Download as docx, pdf, or txt
You might also like
- 45 Aesthetic Techniques For Lip TreatmentDocument33 pages45 Aesthetic Techniques For Lip TreatmentFritz Tumaneng100% (1)
- Soap NoteDocument2 pagesSoap Notetopopirate100% (4)
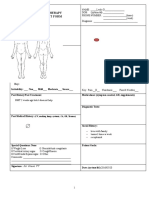
- Physical Therapy Amputee Assessment FormDocument4 pagesPhysical Therapy Amputee Assessment FormTopaz CompanyNo ratings yet
- Soap Note 5.0Document4 pagesSoap Note 5.0Paulus IskandarNo ratings yet
- 11 - Dot Phrase Templates HMC ED June 2017 - Rev 9.6.17Document13 pages11 - Dot Phrase Templates HMC ED June 2017 - Rev 9.6.17M100% (1)
- Physiologic Transition From Intrauterine To Extrauterine LifeDocument12 pagesPhysiologic Transition From Intrauterine To Extrauterine Lifeyhojar PisfilNo ratings yet
- Burnstrom, MRP Approaches For Neurological ConditionsDocument68 pagesBurnstrom, MRP Approaches For Neurological ConditionsSaba IqbalNo ratings yet
- CH7060 Manufacture and Clinical Trials of MedicinesDocument11 pagesCH7060 Manufacture and Clinical Trials of MedicinesjaweriaNo ratings yet
- Ortho ClerkingDocument4 pagesOrtho ClerkingNur Liyana Ahmad ZakiNo ratings yet
- CNMCH Intern Guide Ortho U-1Document13 pagesCNMCH Intern Guide Ortho U-1Sandip DasNo ratings yet
- Clinic Guidance Case History Form UCO Sep2017 FINALDocument4 pagesClinic Guidance Case History Form UCO Sep2017 FINALShaun TylerNo ratings yet
- OSCEDocument34 pagesOSCEsona67% (3)
- Clinical Reasoning For PT StudentDocument28 pagesClinical Reasoning For PT StudentCantoria Willa 2 PTNo ratings yet
- Sample TemplatesDocument153 pagesSample TemplatesRusty Kuule50% (2)
- UVA Surgical Clerkship Survival GuideDocument15 pagesUVA Surgical Clerkship Survival GuideNadiim Rajabalee100% (1)
- Knee ExaminationDocument12 pagesKnee ExaminationNILABHNo ratings yet
- Lab Activity Week 2Document3 pagesLab Activity Week 2Mary SotoNo ratings yet
- 1 - General PrinciplesDocument22 pages1 - General PrinciplesFlorin PanduruNo ratings yet
- ESR Follow-Up FormDocument2 pagesESR Follow-Up FormAflkjael JamaelNo ratings yet
- Flores - BSPT 1a - Activity 16 - Stacking ConesDocument5 pagesFlores - BSPT 1a - Activity 16 - Stacking ConesBrandon FloresNo ratings yet
- Aneurysm Bone Cyst of Proximal PhalynxDocument6 pagesAneurysm Bone Cyst of Proximal Phalynxhemanarasimha gandikotaNo ratings yet
- Format Askep KGD KritisDocument14 pagesFormat Askep KGD KritisRirin Alfiah RiantiNo ratings yet
- PN Day 1 ReqsDocument17 pagesPN Day 1 ReqsDoneva Lyn MedinaNo ratings yet
- Billable ElementsDocument18 pagesBillable Elementsheidel anneNo ratings yet
- Augtonovmtr Form CghciDocument14 pagesAugtonovmtr Form CghciKyle Albert EstoestaNo ratings yet
- Physical Therapy Assessment Form: Right Shoulder PainDocument2 pagesPhysical Therapy Assessment Form: Right Shoulder PainSen PerNo ratings yet
- Lab#1 Elbow/Forearm: Examination: PT761.02 M. Briggs PT, DPT, SCS, Atc 4Document8 pagesLab#1 Elbow/Forearm: Examination: PT761.02 M. Briggs PT, DPT, SCS, Atc 4msbriggsNo ratings yet
- Year 4 - Clinical Skills Sign-Off Sheet PDFDocument2 pagesYear 4 - Clinical Skills Sign-Off Sheet PDFShandev IndoiNo ratings yet
- Initial Evaluation LormaDocument8 pagesInitial Evaluation LormaVanessa Yvonne GurtizaNo ratings yet
- Assessment Chart (BK) - 20210618 - inIN - Google SheetsDocument2 pagesAssessment Chart (BK) - 20210618 - inIN - Google Sheetsamit.kumarNo ratings yet
- Asuhan Keperawatan Di Instalasi Gawat DaruratDocument5 pagesAsuhan Keperawatan Di Instalasi Gawat DaruratLatifah khusnul SugiartoNo ratings yet
- Asuhan Keperawatan Di Instalasi Gawat DaruratDocument5 pagesAsuhan Keperawatan Di Instalasi Gawat DaruratDyah PerwaNo ratings yet
- Asuhan Keperawatan Di Instalasi Gawat DaruratDocument5 pagesAsuhan Keperawatan Di Instalasi Gawat DaruratAnnaNo ratings yet
- Asuhan Keperawatan Di Instalasi Gawat DaruratDocument5 pagesAsuhan Keperawatan Di Instalasi Gawat DaruratrisaNo ratings yet
- Asuhan Keperawatan Di Instalasi Gawat DaruratDocument5 pagesAsuhan Keperawatan Di Instalasi Gawat DaruratRidha TiomantaNo ratings yet
- Sample Emg/Ncv Report - Normal StudyDocument5 pagesSample Emg/Ncv Report - Normal StudyPhysiotherapist AliNo ratings yet
- Uscg Nremt Skill SheetsDocument13 pagesUscg Nremt Skill SheetsJeffTabor100% (1)
- Moseley G L (2008) Distorted Body Image and Tactile Dysfunction in PatientsDocument5 pagesMoseley G L (2008) Distorted Body Image and Tactile Dysfunction in PatientsLiliana SantosNo ratings yet
- Laporan Operasi Spine 20231011 - VivoDocument18 pagesLaporan Operasi Spine 20231011 - VivoIrvan IrvanNo ratings yet
- Abdominal Hollowing ExercisesDocument8 pagesAbdominal Hollowing ExercisesKinesiología TalganteNo ratings yet
- Cardiovascular Exam (12 Minute) : Examiner - Student InteractionDocument6 pagesCardiovascular Exam (12 Minute) : Examiner - Student InteractionFate ChanNo ratings yet
- Clinical ModuleDocument6 pagesClinical ModuleNovee100% (1)
- Nov 30 Dec 2 Case Study Module 1Document7 pagesNov 30 Dec 2 Case Study Module 1Kristian Karl Bautista Kiw-isNo ratings yet
- Assessment Chart翻译微信renwyi0107Document40 pagesAssessment Chart翻译微信renwyi0107jhonyhoweNo ratings yet
- HA Lab SAS26 Putting It All TogetherDocument9 pagesHA Lab SAS26 Putting It All TogetherMathewNo ratings yet
- How Many Joints in The Hands and Wrists Should Included in A Score Radiologic Abnormalities Used To Assess Rheumatoid Arthritis?Document10 pagesHow Many Joints in The Hands and Wrists Should Included in A Score Radiologic Abnormalities Used To Assess Rheumatoid Arthritis?Devi PrilliantiNo ratings yet
- Example Exam Questions CCSDocument4 pagesExample Exam Questions CCSishanschneider00No ratings yet
- Post OpDocument6 pagesPost OpFrinkaWijayaNo ratings yet
- PT Visit NotesDocument6 pagesPT Visit NotesmothstacheNo ratings yet
- Hestining Yuniar Pratiwi - P07125119014 - Oral Care FormDocument8 pagesHestining Yuniar Pratiwi - P07125119014 - Oral Care Formhyuniar pratwNo ratings yet
- Assessment For Comon Script 2017-1Document6 pagesAssessment For Comon Script 2017-1Coman AndreiNo ratings yet
- CPSP IMM Orthodontics-Template For Treated Cases of CandidatesDocument36 pagesCPSP IMM Orthodontics-Template For Treated Cases of CandidatesMuhammad UzairNo ratings yet
- Skala NyeriDocument20 pagesSkala NyeripuspaNo ratings yet
- Musculoskeletal System Examination For Neck and Shoulder StiffnessDocument4 pagesMusculoskeletal System Examination For Neck and Shoulder StiffnessnyeeperNo ratings yet
- Funda HandoutsDocument16 pagesFunda HandoutsAlvin pagaduan (AceSnake)No ratings yet
- Sekolah Tinggi Ilmu Kesehatan "Artha Bodhi Iswara" (Stikes - Abi)Document7 pagesSekolah Tinggi Ilmu Kesehatan "Artha Bodhi Iswara" (Stikes - Abi)Lailatul SisiliahNo ratings yet
- Synoposis Kahkishan (Repaired) 2Document25 pagesSynoposis Kahkishan (Repaired) 2Politic FeverNo ratings yet
- Initial Evaluation For Spinal Cord Injury: in Partial Fulfillment of The Requirements For Clin Ed 1: Case ConferenceDocument35 pagesInitial Evaluation For Spinal Cord Injury: in Partial Fulfillment of The Requirements For Clin Ed 1: Case ConferenceAnne BorelaNo ratings yet
- Objective Assessment of Spinal Cord InjuryDocument25 pagesObjective Assessment of Spinal Cord InjuryYangNo ratings yet
- OSCE & OSPE Final PresentationDocument49 pagesOSCE & OSPE Final PresentationKrini Tandel100% (1)
- MRI of Degenerative Disease of the Spine: A Case-Based AtlasFrom EverandMRI of Degenerative Disease of the Spine: A Case-Based AtlasNo ratings yet
- 14 Benign Lesions of LarynxDocument80 pages14 Benign Lesions of LarynxAbhishek ShahNo ratings yet
- MS Definition and AnatomyDocument9 pagesMS Definition and Anatomyejikieru03No ratings yet
- Ppda Q1 Booklet FinalDocument62 pagesPpda Q1 Booklet FinalRinalyn Centino-BesoNo ratings yet
- Anatomy of LarynxDocument49 pagesAnatomy of LarynxenoNo ratings yet
- 5z-12-Shania Lee Digestive System ReportDocument6 pages5z-12-Shania Lee Digestive System Reportapi-254080761No ratings yet
- 1 PBDocument8 pages1 PBDewi SartikaNo ratings yet
- CPT Exam Prep WorkbookDocument63 pagesCPT Exam Prep WorkbookAmethyst Carey100% (2)
- Orthopedic NursingDocument22 pagesOrthopedic NursingNicole Anne ValerioNo ratings yet
- Class 9-Biology-Lesson 11-Sense Organs-EarDocument10 pagesClass 9-Biology-Lesson 11-Sense Organs-EarShlok JaiswalNo ratings yet
- Abdominal Assessment HA LectureDocument44 pagesAbdominal Assessment HA LectureKatrina BeltranNo ratings yet
- Gambaran Radiologi AtelektasisDocument40 pagesGambaran Radiologi AtelektasisRaymond Frazier100% (1)
- The Neuroscience of Language. On Brain Circuits of Words and Serial Order by Friedemann PulvermüllerDocument332 pagesThe Neuroscience of Language. On Brain Circuits of Words and Serial Order by Friedemann PulvermüllerMauricio Escobar CastañedaNo ratings yet
- Bingo Cards 2x2Document5 pagesBingo Cards 2x2Marta Pérez MadridNo ratings yet
- The Respiratory SystemDocument21 pagesThe Respiratory Systemhanatabbal19No ratings yet
- Throat Pharynx Adenoids ENT LecturesDocument33 pagesThroat Pharynx Adenoids ENT LecturesRaju GangadharanNo ratings yet
- HarnMaster - Gold Character PortfolioDocument6 pagesHarnMaster - Gold Character PortfolioDDTWilsonNo ratings yet
- Effectiveness of The Teacher-Made SciencDocument4 pagesEffectiveness of The Teacher-Made SciencElaDonatoAriolaNo ratings yet
- Types of Reconstructive & Cosmetic SurgeryDocument28 pagesTypes of Reconstructive & Cosmetic SurgerySimon Josan100% (1)
- The Effect of Exercise On The Cardiorespiratory SystemDocument15 pagesThe Effect of Exercise On The Cardiorespiratory SystemBASAVARAJ100% (1)
- Auric Recon Slides 070516Document92 pagesAuric Recon Slides 070516Yudhistira AdeNo ratings yet
- Epithelial Tissue - Overview PDFDocument9 pagesEpithelial Tissue - Overview PDFAslak TorgersenNo ratings yet
- P Brachialis 2Document2 pagesP Brachialis 2jessgabNo ratings yet
- Muscular SystemDocument41 pagesMuscular SystemGem Rose UretaNo ratings yet
- NCM 116 Lecture ENDOCRINE Pituitary Gland Thyroid Gland DisordersDocument4 pagesNCM 116 Lecture ENDOCRINE Pituitary Gland Thyroid Gland DisordersMeryville JacildoNo ratings yet
- Ropa Running Compresión 2XU Catálogo 2014Document43 pagesRopa Running Compresión 2XU Catálogo 2014Mayayo: Carrerasdemontana.comNo ratings yet
- Muscle GroupsDocument25 pagesMuscle GroupsRoxana LorenteNo ratings yet
- 24 Digestive SystemDocument52 pages24 Digestive SystemkikiNo ratings yet