDFDocument6 pagesThrombotic Thrombocytopenic Purpura PDFDany EdyNo ratings yet
- Kuliah Kelainan Leukosit & RES - ZIADocument114 pagesKuliah Kelainan Leukosit & RES - ZIAannnisaNo ratings yet
- Aplastic Anemia and Approach To Diagnosis in A Case of AnemiaDocument19 pagesAplastic Anemia and Approach To Diagnosis in A Case of Anemia2006suzainNo ratings yet
- Hematology Topics 16-20Document20 pagesHematology Topics 16-20Angelo Jude CobachaNo ratings yet
- Bone Marrow Hypoplasia 2023Document34 pagesBone Marrow Hypoplasia 2023Dafne LunaNo ratings yet
- Bone Marrow Hypoplasia 2022Document34 pagesBone Marrow Hypoplasia 2022Jose Angel Cobian GaliciaNo ratings yet
- Hema 2 5th Ed SummaryDocument9 pagesHema 2 5th Ed Summarymonzon.mika1801No ratings yet
- Haematological Manifestationsin SLE PDFDocument21 pagesHaematological Manifestationsin SLE PDFLe DungNo ratings yet
- MRCPass Notes For MRCP 1 - HEMATOLOGYDocument9 pagesMRCPass Notes For MRCP 1 - HEMATOLOGYsabdali100% (1)
- Physiology Group 2Document58 pagesPhysiology Group 2Akinmade AyobamiNo ratings yet
- Multiple Myeloma OverviewDocument52 pagesMultiple Myeloma OverviewanmegpraNo ratings yet
- Aplastic Anemia and HomoeopathyDocument3 pagesAplastic Anemia and HomoeopathyDr. Rajneesh Kumar Sharma MD Hom100% (1)
- The Complete Guide on Anemia: Learn Anemia Symptoms, Anemia Causes, and Anemia Treatments. Anemia types covered in full details: Iron-deficiency, Microcytic, Autoimmune Hemolytic, Sideroblastic, and Normocytic AnemiaFrom EverandThe Complete Guide on Anemia: Learn Anemia Symptoms, Anemia Causes, and Anemia Treatments. Anemia types covered in full details: Iron-deficiency, Microcytic, Autoimmune Hemolytic, Sideroblastic, and Normocytic AnemiaRating: 3.5 out of 5 stars3.5/5 (10)
- Comprehensive Insights into AA Amyloidosis: Understanding, Managing, and ThrivingFrom EverandComprehensive Insights into AA Amyloidosis: Understanding, Managing, and ThrivingNo ratings yet
- GLP Assessment WorksheetDocument24 pagesGLP Assessment WorksheetKabirNo ratings yet
- ANDA SubmissionsDocument15 pagesANDA SubmissionsKabirNo ratings yet
- Https Jmpas - Com Abstract 1132Document9 pagesHttps Jmpas - Com Abstract 1132KabirNo ratings yet
- SchizophreniaDocument11 pagesSchizophreniaKabirNo ratings yet
- SET 21 General (X)Document16 pagesSET 21 General (X)KabirNo ratings yet
- RAM TypesDocument11 pagesRAM TypesKabirNo ratings yet
- Reviewing The Requirements of ISO 9000Document3 pagesReviewing The Requirements of ISO 9000KabirNo ratings yet
- Antimicrobial 013502Document6 pagesAntimicrobial 013502KabirNo ratings yet
- Pharmacognosy 11250071Document124 pagesPharmacognosy 11250071KabirNo ratings yet
- AnticancerDocument19 pagesAnticancerKabirNo ratings yet
- Pharmaceutical ContaminationDocument3 pagesPharmaceutical ContaminationKabirNo ratings yet
- Pharmacuetics 11250072Document113 pagesPharmacuetics 11250072KabirNo ratings yet
- Inflammatory Bowel Disease: EpidemiologyDocument9 pagesInflammatory Bowel Disease: EpidemiologyKabirNo ratings yet
- EpilepsyDocument8 pagesEpilepsyKabirNo ratings yet
- Anxiety DisordersDocument8 pagesAnxiety DisordersKabirNo ratings yet
- He DacheDocument8 pagesHe DacheKabirNo ratings yet
- Drug Induced Liver DisordersDocument15 pagesDrug Induced Liver DisordersKabirNo ratings yet
- AnemiaDocument7 pagesAnemiaKabirNo ratings yet
- Venous ThromboembolismDocument10 pagesVenous ThromboembolismKabirNo ratings yet
- Evidence Based Medicine: Jan Baptist Van HelmontDocument4 pagesEvidence Based Medicine: Jan Baptist Van HelmontKabirNo ratings yet
- Pharmacology Terms & DefinitionDocument10 pagesPharmacology Terms & DefinitionKabirNo ratings yet
- EMA VICH Implementation Draft GuideDocument41 pagesEMA VICH Implementation Draft GuideKabirNo ratings yet
- Alzheimer DiseaseDocument6 pagesAlzheimer DiseaseKabirNo ratings yet
- Covid-19 Management: FAQs by HCWsDocument31 pagesCovid-19 Management: FAQs by HCWsKabirNo ratings yet
- Short Catalog 160719 HRDocument30 pagesShort Catalog 160719 HRtuanudinNo ratings yet
- School Orientation Narrative Report 1Document2 pagesSchool Orientation Narrative Report 1Marry Joy Molina100% (5)
- Di MCB DB Pricelist01!07!2018Document1 pageDi MCB DB Pricelist01!07!2018saurabhjerps231221No ratings yet
- EE - exam.PowerSystem - Feb 2 2015-2Document3 pagesEE - exam.PowerSystem - Feb 2 2015-2giophilipNo ratings yet
- NCP ConstipationDocument3 pagesNCP Constipationjlucando50% (2)
- MSDS Citronela OilDocument9 pagesMSDS Citronela OilIndra SanjayaNo ratings yet
- Supply Chain Management - Pgfa1941Document9 pagesSupply Chain Management - Pgfa1941Ravina SinghNo ratings yet
- Lysosome PresentationDocument5 pagesLysosome Presentationapi-241502402No ratings yet
- S Listing Ui Group Eae26ab3f22c4787 2603 125516 DefaultDocument16 pagesS Listing Ui Group Eae26ab3f22c4787 2603 125516 DefaulthcghealthcureNo ratings yet
- Gas Oil: Section 1 - Chemical Product and Company IdentificationDocument10 pagesGas Oil: Section 1 - Chemical Product and Company Identificationasep supriyadiNo ratings yet
- Oil Tank BylawDocument1 pageOil Tank BylawDec DmcNo ratings yet
- Design, Calculation and Simulation 3 Dof Capacitive Force SensorDocument5 pagesDesign, Calculation and Simulation 3 Dof Capacitive Force SensorLaNo ratings yet
- Osteological ReproductionsDocument88 pagesOsteological ReproductionsAntonioNo ratings yet
- Relationship Between Mortar and Early Age StrengthDocument24 pagesRelationship Between Mortar and Early Age StrengthMuhammadWazimAkramNo ratings yet
- Batch 3 UnescoDocument27 pagesBatch 3 UnescoHeaven Diaz100% (1)
- Magnum Ms - Pae DatasheetDocument1 pageMagnum Ms - Pae DatasheetGissell Del CastilloNo ratings yet
- E-STOP Relays, Safety Gate Monitors: Pnoz S5Document10 pagesE-STOP Relays, Safety Gate Monitors: Pnoz S5KAMRAN AHMEDNo ratings yet
- Ari Bag LocationDocument4 pagesAri Bag LocationIkram UlNo ratings yet
- 8 Sports Injury ManagementDocument21 pages8 Sports Injury ManagementPatch04No ratings yet
- IFIF@: Ehicle Request Form & Rigging PlanDocument1 pageIFIF@: Ehicle Request Form & Rigging PlanfahadullahNo ratings yet
- FOMAR-QTN-2019-20-117 Kamat PDFDocument1 pageFOMAR-QTN-2019-20-117 Kamat PDFPriyesh KamatNo ratings yet
- 3 Reasons Homework Should Be BannedDocument8 pages3 Reasons Homework Should Be Bannedersanb3k100% (1)
- CycloneDocument25 pagesCycloneAna Marie AllamNo ratings yet
- Design and Fabrication of Hybrid VehicleDocument4 pagesDesign and Fabrication of Hybrid VehicleRagbt CNo ratings yet
- Draka Power and InstrumentationDocument33 pagesDraka Power and Instrumentationnokaraju100% (1)
- Global Vaccine Action Plan: Tetanus & Difteri (TD/DPT)Document6 pagesGlobal Vaccine Action Plan: Tetanus & Difteri (TD/DPT)Gusti IndrakusumaNo ratings yet
- Pre-Extraction Records in Edentulous Patients - A Literature ReviewDocument6 pagesPre-Extraction Records in Edentulous Patients - A Literature ReviewMaywiNo ratings yet
- Datasheet Luxor 530W LX 530M 144 Bifacial HalfCell PERCDocument2 pagesDatasheet Luxor 530W LX 530M 144 Bifacial HalfCell PERCDimitarNo ratings yet