Professional Documents
Culture Documents
Epidemiology and Pathophysiology of MS
Epidemiology and Pathophysiology of MS
Uploaded by
David EduardoCopyright
Available Formats
Share this document
Did you find this document useful?
Is this content inappropriate?
Report this DocumentCopyright:
Available Formats
Epidemiology and Pathophysiology of MS
Epidemiology and Pathophysiology of MS
Uploaded by
David EduardoCopyright:
Available Formats
REVIEW ARTICLE
Epidemiology and
C O N T I N UU M A UD I O
I NT E R V I E W A V AI L A B L E
ONLINE
Pathophysiology of
Multiple Sclerosis
By Melanie Ward, MD; Myla D. Goldman, MD, MSc, FAAN
CITE AS:
CONTINUUM (MINNEAP MINN)
2022;28(4, MULTIPLE SCLEROSIS
ABSTRACT
AND RELATED DISORDERS):988–1005.
PURPOSE OF REVIEW: This article provides an overview of genetic,
Address correspondence to environmental, and lifestyle risk factors affecting the disease course of
Dr Melanie Ward, One Medical multiple sclerosis (MS) and reviews the pathophysiologic characteristics of
Center Dr, Ste 1310, Morgantown,
WV 26506, mward9@hsc.wvu.edu.
both relapsing and progressive MS.
RELATIONSHIP DISCLOSURE: RECENT FINDINGS: The prevalence of MS has increased in recent decades,
Dr Ward has received personal
compensation in the range of and costs of care for patients with MS have risen dramatically. Black,
$500 to $4999 for serving as a Asian, and Hispanic individuals may be at risk for more severe MS-related
consultant for Bristol-Myers disability. Multiple genetic MS risk factors have been identified. Factors
Squibb Company, Celgene
Corporation, EMD Serono, such as low vitamin D levels and a history of Epstein-Barr virus, smoking,
Genentech, Inc, and Novartis AG. and obesity, especially during childhood, also influence MS risk.
The institution of Dr Ward has
received research support from
Traditionally thought to be a T-cell–mediated disease, recent research has
Genentech, Inc. Dr Goldman has highlighted the additional roles of B cells and microglia in both relapsing
received personal compensation and progressive MS.
in the range of $500 to $4999 for
serving as a consultant for
Greenwich Biosciences, Inc, SUMMARY: Complex interactions between genetic, environmental, and
Merck & Co, Inc, and Novartis AG lifestyle factors affect the risk for MS as well as the disease course. People
and as a data safety monitoring
board member for BrainStorm of color have historically been underrepresented in both MS clinical trials
Cell Limited; has received and literature, but current research is attempting to better clarify unique
personal compensation in the
considerations in these groups. MS pathology consists of the focal
range of $5000 to $9999 for
serving as a consultant for inflammatory lesions that have been well characterized in relapsing MS, as
Biogen, EMD Serono, Inc, well as a more widespread neurodegenerative component that is posited
Genentec, Inc, Immunic
Therapeutics, and Sanofi; and
to drive progressive disease. Recent advances in characterization of both
has received personal the inflammatory and neurodegenerative aspects of MS pathophysiology
compensation in the range of have yielded potential targets for future therapeutic options.
$10,000 to $49,999 for serving as
a consultant for Adamas
Pharmaceuticals, Inc.
UNLABELED USE OF INTRODUCTION
M
PRODUCTS/INVESTIGATIONAL ultiple sclerosis (MS) is an autoimmune demyelinating disease
USE DISCLOSURE:
of the central nervous system (CNS) with both inflammatory
Drs Ward and Goldman discuss
the unlabeled/investigational and neurodegenerative components and is the most common
use of rituximab, Bruton tyrosine nontraumatic disabling neurologic condition in young adults.1,2
kinase inhibitors, and vitamin D
supplementation for the
Although initial disease descriptions date to hundreds of
treatment of multiple sclerosis. years ago, therapeutic options were limited until the past several decades.
Unprecedented advances in understanding pathogenesis and treatment of MS
© 2022 American Academy have occurred in recent years, and this article reviews both historical descriptions
of Neurology. of MS as well as current understanding of disease expression and pathophysiology.
988 AUGUST 2022
Copyright © American Academy of Neurology. Unauthorized reproduction of this article is prohibited.
Particular attention is paid to populations that have been traditionally KEY POINTS
underrepresented in MS literature.
● The prevalence of
multiple sclerosis (MS) is
HISTORICAL PERSPECTIVE increasing, potentially
because of changes to
Early descriptions of possible MS date to the Middle Ages. Lidwina of Schiedam,
diagnostic criteria that allow
Holland, was born in 1380, and at age 16, she had a fall with subsequent gait for earlier diagnosis, more
impairment. She later developed facial pain possibly representative of trigeminal widespread use of MRI, and
neuralgia, progressive visual impairment, weakness, dysphagia, and difficulty population aging.
walking with few periods of remission. At the time, Lidwina’s affliction was
● Female predominance in
thought to come from God, and she was ultimately canonized in 1890.3 Diary MS has persisted over time,
entries from Augustus d’Este, grandson of King George III of England, are also with a female to male ratio
considered to be one of the first reported MS cases. In the 1800s, he maintained of approximately three to
detailed records of his struggles with initial relapsing symptoms, including one.
possible optic neuritis at age 28. Attempts at treatment included blood-letting,
dietary changes, and massage. After several focal, remitting events, he developed
a more progressive course that resulted in paralysis, marked spasticity, and death
by age 54.4
Jean-Martin Charcot detailed comprehensive clinical and pathophysiologic
descriptions of MS in the 1860s, and his reports included autopsy findings from
one of his own employees who developed progressive motor dysfunction.3 More
than 120 years after Charcot’s initial pathologic descriptions, the first
disease-modifying therapy (DMT) for MS was approved.3
PREVALENCE
The prevalence of MS in the adult population in the United States was estimated
at 309 per 100,000 population in 2010, and the extrapolated prevalence in 2017
was 337 to 362 per 100,000 population.1 This translates to more than 900,000
individuals living with MS in the United States.1 In contrast, estimated
prevalence in 1990 was 58 per 100,000, with an estimated 300,000 total US
patients.1 Female predominance, with a female to male ratio of approximately
three to one has held steady in this time period1 and persists across racial
populations.5,6 Several factors may contribute to increased MS prevalence,
including widespread access to MRI, changes to diagnostic criteria allowing for
diagnosis earlier in disease presentation, and population aging accompanied by
longer survival.1
PATHOPHYSIOLOGY OF MULTIPLE SCLEROSIS
Normally, CNS autoreactive immune cells are deleted during development
through central tolerance in the thymus (T cells) or bone marrow (B cells).
Although some may escape this mechanism and be released into the circulation,
peripheral tolerance mechanisms typically prevent them from causing disease.
Mechanisms by which peripheral tolerance can fail include impaired regulatory T
cell (Treg) function or resistance of autoreactive cells to suppression. A complex
interplay between genetic and environmental risk factors may influence function
and activation of these autoreactive cells and lead to disease pathogenesis.
Primary T cell subsets implicated in MS include CD8+ T cells and CD4+ T helper
(TH) 1 and TH17 cells.7 Autoreactive T cells also produce cytokines that may
contribute to MS pathogenesis including interferon gamma, interleukin (IL)-17,
and granulocyte-macrophage colony-stimulating factor.8 Efficacy of some MS
CONTINUUMJOURNAL.COM 989
Copyright © American Academy of Neurology. Unauthorized reproduction of this article is prohibited.
MS EPIDEMIOLOGY AND PATHOPHYSIOLOGY
DMTs may at least partially relate to shifting T cell differentiation from TH1 and
TH17 to TH2 phenotypes, which have a less inflammatory profile.7
Although MS was historically thought to be a primarily T cell–driven disease,
the role of B cells in MS pathophysiology has been increasingly recognized and
characterized in recent years. CSF-specific oligoclonal IgG bands are antibodies
produced by B cells and have long been included in MS diagnostic criteria,9 and
peripheral B cells play a variety of roles in the pathophysiology of MS. In MS, B
cells produce proinflammatory cytokines including lymphotoxin-α, IL-6, TNF-α,
and granulocyte-macrophage colony-stimulating factor. In turn, B-cell depletion
can attenuate proinflammatory activity of CD4+ and CD8+ T cells.9,10 Normally,
B cells can also generate anti-inflammatory cytokines including IL-10, IL-35, and
transforming growth factor β1, but the production of these in patients with MS
may be impaired.9 Interestingly, higher levels of IL-10–producing B cells were
previously found in patients with MS with concurrent helminth infections, and
this correlated with lower MS disease activity.11
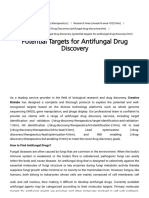
FIGURE 1-1
Microglial involvement in neurodegeneration in multiple sclerosis (MS). Microglia and
macrophages release many cytokines, including tumor necrosis factor (TNF)-α, and interleukin
(IL)-1β, which may contribute to neurodegeneration via cytokine-induced cell death, inhibition
of astrocytic glutamate reuptake, and the induction of dysfunctional RNA-binding proteins.
Microglia and macrophages can also release glutamate, potentially contributing to glutamate
excitotoxicity and neurodegeneration. Lastly, microglia and macrophages release reactive
oxygen species/reactive nitrogen species, which may contribute to neurodegeneration by
inducing oxidative stress and mitochondrial injury. Microglia can also express anti-inflammatory
phenotypes, which may contribute to remyelination, and much remains to be determined
regarding the definitive pathophysiologic mechanisms underlying neurodegeneration in MS.
Modified from Kamma E, et al, J Neuroinflamm.17 © 2022 The Authors.
990 AUGUST 2022
Copyright © American Academy of Neurology. Unauthorized reproduction of this article is prohibited.
Within the CNS, inflammatory B-cell infiltrates can be found in the meninges KEY POINTS
of patients with MS, and a higher burden of these infiltrates correlates with the
● Autoreactive T cells are
degree of cortical lesions and neurodegeneration as well as clinical disability.9,12 involved in MS pathogenesis
B cells may also act as a reservoir for Epstein-Barr virus (EBV), which is further and were traditionally felt
discussed in a subsequent section of this article. Other pathologic mechanisms to be the primary
involving B cells in MS include antigen presentation to T cells and secretion of disease-driving immune
subset. B cells have been
molecules that may be directly toxic to oligodendrocytes.9,13 B cell–depleting
increasingly recognized as
agents have emerged as effective DMTs and are now widely used in MS treatment. important in MS
Currently used agents are monoclonal antibodies to CD20, a protein expressed by pathophysiology as well,
several subtypes of B cells, and include rituximab, ocrelizumab, and ofatumumab. likely through multiple
mechanisms.
Ocrelizumab is also the only DMT currently approved by the US Food and Drug
Administration (FDA) for treatment of primary progressive MS (PPMS).9 ● Microglia are immune
Microglia are immune cells residing in the CNS and can shift between both cells residing in the central
pro- and anti-inflammatory phenotypes.2 Microglia have previously been nervous system and are
implicated in genetic leukoencephalopathies and neurodegenerative diseases and involved in both active and
chronic MS lesions. Several
are increasingly recognized in MS pathophysiology. Microglia contribute to both therapeutic agents
acute and chronic lesion formation in MS and, on the opposite spectrum, can also potentially targeting
facilitate remyelination and neuronal repair.2,14,15 In early active MS lesions, microglia are in
about 40% of phagocytic cells are proinflammatory microglia.15 Activated development.
microglia and CD8+ T cells lead to myelin destruction; recruitment of B cells,
● Compared with the acute
other T cells, and macrophages; axon damage; and disruption of the blood-brain inflammatory lesions that
barrier.16 Activated microglia are also found in the periphery of mixed active/ characterize relapsing MS,
inactive (also called chronic, slowly expanding, or smoldering) lesions, whereas chronic, inactive, and
cortical lesions and
inactive lesions demonstrate more axonal loss and less microglia.2,14 In
more widespread
progressive MS, activated microglia and macrophages may mediate neurodegeneration
neurodegeneration by several mechanisms including cytokine release, glutamate may predominate in
release resulting in excitotoxicity, and release of reactive oxygen/nitrogen species progressive MS.
resulting in oxidative injury (FIGURE 1-1).17 Consequently, interest has increased
in therapeutic agents potentially targeting microglia. Bruton tyrosine kinase is
expressed in B cells and in CNS microglia, and several therapeutic agents
targeting inhibition of Bruton tyrosine kinase are currently in clinical trials for
both relapsing and progressive MS.2
Relapsing MS is primarily characterized by acute inflammatory activity
associated with disruption of the blood-brain barrier, as evidenced by
gadolinium-enhancing lesions on MRI.16,18 Classic acute lesions begin with
infiltrates of inflammatory B, T, and plasma cells and macrophages surrounding
a central vein.19 As discussed, proinflammatory microglia are also present in
acute lesions.16 In addition to demyelination, axonal and neuronal injury also
occurs within acute lesions.19 As lesions evolve, remyelination occurs in varying
degrees and may be partially mediated by anti-inflammatory microglia.20
Previously felt to be a predominantly white matter disease, cortical and deep gray
matter involvement have now been well characterized in all subtypes of MS and
have been associated with disability progression.21-23
Although relapsing MS is primarily influenced by peripheral immune
responses targeting the CNS, progressive forms of MS may be more heavily
driven by intrinsic immune processes within the CNS behind an apparently
intact blood-brain barrier.16,24,25 Although active/enhancing lesions can occur in
progressive disease, studies indicate that slowly expanding, inactive, and
remyelinated shadow plaques, as well as cortical lesions, may be more
abundant.16 Other mechanisms contributing to neurodegeneration in progressive
CONTINUUMJOURNAL.COM 991
Copyright © American Academy of Neurology. Unauthorized reproduction of this article is prohibited.
MS EPIDEMIOLOGY AND PATHOPHYSIOLOGY
MS may include chronic microglial activation (even in normal-appearing white
matter), impaired ion homeostasis, mitochondrial injury, and meningeal
inflammation.16,24 Characteristics of meningeal involvement appear to differ
between PPMS and secondary progressive MS (SPMS). In SPMS lymphoid
follicles consisting of B and T lymphocytes, macrophages, and plasma cells are
frequently found in the meninges and perivascular spaces, whereas meningeal
inflammation in PPMS is more diffuse without the presence of follicles.17,24
Compared with relapsing MS, spinal cord lesion load has been demonstrated to
be higher in progressive MS and, in combination with spinal cord gray matter
atrophy, correlates with disability severity in progressive MS.24,26,27 Although
understanding of both the shared and distinct features of progressive MS has
increased markedly, much remains yet to be elucidated regarding the definitive
pathophysiology of progressive MS.17 In addition, while relapsing and
progressive MS have been characterized as distinct phenotypes clinically,
expanding research indicates that features of both the inflammatory and
neurodegenerative processes in MS exist in parallel across varying disease
subtypes.19
RISK FACTORS
Studies in MS have identified several environmental, lifestyle, and genetic risk
factors relevant in both the risk of MS disease onset and course following
diagnosis.
Ultraviolet Radiation and Vitamin D
The prevalence of MS increases in a geographic gradient, with a higher
prevalence occurring in northern regions.1 Proposed reasons for this geographic
gradient include exposure to ultraviolet B (UVB) radiation and vitamin D. Living
in areas with high ambient UVB and increased summer sun exposure during
childhood is associated with decreased risk of MS.28,29 UVB exposure may also
influence MS risk independently of vitamin D.30
In humans, vitamin D is obtained via UVB-induced production in skin or
dietary intake through vitamin D–rich foods or supplementation. Vitamin D–rich
foods include fatty fishes (such as salmon, tuna, mackerel, and trout), some
mushrooms, and egg yolks.31-33 However, few foods contain significant amounts
of vitamin D, and dietary intake alone is often insufficient to meet total needs.32
Vitamins D3 (cholecalciferol, synthesized in skin via UVB-mediated production)
and D2 (ergocalciferol, found in plant sources of vitamin D) are metabolized to
25(OH)D3 and then ultimately to 1,25(OH)2D3, the active metabolite.32 In innate
immune cells, vitamin D may enhance pathogen elimination and immune
tolerance. Effects of vitamin D in adaptive immune cells include inducing
differentiation to regulatory T and B cells, decreased production of
proinflammatory cytokines, and increased secretion of anti-inflammatory
cytokines.31 In addition to these potential immunomodulatory effects, direct
effects of vitamin D on neural cells have also been observed, including promoting
oligodendrocyte maturation.34
Multiple studies have demonstrated associations between low vitamin D levels
and increased MS risk.31,35,36 Low vitamin D has also been associated with
increased risk of conversion from clinically isolated syndrome (CIS) to clinically
definite MS37 and increased risk of MS relapse.31,38,39 Exact mechanisms by which
vitamin D contributes to MS are multifactorial and are also likely influenced by
992 AUGUST 2022
Copyright © American Academy of Neurology. Unauthorized reproduction of this article is prohibited.
other genetic and environmental risk factors.31 For example, genetic KEY POINT
polymorphisms in the vitamin D pathway have been associated with both serum
● Low vitamin D levels are
vitamin D levels and relapse rates in pediatric MS patients,39 and vitamin D and associated with an
its associated receptors may interact with EBV nuclear antigens to contribute to increased risk of MS.
MS pathogenesis.34 Finally, lower increases in serum vitamin D levels after Current trials aim to clarify
supplementation have been observed in patients with MS compared with the role of supplementation
and vitamin D goal levels in
controls, suggesting that in patients with MS vitamin D metabolism may also
patients with MS.
be altered.40
Despite mounting evidence regarding the relationship between low vitamin D
levels and the risk of MS and MS relapse, data are mixed regarding efficacy of
vitamin D supplementation on clinical and radiographic outcome measures.41 To
date, studies have been limited by small sample sizes, short durations, and
concurrent use of DMTs, which may have confounded results.31,42 Recent
meta-analyses have not clearly identified benefits of vitamin D in the treatment
of MS.41,42 Larger, more sufficiently powered studies are underway and will
hopefully provide clearer evidence regarding the role of vitamin D
supplementation in both MS and CIS.43,44
Risks of vitamin D toxicity include hypercalcemia, hyperphosphatemia,
hypercalciuria, and renal failure. Most trials evaluating the effects of vitamin D
supplementation in MS excluded patients with contraindications for high-dose
vitamin D supplementation, including renal impairment, granulomatous disease,
and primary hyperparathyroidism.31 Otherwise, for most adults, risks of vitamin
D supplementation are low, and toxicity typically does not occur in levels less
than 150 ng/mL.32,45 While awaiting results of more definitive trials regarding the
role of supplementation, assessing vitamin D status in patients with CIS and MS
is often considered reasonable in clinical practice. The following discussion
regarding clinical assessment of vitamin D refers to serum 25(OH)D3 level, as this
is most representative of total body stores and is most often measured in clinical
practice.31 Consensus has not been reached regarding goal vitamin D levels and
optimal supplement dosing in patients with MS. In the general adult population,
Endocrine Society guidelines suggest that vitamin D levels of 30 ng/mL are
sufficient.46 At least 1500 international units (IU) to 2000 IU daily of
supplemental vitamin D may be needed to maintain these levels, with some
patients requiring higher doses.46 Some MS specialists recommend a goal vitamin
D level of 40 ng/mL to 60 ng/mL, which may require even higher dosing
(2000 IU to 5000 IU daily).47 For patients with MS, repeat monitoring of vitamin
D levels is suggested 3 months after starting supplementation to direct further
dose adjustments.47
Genetics
The human leukocyte antigen (HLA) complex contains multiple genes related to
immune system functioning, and HLA genotype has been increasingly well
characterized regarding MS risk.48 HLA-DRB1*15:01 is associated with increased
risk of MS and is present in up to 30% of the population in the United States and
northern Europe.49 HLA-A*02 is associated with decreased MS risk.48 Many
other normal-variant single nucleotide polymorphisms, which are located
outside the HLA complex but typically near genes associated with immune
functions, have also been associated with MS risk to varying degrees.48,49
Combinations of genetic factors also likely contribute to disease risk; for
example, the presence of HLA-DRB1*15:01 and the lack of HLA-A*02 are
CONTINUUMJOURNAL.COM 993
Copyright © American Academy of Neurology. Unauthorized reproduction of this article is prohibited.
MS EPIDEMIOLOGY AND PATHOPHYSIOLOGY
associated with higher risk of MS than the presence of HLA-DRB1*15:01 alone.48
Gene–environmental interactions that may contribute to MS pathogenesis
include vitamin D levels,39 obesity in childhood,50 EBV infection,49 and
smoking.48 However, in clinical practice, testing for genetic variants associated
with MS risk is not currently recommended even in patients with a family history
of MS.49
Epstein-Barr Virus
EBV is a herpes virus frequently acquired in childhood and is often
asymptomatic. Later-onset infection in adolescence and adulthood is more
commonly associated with clinical illness manifesting as infectious
mononucleosis.51 Following infection, latent EBV remains in host B
lymphocytes.52 Across multiple meta-analyses, EBV antibody seropositivity and
infectious mononucleosis have consistently been associated with MS risk.53 Even
more definitively, a recent large study by Bjornevik and colleagues52 indicated
that MS is almost always preceded by EBV infection and that EBV may be a
primary cause of MS. That being said, EBV seropositivity is high not only in
patients with MS but also in the general population; thus, the role of EBV in MS
pathogenesis is likely multifactorial and may include interactions between EBV,
predisposing genetic factors, and environmental risk factors.49,54
EBV nuclear antigen 1 (EBNA1) is expressed in EBV-infected B cells and
contributes to transcription regulation and viral genome maintenance.54
Proposed mechanisms by which EBV may contribute to MS pathogenesis include
molecular mimicry between EBNA1 and glial cell adhesion molecules expressed
by CNS oligodendrocytes and astrocytes resulting in cross-reactive antibodies.55
In human tissue studies, a significantly higher number of EBV-related proteins
were present in chronic MS lesions compared with non-MS controls, and 85% of
patients with MS had EBV-encoded RNA-positive B cells in their brains
compared with rare occurrence in control brains.56 In another study, EBV
infection was also demonstrated directly in astrocytes and microglia of patients
with MS and was not solely confined to B cells.57
Several other potential viral contributors to MS risk, including human herpes
virus 6, cytomegalovirus, herpes simplex virus, and human endogenous
retroviruses, have been explored, but thus far have less well-established
associations with MS pathogenesis than EBV.49
Smoking
Smoking has been associated with increased risk of MS,58 as well as
conversion from CIS to clinically definite MS33 and conversion of relapsing
to secondary progressive MS.59,60 Smoking may also reduce efficacy of at
least some DMTs including interferon and natalizumab.61,62 Passive smoke
exposure has also been associated with increased MS risk.48 Interestingly, use
of oral tobacco has been associated with decreased risk of MS, suggesting that
lung inflammation from smoking may be the driver of increased MS risk
in smokers.48
Genetic factors may influence the effect of smoking on MS risk. For example,
one Swedish study found that among patients who had HLA-DRB1*15:01 and
lacked HLA-A*02, smoking contributed to development of MS in 41% of cases.63
This illustrates the importance of smoking, including passive exposure, as a
modifiable risk factor both for disease development and disease course in MS.
994 AUGUST 2022
Copyright © American Academy of Neurology. Unauthorized reproduction of this article is prohibited.
Small studies indicate that patients are often unaware of the MS-specific risks of KEY POINTS
smoking and that education by MS clinicians and referral to quit support services
● Human leukocyte antigen
may be an opportunity for improvement in clinical practice.64,65 (HLA)-DRB1*15:01 genotype
increases MS risk, whereas
Obesity HLA-A*02 may be
Obesity in adolescence and childhood has been associated with increased risk protective. Other single
nucleotide polymorphisms
of both pediatric and adult-onset MS, with a seemingly stronger association
influencing MS risk have also
in females compared with males.66,67 In pediatric patients, obesity may been identified.
precede MS diagnosis by several years.67 Abdominal obesity has also been
associated with more severe disability in patients with known MS.68 Proposed ● Epstein-Barr virus
mechanisms by which obesity may be involved in MS pathogenesis seropositivity and infectious
mononucleosis are
include promotion of a proinflammatory milieu,48 decreased vitamin D associated with increased
bioavailability,48 and interactions with predisposing genetic MS risk factors50 risk of MS. Other viral
and EBV infection.69 associations with MS have
been less clearly defined.
Microbiome and Diet ● Smoking, including
The human body contains more microbial cells than human cells, and most passive smoke exposure,
human microbes reside in the gut. Gut colonization in early life is influenced by a has been associated with
variety of factors including method of delivery, breastfeeding, antibiotic both MS risk and disease
progression. Smoking
exposure, and genetic, environmental, and maternal factors. Diet significantly
cessation should be
influences microbiome composition throughout the remainder of an individual’s encouraged, and dedicated
life.70-72 Species of Bacteroides and Firmicutes within the gut use indigestible fiber education by clinicians may
and complex carbohydrates to produce short chain fatty acids that can ultimately increase the likelihood of
cessation.
increase production of regulatory T cells important in suppressing autoreactive
immune cells in MS.71,73 Bacteria can also produce cytokines that can influence ● Childhood and
both pro- and anti-inflammatory immune cells.71 Multiple studies have adolescent obesity have
demonstrated differing gut microbiomes in patients with MS compared with been associated with
controls, although exact bacterial compositions have been mixed.71 Much increased MS risk, and
abdominal obesity has also
remains to be determined regarding the exact role of diet in MS pathogenesis and been associated with a
disease course, and a unifying ideal MS diet has not been established. To date, degree of MS-related
studies have primarily evaluated the influence of diets high in vegetables, fruits, disability.
and whole grains and limited in the amounts of fats and animal products on both
● Gut microbiome may
microbiome composition and clinical outcomes. Consistent associations between
influence systemic
diet, relapse rate, and disability progression in MS have not been demonstrated, inflammation. A unifying
but there have been some associations between diet quality and symptomatic “MS microbiome” has not
issues such as fatigue and depression.74-77 been demonstrated, and the
role of diet in MS outcomes
has yet to be clearly
Comorbidities and Multiple Sclerosis Disease Course defined, but a higher quality
Comorbid conditions are common in patients with MS and increase with age.78 diet may assist in improving
Comorbid conditions can contribute to delays in MS diagnosis and treatment common symptomatic
initiation79 and adversely affect health-related quality of life.80 At the time of MS issues.
diagnosis, common comorbidities include depression, anxiety, hypertension,
chronic lung disease, and hyperlipidemia.81 Vascular comorbidities (including
hypertension, hyperlipidemia, diabetes, and peripheral vascular disease) and
obstructive lung disease have been associated with disability progression in
MS.82,83 Psychiatric comorbidities, including anxiety and mood disorders, have
been associated with relapse risk,78 disability progression,84 and adherence to MS
treatments.85,86 Many patients with MS have more than one comorbidity, and the
cumulative number of comorbid conditions that a patient has may increase their
risk of relapse78 and has been associated with higher disability scores.87
CONTINUUMJOURNAL.COM 995
Copyright © American Academy of Neurology. Unauthorized reproduction of this article is prohibited.
MS EPIDEMIOLOGY AND PATHOPHYSIOLOGY
Comorbidities may also affect treatment decisions, response, and adherence in
patients with MS.88,89
Potentially modifiable MS risk factors are summarized in TABLE 1-1.
POPULATIONS OF SPECIAL INTEREST
Recognition and understanding of specific subgroups within the MS community
have increased in recent years.
Race-specific Considerations
Data regarding people of color have historically been underrepresented in the MS
literature.90 MS has long been considered to predominantly affect White people
of Northern European ancestry, but this assumption has been challenged in
recent demographic data. Studies suggest a higher incidence of MS in the US
Black population than previously characterized (CASE 1-2) and up to a 47%
higher risk of MS in Black women compared with White women in the US.6,91,92
Black patients are more likely than White patients to present with multifocal
symptoms, more frequently develop transverse myelitis, and may have worse
visual impairment from acute optic neuritis and more rapid retinal nerve fiber
loss leading to greater vision dysfunction.5,93,94 Rates of relapsing versus
progressive disease are similar between Black patients and White patients.5 MS
occurs more frequently in Black Americans than Africans, which may relate to
TABLE 1-1 Potentially Modifiable Multiple Sclerosis Risk Factors
Risk factor Association in multiple sclerosis Interventions in clinical practice
Vitamin D Increased risk of multiple sclerosis (MS)/clinically Consider assessing serum total vitamin D level for
deficiency isolated syndrome (CIS)31,35,36 patients with MS/CIS
Increased risk of MS relapse31,38,39 Definitive goal level for patients with MS not yet
established; Endocrine Society guidelines
recommend goal level of 30 ng/mL for the general
population,46 and some MS specialists recommend
goal level of 40-60 ng/mL47
Smoking Associated with increased risk of MS/CIS58,60 Encourage cessation and educate patients regarding
and increased risk of disease progression59,60 MS-specific smoking risks, consider referral to
smoking cessation support services64,65
Obesity Childhood/adolescent obesity associated with Counsel patients regarding MS-specific obesity
increased MS risk66,67 concerns, encourage healthy weight67
Abdominal obesity associated with worse MS
disability67
Diet and Gut microbiome may contribute to systemic Discuss potential role of higher quality diet in MS
microbiome inflammation71,73 symptom management
Unifying ideal MS diet has not yet emerged, but
diet may contribute to symptom management74-77
Comorbid Systemic and psychiatric comorbidities may Inform patients of importance of managing
conditions contribute to relapse risk,78 degree of disability,84,87 comorbidities
and adherence to treatment85,86
996 AUGUST 2022
Copyright © American Academy of Neurology. Unauthorized reproduction of this article is prohibited.
differences in both genetic and environmental risk factors.5 Black patients may KEY POINTS
develop earlier ambulatory dysfunction, requiring cane assistance several years
● Comorbid conditions are
earlier than White patients.5 Disability owing to hand and visual dysfunction is common in patients with
more common in Black patients compared with White patients,95 and more MS. Comorbidities influence
severe cognitive processing involvement has been demonstrated in Black relapse risk, disability
patients with MS, as well.96 Higher lesion burden and accelerated rates of both scores, health-related
quality of life, and treatment
brain volume loss and retinal atrophy in Black patients may contribute to greater
adherence.
accumulation of disability.96,97
Compared with White and Black patients, Asian, Native American, and ● The incidence of MS is
Hispanic patients appear to have a lower incidence of MS.6,91,92,95 Adult Hispanic higher than previously
people with MS tend to have a younger age of disease onset compared with recognized in Black people
in the United States, and
White and Black patients.6 Among Hispanic immigrants to the United States, Black, Asian, and Hispanic
immigration before adolescence was associated with younger age at MS onset patients may be at risk for
compared with later immigrants and hints at a potential role of age-dependent more severe disability
environmental risk factors in disease pathogenesis. Later age at immigration has related to MS.
been associated with worse disability in Hispanic patients.98 Hispanic patients may ● Among Hispanic
be more likely to present with optic neuritis (at least in patients from the western immigrants to the United
United States),93,99,100 may more frequently develop transverse myelitis,93,100 and States, immigration before
may have a more aggressive disease course compared to White patients.101 adolescence has been
associated with younger age
Historical data suggest that, similar to Black and Hispanic patients with MS,
at MS onset, and later
Asian patients with MS are at higher risk of optic nerve and spinal cord immigration has been
involvement compared with White patients, which may lead to more significant associated with worse
ambulatory disability.93 However, it is important to note that some of these data disability.
were obtained before formalized diagnostic criteria and antibody testing for
neuromyelitis optica spectrum disorders (NMOSD) as separate disease entities
from MS. Therefore, regardless of race, it is important to consider and evaluate
for alternative diagnoses (eg, NMOSD) in patients presenting with predominantly
optic nerve and spinal cord disease involvement to guide appropriate treatment
decision making.93
Few data are available regarding MS in Native Americans, but Native
American ancestry has been associated with risk of optic neuritis as a presenting
symptom in Hispanic patients,102 as well as increased risk of neuromyelitis optica
in Mexican populations.103
Disparities in care across racial backgrounds have been demonstrated for
several chronic neurologic conditions, including MS. One US study found that
Black and Hispanic patients with MS were less likely than White patients to see a
neurologist.104 Treatment responses to DMT between White patients and
patients of color may also differ; prior studies have suggested lower response to
interferon therapies in Black patients.105 The ability to draw race-specific
conclusions about DMT efficacy in patients of color has been limited by
disproportionately small numbers of participants of color enrolled in clinical
trials.106,107 Ongoing research will hopefully yield better understanding of
race-specific considerations in MS pathogenesis, disease course, and treatment
optimization, including in subpopulations of racial and ethnic cohorts that are
often grouped together but have varying ancestral genetic admixtures.98,100
LGBTQAI Populations
Limited data exist regarding lesbian, gay, bisexual, transgender, queer (or
questioning), asexual (or allied), and intersex (LGBTQAI)-specific
considerations in MS. In a prior analysis of 5604 patients with MS enrolled in the
CONTINUUMJOURNAL.COM 997
Copyright © American Academy of Neurology. Unauthorized reproduction of this article is prohibited.
MS EPIDEMIOLOGY AND PATHOPHYSIOLOGY
North American Research Committee on Multiple Sclerosis registry, 95.4% of
patients identified as heterosexual and 4.6% of patients identified as lesbian, gay,
or other sexual orientation (see the article by Khayambashi and colleaguees108 for
the full description of available responses in this survey). Patients who identified
as lesbian, gay, or another orientation were less likely to report that their provider
knew their sexual orientation and were less comfortable discussing sexual health
with their providers. In the same study, 0.45% of patients identified as
CASE 1-2 A 53-year-old man presented with a 1-year history of progressively
worsening gait, muscle stiffness, incomplete urinary emptying, and
cognitive difficulty without discrete focal events. He had experienced
daytime fatigue and physical lassitude for approximately 3 years prior to
onset of his other neurologic symptoms. He had a history of smoking.
Examination revealed increased tone in his lower extremities, spastic
gait, and hyperreflexia. Brain MRI revealed periventricular, subcortical, and
juxtacortical lesions in a pattern consistent with multiple sclerosis (MS)
(FIGURES 1-2A and 1-2B). MRI of his cervical and thoracic spine also revealed
demyelinating lesions (FIGURE 1-2C). No lesions enhanced with contrast. His
vitamin D level was low at 28 ng/mL (normal ≥30). He was Black.
One year of progressive neurologic symptoms, characteristic lesions on
brain and spinal cord MRI, and no other more likely diagnosis met criteria for
a diagnosis of primary progressive multiple sclerosis, and lumbar puncture
was not completed. He stopped smoking shortly after diagnosis. He was
treated with B cell–depleting therapy with clinical stabilization. Repeat
vitamin D level following initiation of supplementation was 41 ng/mL.
COMMENT Recent studies suggest that the incidence of MS in Black patients in the
United States is higher than previously characterized and similar to the
incidence in White patients. Black patients may be more likely to have visual
and spinal cord disease involvement and may develop ambulatory
dysfunction earlier than White patients. Patients of color have historically
been underrepresented in clinical trials of MS disease-modifying
therapies.
Low vitamin D levels have been associated with an increased risk of MS,
and although the role of supplementation has not been clearly defined, it is
often considered in clinical practice. Consensus has not yet been reached
regarding goal vitamin D levels for patients with MS, but levels of at least
40 ng/mL to 60 ng/mL have been suggested. Smoking has been associated
with both risk of MS and disease course, and education regarding
MS-specific risks of smoking may influence the likelihood of cessation.
Another modifiable risk factor for MS that did not apply in this case
includes obesity, especially in adolescence and childhood. Abdominal
obesity in particular may have associations with the degree of MS-related
disability. Nonmodifiable MS risk factors include Epstein-Barr virus (EBV)
infection (at least currently, given widespread seropositivity in the general
population and lack of definitive treatment for EBV) and genotype.
998 AUGUST 2022
Copyright © American Academy of Neurology. Unauthorized reproduction of this article is prohibited.
transgender. Only 62.5% of 25 transgender patients reported that their provider
was aware of their gender identity, and provider awareness of gender identity
was associated with increased patient satisfaction. Patients who identified as
transgender were also less comfortable discussing sexual health with their
providers.108 Sexual dysfunction is common in patients with MS in general, may
be at least indirectly associated with mood symptoms,109 and is rarely asked
about by physicians.110 Better physician understanding regarding sexual
FIGURE 1-2
Imaging from the patient in CASE 1-1. Brain axial (A) and sagittal (B) fluid-attenuated inversion
recovery (FLAIR) MRI demonstrating periventricular lesions consistent with multiple
sclerosis. Axial T2-weighted MRI (C) of cervical spine demonstrating a demyelinating lesion.
CONTINUUMJOURNAL.COM 999
Copyright © American Academy of Neurology. Unauthorized reproduction of this article is prohibited.
MS EPIDEMIOLOGY AND PATHOPHYSIOLOGY
KEY POINTS orientation and gender identity may be an opportunity for optimization of
comprehensive MS care, and more data are needed regarding LGBTQAI-specific
● Physician awareness
regarding patients’ gender
considerations in MS.
identity and sexual
orientation is an important Socioeconomic Status
opportunity for improved Socioeconomic factors, including income, employment, access to health
comprehensive care and
insurance, and education are increasingly recognized as contributors to clinical
patient satisfaction.
outcomes in MS.111 Lower socioeconomic status has been associated with worse
● Socioeconomic factors disability,112-114 and adjusting for socioeconomic status attenuates some racial
contribute to MS outcomes, differences in degree of disability.95 Lower socioeconomic status has also been
and costs of care related to associated with worse MS-related symptoms including fatigue, depression, and
MS have steadily increased.
Many patients with MS anxiety.110,113 Nearly three-fourths of patients at one MS center experienced
experience financial worry, financial worry, and cost of care contributed to nonadherence to clinic visits,
and costs may affect patient imaging, or medications in more than one-third of patients at the same center.115,116
adherence and quality On a larger population level, the 2019 total estimated US economic burden
of life.
of MS was $85 billion, and prescription medications (DMT and non-DMT)
accounted for almost $40 billion of direct MS medical costs.117 In recent years,
costs of DMT have risen significantly, drastically out of proportion to the rate of
inflation, and far outpace spending for clinical services.118 Costs of care rise with
increasing disability, and in prior meta-analyses MS ranked second only to
congestive heart failure in direct cost of care for chronic medical conditions.119
Cooperative efforts between physicians and health insurance plans may provide
opportunities for improvements in cost stewardship as well as equity and quality
of care.120
CONCLUSION
MS occurs in patients of all backgrounds and can develop in childhood through
adulthood. The prevalence of MS has increased in recent decades, and the
economic impacts of the disease on both individual patients and the health care
system at large are considerable. MS pathogenesis likely results from complex
interactions between genetic and environmental risk factors. Recent decades
have yielded marked advances regarding understanding of MS disease processes,
and treatment options have also significantly expanded. Still, much remains to be
elucidated regarding MS disease mechanisms, including the importance of
individual variation in inflammatory dysfunction, early and sustained impact of
risk factor and comorbid disease mitigation, and pathobiologic differences
between relapsing and progressive disease. Further understanding of these areas
will have important and meaningful implications for disease prevention and
individual therapeutic options. Future studies are needed, especially regarding
the discussed unique subgroups of patients with MS who have historically been
underrepresented in MS-related research and clinical trials.
REFERENCES
1 Wallin M, Culpepper W, Campbell J, et al. The 2 Geladaris A, Häusler D, Weber M. Microglia: the
prevalence of MS in the United States: a missing link to decipher and therapeutically
population-based estimate using health claims control MS progression? Int J Mol Sci 2021;22(7):
data. Neurology 2019;92(10):e1029-e1040. doi: 3461. doi:10.3390/ijms22073461
10.1212/WNL.0000000000007035
1000 AUGUST 2022
Copyright © American Academy of Neurology. Unauthorized reproduction of this article is prohibited.
3 Grzegorski T, Losy J. Multiple sclerosis—the 17 Kamma E, Lasisi W, Libner C, et al. Central
remarkable story of a baffling disease. nervous system macrophages in progressive
Rev Neurosci 2019;30(5):511-526. doi:10.1515/ multiple sclerosis: relationship to
revneuro-2018-0074 neurodegeneration and therapeutics.
J Neuroinflammation 2022;19:45. doi:10.1186/
4 Firth D. The case of Augustus d’Este (1794-1848):
s12974-022-02408-y
the first account of disseminated sclerosis:
section of the history of medicine. Proc R Soc 18 Luchinetti C, Bruck W, Parisi J, et al.
Med 1941;34(7):381-384. Heterogeneity of multiple sclerosis lesions:
implications for the pathogenesis of
5 Cree B, Khan O, Bourdette D, et al. Clinical
demyelination. Ann Neurol 2000;47(6):707-717.
characteristics of African Americans vs
doi:10.1002/1531-8249(200006)47:6
Caucasian Americans with multiple sclerosis.
Neurology 2004;63(11):2039-2045. doi:10.1212/01. 19 Lassmann H. Pathogenic mechanisms associated
wnl.0000145762.60562.5d with different clinical courses of multiple
sclerosis. Front Immunol 2019;9:3116. doi:10.3389/
6 Langer-Gould A, Brara S, Beaber B, Zhang J.
fimmu.2018.03116
Incidence of multiple sclerosis in multiple racial
and ethnic groups. Neurology 2013;80(19): 20 Tsouki F, Williams A. Multifaceted involvement of
1734-1739. doi:10.1212/WNL.0b013e3182918cc2 microglia in gray matter pathology in multiple
sclerosis. Stem Cells 2021;39:993-1007. doi:
7 Dendrou CA, Fugger L, Friese MA.
10.1002/stem.3374
Immunopathology of multiple sclerosis. Nat Rev
Immunol 2015;15(9):545-558. doi:10.1038/nri3871 21 Lucchinetti C, Popescu B, Bunyan R, et al.
Inflammatory cortical demyelination in early
8 Wagner CA, Roque PJ, Goverman JM. Pathogenic
multiple sclerosis. N Engl J Med 2011;365(23):
T cell cytokines in multiple sclerosis. J Exp Med
2188-2197. doi:10.1056/NEJMoa1100648
2020;217(1):e20190460. doi:10.1084/jem.20190460
22 Eshagi A, Prados F, Brownlee WJ. Deep gray
9 Comi G, Bar-Or A, Lassmann H, et al. Role of B
matter volume loss drives disability worsening in
cells in multiple sclerosis and related disorders.
multiple sclerosis. Ann Neurol 2018;83:210-222.
Ann Neurol 2021;89(1):13-23. doi:10.1002/
doi:10.1002/ana.25145
ana.25927
23 Calabrese M, Poretto V, Favaretto A, et al.
10 Bar-Or A, Fawaz L, Fan B, et al. Abnormal B-cell
Cortical lesion load associates with progression
cytokine responses a trigger of T-cell-mediated
of disability in multiple sclerosis. Brain 2012;
disease in MS? Ann Neurol 2010;67(4):452-461.
135(Pt 10):2952-2961. doi:10.1093/brain/aws246
doi:10.1002/ana.21939
24 Correale J, Gaitan MI, Ysrraelit MC, Fiol MP.
11 Correale J, Farez M, Razzitte G, et al. Helminth
Progressive multiple sclerosis: from pathogenic
infections associated with multiple sclerosis
mechanisms to treatment. Brain 2017;140:
induce regulatory B cells. Ann Neurol 2008;64(2):
527-546. doi:10.1093/brain/aww258
187-199. doi:10.1002/ana.21438
25 Cree BAC, Arnold DL, Chataway J, et al.
12 Magliozzi R, Howell O, Vora A, et al. Meningeal
Secondary progressive multiple sclerosis: new
B-cell follicles in secondary progressive multiple
insights. Neurology 2021;97(8):378-388. doi:
sclerosis associate with early onset of disease
10.1212/WNL.0000000000012323
and severe cortical pathology. Brain 2007;
130(Pt 4):1089-1104. doi:10.1093/brain/awm038 26 Kearney H, Altmann DR, Samson RS, et al.
Cervical cord lesion load is associated with
13 Lisak RP, Benjamins JA, Nedelkoska L, et al.
disability independently from atrophy in MS.
Secretory products of multiple sclerosis B cells
Neurology 2015;84:367-373. doi:10.1212/
are cytotoxic to oligodendroglia in vitro.
WNL.0000000000001186
J Neuroimmunol 2012;246(1-2):85-95. doi:10.1016/j.
jneuroim.2012.02.015 27 Schlaeger R, Papinutto N, Zhu AH, et al.
Association between thoracic spinal cord gray
14 Guerrero BL, Sicotte NL. Microglia in multiple
matter atrophy and disability in multiple
sclerosis: friend or foe? Front Immunol 2020;11:
sclerosis. JAMA Neurol 2015;72(8):897-904. doi:
374. doi:10.3389/fimmu.2020.00374
10.1001/jamaneurol.2015.0993
15 Zrzavy T, Hametner S, Wimmer I, et al. Loss of
28 Tremlett H, Zhu F, Ascherio A, Munger K. Sun
‘homeostatic’ microglia and patterns of their
exposure over the life course and associations
activation in active multiple sclerosis. Brain 2017;
with multiple sclerosis. Neurology 2018;90(14):
140(7):1900-1913. doi:10.1093/brain/awx113
e1191-e1199. doi:10.1212/WNL.0000000000005257
16 Lassmann H, Horssen J, Mahad D, et al.
29 Sebastian P, Cherbuin N, Barcellos LF, et al.
Progressive multiple sclerosis: pathology and
Association between time spent outdoors and
pathogenesis. Nat Rev Neurol 2012;8(11):647-656.
risk of multiple sclerosis. Neurology 2022;98:
doi:10.1038/nrneurol.2012.168
e267-e278. doi:10.1212/WNL.0000000000013045
30 Lucas R, Ponsonby A, Dear K, et al. Sun exposure
and vitamin D are independent risk factors for
CNS demyelination. Neurology 2011;76(6):
540-548. doi:10.1212/WNL.0b013e31820af93d
CONTINUUMJOURNAL.COM 1001
Copyright © American Academy of Neurology. Unauthorized reproduction of this article is prohibited.
MS EPIDEMIOLOGY AND PATHOPHYSIOLOGY
31 Yeh W, Gresle M, Jokubaitis V, et al. 44 Clinicaltrialsgov. Efficacy of cholecalciferol
Immunoregulatory effects and therapeutic (vitamin D3) for delaying the diagnosis of MS
potential of vitamin D in multiple sclerosis. Br J after a clinically isolated syndrome (D-Lay-MS).
Pharmacol 2020;177(18):4113-4133. doi:10.1111/ Updated January 10, 2022. Accessed June 6,
bph.15201 2022. clinicaltrials.gov/ct2/show/NCT01817166
32 Sintzel M, Rametta M, Reder A, et al. Vitamin D 45 Galior K, Grebe S, Singh R, et al. Development of
and multiple sclerosis: a comprehensive review. vitamin D toxicity from overcorrection of vitamin
Neurol Ther 2018;7(1):59-85. doi:10.1007/s40120- D deficiency: a review of case reports. Nutrients
017-0086-4 2018;10(8):953. doi:10.3390/nu10080953
33 National Institutelse of Health. Vitamin D fact 46 Holick M, Binkley N, Bischoff-Ferrari H, et al.
sheet for health care professionals. Accessed Evaluation, treatment, and prevention of vitamin
May 12, 2022. ods.od.nih.gov/factsheets/ D deficiency: an Endocrine Society Clinical
VitaminD-HealthProfessional/ Practice Guideline. J Clin Endocrinol Metab 2011;
96(7):1911-1930. doi:10.1210/jc.2011-0385
34 Miclea A, Bagnoud M, Chan A, Hoepner R. A brief
review of the effects of vitamin D on multiple 47 Shoemaker T, Mowry E. A review of vitamin D
sclerosis. Front Immunol 2020;11:781. doi:10. supplementation as disease-modifying therapy.
3389/fimmu.2020.00781 Mult Scler 2018;24(1):6-11. doi:10.1177/
1352458517738131
35 Munger K, Zhang S, O’Reilley E, et al. Vitamin D
intake and incidence of multiple sclerosis. 48 Olsson T, Barcellos L, Alfredsson L, et al.
Neurology 2004;62(1):60-65. doi:10.1212/01. Interactions between genetic, lifestyle and
wnl.0000101723.79681.38 environmental risk factors for multiple sclerosis.
Nat Rev Neurol 2017;13(1):25-36. doi:10.1038/
36 Munger K, Levin L, Hollis B, et al. Serum
nrneurol.2016.187
25-hydroxyvitamin D levels and risk of multiple
sclerosis. JAMA 2006;296(23):2832-2838. doi:10. 49 Waubant E, Lucas R, Mowry E, et al.
1001/jama.296.23.2832 Environmental and genetic risk factors for MS: an
integrated review. Ann Clin Transl Neurol 2019;
37 Martinelli V, Dalla Costa G, Colombo B, et al.
6(9):1905-1922. doi:10.1002/acn3.50862
Vitamin D levels and risk of multiple sclerosis in
patients with clinically isolated syndrome. Mult 50 Meir Jacobs B, Noyce A, Bestwick J, et al.
Scler 2014;20(2):147-155. doi:10.1177/ Gene-environment interactions in multiple
1352458513494959 sclerosis: a UK Biobank study. Neurol
Neuroimmunol Neuroinflamm 2021;8(4):e1007.
38 Simpson S, Taylor B, Blizzard L, et al. Higher
doi:10.1212/NXI.0000000000001007
25-hydroxyvitamin D is associated with lower
relapse risk in multiple sclerosis. Ann Neurol 2010; 51 Langer-Gould A, Wu J, Lucas R, et al. Epstein-Barr
68(2):193-203. doi:10.1002/ana.22043 virus, cytomegalovirus, and multiple sclerosis
susceptibility: a multiethnic study. Neurol 2017;
39 Graves J, Barcellos L, Krupp L, et al. Vitamin D
89(13):1330-1337. doi:10.1212/WNL.
genes influence MS relapses in children. Mult
0000000000004412
Scler 2020;26(8):894-901. doi:10.1177/
1352458519845842 52 Bjornevik K, Cortese M, Healy BC, et al.
Longitudinal analysis reveals high prevalence of
40 Bhargava P, Steele S, Waubant E, et al. Multiple
Epstein-Barr virus associated with multiple
sclerosis patients have a diminished serologic
sclerosis. Science 2022;375:296-301. doi:10.1126/
response to vitamin D supplementation
science.abj8222
compared to healthy controls. Mult Scler 2016;
22(6):753-760. doi:10.1177/1352458515600248 53 Belbasis L, Bellou V, Evangelou E, et al.
Environmental risk factors and multiple sclerosis:
41 Boltjes R, Knippenberg S, Gerlach O, et al.
an umbrella review of systematic reviews and
Vitamin D supplementation in multiple sclerosis:
meta-analyses. Lacet Neurol 2015;14(3):263-273.
an expert opinion based on the review of current
doi:10.1016/S1474-4422(14)70267-4
evidence. Expert Rev Neurother 2021;21(6):
715-725. doi:10.1080/14737175.2021.1935878 54 Marcucci S, Obeidat A. EBNA1, EBNA2, and
EBNA3 link Epstein-Barr virus and
42 Jagannath V, Filippini G, Di Pietrantonj C, et al.
hypovitaminosis D in multiple sclerosis
Vitamin D for the management of multiple
pathogenesis. J Neuroimmunol 2020;339:577116.
sclerosis. Cochrane Database Syst Rev 2018;9(9):
doi:10.1016/j.jneuroim.2019.577116
CD008422. doi:10.1002/14651858.CD008422.
pub3 55 Lanz T, Brewer RC, Ho PP, et al. Clonally
expanded B cells in multiple sclerosis bind EBV
43 Bhargava P, Cassard S, Steele SU, et al. The
EBNA1 and GlialCAM. Nature 2022;63:321-327.
vitamin D to ameliorate multiple sclerosis
doi:10.1038/s41586-022-04432-7
(VIDAMS) trial: study design for a multicenter,
randomized, double-blind controlled trial of 56 Moreno M, Or-Geva N, Aftab B, et al. Molecular
vitamin D in multiple sclerosis. Contemp Clin signature of Epstein-Barr virus infection in MS
Trials 2014;39(2):288-293. doi:10.1016/j.cct.2014. brain lesions. Neurol Neuroimmunol
10.004 Neuroinflamm 2018;5(4):e466. doi:10.1212/NXI.
0000000000000466
1002 AUGUST 2022
Copyright © American Academy of Neurology. Unauthorized reproduction of this article is prohibited.
57 Hassani A, Corboy JR, Al-Salam S, Khan G. 70 Sender R, Fuchs S, Milo R, et al. Revised
Epstein-Barr virus is present in the brain of most estimates for the number of human and bacteria
cases of multiple sclerosis and may engage more cells in the body. PLoS Biol 2016;14(8):1002533.
than just B cells. PLoS One 2018;13(2):e0192109. doi:10.1371/journal.pbio.1002533
doi:10.1371/journal.pone.0192109
71 Mowry EM, Glenn JD. The dynamics of the gut
58 Hawkes C. Smoking is a risk factor for multiple microbiome in multiple sclerosis in relation to
sclerosis: a metanalysis. Mult Scler 2007;13(5): disease. Neurol Clin 2018;36(1):185-196.
610-615. doi:10.1177/1352458506073501 doi:10.1016/j.ncl.2017.08.008
59 Ramanujam R, Hedstrom A, Manouchehrinia A, 72 Cryan J, O’Riordan K, Sandhu K, et al. The gut
et al. Effect of smoking cessation on multiple microbiome in neurological disorders. Lancet
sclerosis prognosis. JAMA Neurol 2015;72(10): Neurol 2020;19(2):179-194. doi:10.1016/S1474-
1117-1123. doi:10.1001/jamaneurol.2015.1788 4422(19)30356-4
60 Barzegar M, Najdaghi S, Ashari-Safavi A, et al. 73 Dopkins N, Nagarkatti P, Nagarkatti M, et al.
Early predictors of conversion to secondary The role of gut microbiome and associated
progressive multiple sclerosis. Mult Scler Relat metabolome in the regulation of
Disord 2021;54:103115. doi:10.1016/j.msard.2021. neuroinflammation in multiple sclerosis and its
103115 implications in attenuating chronic inflammation
in other inflammatory and autoimmune
61 Petersen E, Oturai A, Koch-Henriksen N, et al.
disorders. Immunology 2018;154(2):178-185. doi:
Smoking affects the interferon beta treatment
10.1111/imm.12903
response in multiple sclerosis. Neurol 2018;90(7):
e593-e600. doi:10.1212/WNL.0000000000004949 74 Sarasella M, Mendozzi L, Rossi V, et al.
Immunological and clinical effect of diet
62 Petersen E, Bach Søndergaard H, Laursen J, et al.
modulation of the gut microbiome in multiple
Smoking is associated with increased disease
sclerosis patients: a pilot study. Front Immunol
activity during natalizumab treatment in multiple
2017;8:1391. doi:10.3389/fimmu.2017.01391
sclerosis. Mult Scler 2019;25(9):1298-1305. doi:10.
1177/1352458518791753 75 Yadav V, Marracci G, Kim E, et al. Low-fat,
plant-based diet in multiple sclerosis: a
63 Hedstrom A, Olsson T, Alfredsson L, et al.
randomized controlled trial. Mult Scler Relat
Smoking is a major preventable risk factor for
Disord 2016;9:80-90. doi:10.1016/j.msard.2016.07.
multiple sclerosis. Mult Scler J 2016;22(8):
001
1021-1026. doi:10.1177/1352458515609794
76 Brenton JN, Banwell B, Bergqvist AGC, et al. Pilot
64 Hunter A, Grech L, Borland R, et al. Barriers and
study of a ketogenic diet in relapsing-remitting
motivators for tobacco smoking cessation in
MS. Neurol Neuroimmunol Neuroinflamm 2019;
people with multiple sclerosis. Mult Scler Relat
6(4):e565. doi:10.1212/NXI.0000000000000565
Disord 2021;54:103085. doi:10.1016/j.
msard.2021.103085 77 Fitzgerald K, Tyry T, Salter A, et al. Diet quality is
associated with disability and symptom severity
65 Brooker C, Goldman M, Tingen R, et al. Smoking
in multiple sclerosis. Neurology 2018;90(1):e1-e11.
cessation considerations for people with
doi:10.1212/WNL.0000000000004768
multiple sclerosis. Innov Pharm 2020;11(2):
10.24926/iip.v11i2.3210. doi:10.24926/iip.v11i2.3210 78 Salter A, Kowalec K, Fitzgerald K, et al.
Comorbidity is associated with disease activity in
66 Liu Z, Zhang T, Yu J, et al. Excess body weight
MS: findings from the CombiRx trial. Neurology
during childhood and adolescence is associated
2020;95(5):e446-e456. doi:10.1212/
with the risk of multiple sclerosis: a meta-
WNL.0000000000010024
analysis. Neuroepidemiology 2016;47(2):103-108.
doi:10.1159/000450854 79 Nelson L, Bourdette D. Two decades of research:
time to incorporate comorbidity management
67 Brenton N, Woolbright E, Briscoe-Abath C, et al.
into the care of MS? Neurology 2020;95(5):
Body mass index trajectories in pediatric multiple
193-194. doi:10.1212/WNL.0000000000010036
sclerosis. Dev Med Child Neurol 2019;61(11):
1289-1294. doi:10.1111/dmcn.14233 80 Berrigan LI, Fisk JD, Patten SB, et al. Health-
related quality of life in multiple sclerosis: direct
68 Fitzgerald K, Salter A, Tyry T, et al. Measures of
and indirect effects of comorbidity. Neurology
general and abdominal obesity and disability
2016;86(15):1417-1424. doi:10.1212/WNL.
severity in a large population of people with
0000000000002564
multiple sclerosis. Mult Scler 2020;26(8):
976-986. doi:10.1177/1352458519845836 81 Marrie R, Patten S, Tremlett H, et al. Sex
differences in comorbidity at diagnosis of
69 Hedstrom A, Brenner N, Butt J, et al. Overweight/
multiple sclerosis: a population-based study.
obesity in young adulthood interacts with
Neurology 2016;86(14):1279-1286. doi:10.1212/
aspects of EBV infection in MS etiology. Neurol
WNL.0000000000002481
Neuroimmunol Neuroinflamm 2021;8(1):e912.
doi:10.1212/NXI.0000000000000912 82 Marrie RA, Rudick R, Horwitz R, et al. Vascular
comorbidity is associated with more rapid
disability progression in multiple sclerosis.
Neurology 2010;30;74(13):1041-1047. doi:10.1212/
WNL.0b013e3181d6b125.
CONTINUUMJOURNAL.COM 1003
Copyright © American Academy of Neurology. Unauthorized reproduction of this article is prohibited.
MS EPIDEMIOLOGY AND PATHOPHYSIOLOGY
83 Conway D, Thompson N, Cohen J. Influence of 96 Gray-Roncal K, Fitzgerald KC, Zhovtis Ryerson L,
hypertension, diabetes, hyperlipidemia, and et al. Association of disease severity and
obstructive lung disease on multiple sclerosis socioeconomic status in Black and White
disease course. Mult Scler 2017;23:277-285. Americans with multiple sclerosis. Neurology
doi:10.1177/1352458516650512 2021;97(9):e881-e889. doi:10.1212/
WNL.0000000000012362
84 McKay KA, Tremlett H, Fisk JD, et al. Psychiatric
comorbidity is associated with disability 97 Caldito N, Saidha S, Sotirchos E, et al. Brain and
progression in multiple sclerosis. Neurology retinal atrophy in African-Americans versus
2018;90(15):e1316-e1323. doi:10.1212/WNL. Caucasian-Americans with multiple sclerosis: a
0000000000005302 longitudinal study. Brain 2018;141(11):3115-3129.
doi:10.1093/brain/awy245
85 Tarrants M, Oleen-Burkey M, Castelli-Haley J,
Lage MJ. The impact of comorbid depression on 98 Amezcua L, McCauley JL. Race and ethnicity on
adherence to therapy for multiple sclerosis. Mult MS presentation and disease course. Mult Scler
Scler Int 2011;2011:271321. doi:10.1155/2011/271321 2020;26(5):561-567. doi:10.1177/1352458519887328
86 Mohr DC, Goodkin DE, Likosky W, et al. Treatment 99 Langer-Gould A, Brara SM, Beaber BE, Zhang J.
of depression improves adherence to interferon The incidence of clinically isolated syndrome in a
beta-1b therapy for multiple sclerosis. Arch multi-ethnic cohort. J Neurol 2014;261:1349-1355.
Neurol 1997;54(5):531-533. doi:10.1001/archneur. doi:10.1007/s00415-014-7349-0
1997.00550170015009
100 Amezcua L, Oksenberg JR, McCauley JL. MS in
87 Zhang T, Tremlett H, Zhu F, et al. Effects of self-identified Hispanic/Latino individuals living
physical comorbidities on disability progression in the US. Mult Scler J Exp Transl Clin 2017;3(3):
in multiple sclerosis. Neurology 2018;90(5): 2055217317725103. doi:10.1177/2055217317725103
e419-e427. doi:10.1212/WNL.0000000000004885
101 Ventura RE, Antezana AO, Bacon T, Kister I.
88 Zhang T, Tremlett H, Leung S, et al. Examining the Hispanic Americans and African Americans
effects of comorbidities on disease-modifying with multiple sclerosis have more severe
therapy use in multiple sclerosis. Neurology 2016; disease course than Caucasian Americans.
86(14):1287-1295. doi:10.1212/WNL. Mult Scler 2017;23(11):1554-1557. doi:10.1177/
0000000000002543 1352458516679894
89 Goldman M, Koenig S, Engel C, et al. 102 Amezcua L, Beecham AH, Delgado SR, et al.
Glucocorticoid-associated blood glucose Native ancestry is associated with optic neuritis
response and MS relapse recovery. Neurol and age of onset in Hispanics with multiple
Neuroimmunol Neuroinflamm 2017;4(5):e378. doi: sclerosis. Ann Clin Transl Neurol 2018;5(11):
10.1212/NXI.0000000000000378 1362-1371. doi:10.1002/acn3.646
90 Khan O, Williams MJ, Amezcua L, et al. Multiple 103 Romero-Hidalgo S, Flores-Rivera J, Rivas-Alonso,
sclerosis in US minority populations: clinical et al. Native American ancestry significantly
practice insights. Neurol Clin Pract 2015;5(2): contributes to neuromyelitis optica susceptibility
132-142. doi:10.1212/CPJ.0000000000000112 in the admixed Hispanic population. Sci Rep
2020;10:13706. doi:10.1038/s41598-020-69224-3
91 Wallin M, Culpepper W, Coffman P, et al. The Gulf
War era multiple sclerosis cohort: age and 104 Saadi A, Himmelstein DU, Woolhandler S, Mejia
incidence rates by race, sex and service. Brain NI. Racial disparities in neurologic health care
2012;135(Pt 6):1778-1785. doi:10.1093/brain/ access and utilization in the United States.
aws099 Neurology 2017;88(24):2268-2275. doi:10.1212/
WNL.0000000000004025
92 Langer-Gould A, Gonzales E, Smith J, Li B, Nelson
L. Racial and ethnic disparities in multiple 105 Cree B, Al-Sabbagh A, Bennett R, et al. Response
sclerosis prevalence [published ahead of print to interferon beta-1a treatment in African
April 28, 2022]. Neurology. doi:10.1212/ American multiple sclerosis patients. Arch
WNL.0000000000200151 Neurol 2005;62(11):1681-1683. doi:10.1001/
archneur.62.11.1681
93 Rivas-Rodríguez E, Amezcua L. Ethnic
considerations and multiple sclerosis disease 106 Avasarala J. Inadequacy of clinical trial designs
variability in the United States. Neurol Clin 2018; and data to control for the confounding impact
36(1):151-162. doi:10.1016/j.ncl.2017.08.007 of race/ethnicity in response to treatment in
multiple sclerosis. JAMA Neurol 2014;71(8):
94 Kimbrough DJ, Sotirchos ES, Wilson JA, et al.
943-944. doi:10.1001/jamaneurol.2014.79
Retinal damage and vision loss in African
American multiple sclerosis patients. Ann Neurol 107 Onuorah H, Charron O, Meltzer E, et al,
2015;77(2):228-236. doi:10.1002/ana.24308 Enrollment of non-white participants and
reporting of race and ethnicity in phase III trials of
95 Marrie R, Cuter G, Tyry T, et al. Does multiple
multiple sclerosis DMTs. Neurology 2022;98:
sclerosis-associated disability differ between
e880-e892. doi:10.1212/WNL.0000000000013230
races? Neurology 2006;66(8):1235-1240. doi:10.
1212/01.wnl.0000208505.81912.82
1004 AUGUST 2022
Copyright © American Academy of Neurology. Unauthorized reproduction of this article is prohibited.
108 Khayambashi S, Salter A, Tyry T, et al. Gender 114 Calocer F, Dejardin O, Kwiatkowski A, et al.
identity and sexual orientation affect health care Socioeconomic deprivation increases the risk of
satisfaction, but not utilization. Mult Scler Relat disability in multiple sclerosis patients. Mult Scler
Disord 2020;37:101440. doi:10.1016/j. Relat Disord 2020;40:101930. doi:10.1016/j.
msard.2019.101440 msard.2020.101930
109 Young C, Tennant A, TONiC Study Group. Sexual 115 Sadigh G, Lava N, Switchenko J, et al. Patient-
functioning in multiple sclerosis: relationships reported financial toxicity in multiple sclerosis:
with depression, fatigue and physical function. predictors and association with care
Mult Scler 2017;23(9):1268-1275. doi:10.1177/ non-adherence. Mult Scler 2021;27(3):453-464.
1352458516675749 doi:10.1177/1352458520913977
110 Wang G, Marrie RA, Fox RJ, et al. Treatment 116 Sadigh G, Switchenko J, Lava N, et al. Longitudinal
satisfaction and bothersome bladder, bowel, changes of financial hardship in patients with
sexual symptoms in multiple sclerosis. Mult Scler multiple sclerosis. Mult Scler Relat Disord 2021;
Relat Disord 2018;20:16-21. doi:10.1016/j. 53:103037. doi:10.1016/j.msard.2021.103037
msard.2017.12.006
117 Bebo B, Cintina I, LaRocca N, et al. Economic
111 Wang Y, Tian F, Fitzgerald K, et al. Socioeconomic burden of multiple sclerosis in the United States:
status and race are correlated with affective estimate of direct and indirect costs. Neurology
symptoms in multiple sclerosis. Mult Scler Relat 2022;98:e1810-e1817. doi:10:1212/
Disord 2020;41:102010. doi:10.1016/j. WNL.0000000000200150.
msard.2020.102010
118 Hartung DM. Health economics of
112 Harding KE, Wardle M, Carruthers R, et al. disease-modifying therapy for multiple sclerosis
Socioeconomic status and disability progression in the United States. Ther Adv Neurol Disord 2021;
in multiple sclerosis: a multinational study. Neurol 14:1756286420987031. doi:10.1177/
2019;92(13):e1497-e1506. doi:10.1212/ 1756286420987031
WNL.0000000000007190
119 Adelman G, Rane SG, Villa KF, et al. The cost
113 Briggs FBS, Thompson NR, Conway DS, et al. burden of multiple sclerosis in the United States:
Prognostic factors of disability in relapsing a systematic review of the literature. J Med Econ
remitting multiple sclerosis. Mult Scler Relat 2013;16(5):639-647. doi:10.3111/
Disord 2019;30:9-16. doi:10.1016/j.msard.2019. 13696998.2013.778268
01.045
120 Langer-Gould A, Klocke S, Beaber B, et al.
Improving quality, affordability, and equity of
multiple sclerosis care. Ann Clin Transl Neurol
2020;8(4):980-991. doi:10.1002/acn3.51326
CONTINUUMJOURNAL.COM 1005
Copyright © American Academy of Neurology. Unauthorized reproduction of this article is prohibited.
You might also like
- S35 - Anil Kumar Pandey (J.K. Pathology) Near V Mart, Gandhi Ground, BADAUN243601 9058494498 / 8755328670Document6 pagesS35 - Anil Kumar Pandey (J.K. Pathology) Near V Mart, Gandhi Ground, BADAUN243601 9058494498 / 8755328670Satyabhan SinghNo ratings yet
- Pathology of Multiple Sclerosis: CNS & Neurological Disorders Drug Targets May 2012Document13 pagesPathology of Multiple Sclerosis: CNS & Neurological Disorders Drug Targets May 2012jhidalgomdNo ratings yet
- Multiple Sclerosis: Genetic Factors, Risk and PrevalenceDocument3 pagesMultiple Sclerosis: Genetic Factors, Risk and PrevalenceGusti TettaNo ratings yet
- Multiple Sclerosis, A Treatable DiseaseDocument7 pagesMultiple Sclerosis, A Treatable DiseaseMuhammad Imam NoorNo ratings yet
- JCM 10 05401Document17 pagesJCM 10 05401Rafael Vidal SanzNo ratings yet
- Ijms 22 07802 v2Document15 pagesIjms 22 07802 v2Wilder Gonzalez DiazNo ratings yet
- p2021b2 SampleDocument23 pagesp2021b2 SampleHgokarolNo ratings yet
- Thesis Multiple SclerosisDocument8 pagesThesis Multiple Sclerosislisathompsonportland100% (2)
- MS Overview PDFDocument19 pagesMS Overview PDFdracoscribdNo ratings yet
- Research Paper Outline On Multiple SclerosisDocument5 pagesResearch Paper Outline On Multiple Sclerosisfznn7hzd100% (1)
- Primer: Multiple SclerosisDocument27 pagesPrimer: Multiple SclerosisYabokuxtoriNo ratings yet
- Multiple SclerosisDocument22 pagesMultiple SclerosisInthe MOON youNo ratings yet
- Living with MS: A Comprehensive Guide for Patients and FamiliesFrom EverandLiving with MS: A Comprehensive Guide for Patients and FamiliesNo ratings yet
- Key Clinical Features of MSDocument5 pagesKey Clinical Features of MSdimitris698No ratings yet
- Karussis 2014Document9 pagesKarussis 2014Edison Chiriboga OrtegaNo ratings yet
- Alzheimer's Disease: Genes, Pathogenesis and Risk PredictionDocument7 pagesAlzheimer's Disease: Genes, Pathogenesis and Risk PredictionWindaNo ratings yet
- U.S. Department of Veterans AffairsDocument18 pagesU.S. Department of Veterans AffairsemiNo ratings yet
- Progresive Multiple Sclerosis Continuum 2022Document21 pagesProgresive Multiple Sclerosis Continuum 2022cuentoNo ratings yet
- Dementia Preventia, Intervention and Care - LANCETDocument34 pagesDementia Preventia, Intervention and Care - LANCETFernando lazzarettiNo ratings yet
- Understanding The Radiologist's Role in Evaluating Multiple Sclerosis - A Review of The Tip of The IcebergDocument30 pagesUnderstanding The Radiologist's Role in Evaluating Multiple Sclerosis - A Review of The Tip of The IcebergAnkita ShahNo ratings yet
- Demencia Continun 2022Document289 pagesDemencia Continun 2022RafaelNo ratings yet
- Epidemiology and Treatment of Multiple Sclerosis in Elderly PopulationsDocument14 pagesEpidemiology and Treatment of Multiple Sclerosis in Elderly PopulationsLütfiye ÇiftçiNo ratings yet
- Multiple SclerosisDocument14 pagesMultiple Sclerosisbrianpeterson000No ratings yet
- Optimizing Therapeutics in The Management of Patients With Multiple Sclerosis: A Review of Drug Efficacy, Dosing, and Mechanisms of ActionDocument12 pagesOptimizing Therapeutics in The Management of Patients With Multiple Sclerosis: A Review of Drug Efficacy, Dosing, and Mechanisms of ActionAndhita Satya Pratama GiovanniNo ratings yet
- Research Paper On Multiple Sclerosis FreeDocument4 pagesResearch Paper On Multiple Sclerosis Freeutwvgkxgf100% (1)
- The Potential of Stem Cell Therapy in Multiple Sclerosis Treatment - A ReviewDocument20 pagesThe Potential of Stem Cell Therapy in Multiple Sclerosis Treatment - A ReviewlucyadiraNo ratings yet
- Johnson 2019Document14 pagesJohnson 2019Mariel González.No ratings yet
- Hauser 2020Document13 pagesHauser 2020JesusNo ratings yet
- Activation of T-Cells-Major Key To Multiple SclerosisDocument14 pagesActivation of T-Cells-Major Key To Multiple Sclerosisbabansub9542No ratings yet
- Lambert-Eaton Myasthenic Syndrome and BotulismDocument19 pagesLambert-Eaton Myasthenic Syndrome and BotulismGabriela RusinNo ratings yet
- 2021 JAMA Diagnosis and Treatment of Multiple Sclerosis A ReviewDocument15 pages2021 JAMA Diagnosis and Treatment of Multiple Sclerosis A ReviewItz Hernandez GarciaNo ratings yet
- Lancet 2020Document34 pagesLancet 2020Javier ValeroNo ratings yet
- New Concepts in The Immunopathogenesis of Multiple SclerosisDocument11 pagesNew Concepts in The Immunopathogenesis of Multiple Sclerosisaedes_agNo ratings yet
- Inflammatory Demyelinating DiseasesDocument22 pagesInflammatory Demyelinating DiseaseslenushpopaNo ratings yet
- Immunologic Aspects of Multiple SclerosisDocument14 pagesImmunologic Aspects of Multiple SclerosisAhmed KumarNo ratings yet
- Multiple Sclerosis Neuroimmune Crosstalk and TherDocument19 pagesMultiple Sclerosis Neuroimmune Crosstalk and TherOUAISILISTEANORD CONSTANTANo ratings yet
- Dementia - Prevention - Intervention - and - Care - 2020 - Lancet - Commision 2Document34 pagesDementia - Prevention - Intervention - and - Care - 2020 - Lancet - Commision 2Jorge Sánchez DomínguezNo ratings yet
- Neuromuscular DiseaseDocument69 pagesNeuromuscular DiseaseDevi SiswaniNo ratings yet
- Research Assignment MSDocument6 pagesResearch Assignment MSSamantha BennNo ratings yet
- c4f - Multiple SclerosisDocument240 pagesc4f - Multiple Sclerosisstewpitt2No ratings yet
- Chinese Herbal Treatment For Multiple SclerosisDocument19 pagesChinese Herbal Treatment For Multiple Sclerosisbharata.ishaya8999No ratings yet
- Miastenia Gravis 1Document17 pagesMiastenia Gravis 1Hairunisa 0049No ratings yet
- Diagnosis and Treatment of Multiple Sclerosis3Document15 pagesDiagnosis and Treatment of Multiple Sclerosis3HgokarolNo ratings yet
- Multiple Sclerosis Phenotypes As A Continuum: The Role of Neurologic ReserveDocument11 pagesMultiple Sclerosis Phenotypes As A Continuum: The Role of Neurologic ReserveRiccardo TroiaNo ratings yet
- Lived Through Past Experienced Present Anticipated Future Understanding Existential Loss in The Context of Life Limiting IllnessDocument16 pagesLived Through Past Experienced Present Anticipated Future Understanding Existential Loss in The Context of Life Limiting Illnessfrancheskaam27No ratings yet
- Fast Facts: Multiple Sclerosis: A new era of disease modification and treatmentFrom EverandFast Facts: Multiple Sclerosis: A new era of disease modification and treatmentNo ratings yet
- Ni Hms 862943Document38 pagesNi Hms 862943Rhinaldy DanaraNo ratings yet
- Euro J of Neurology - 2018 - Dobson - Multiple Sclerosis A ReviewDocument14 pagesEuro J of Neurology - 2018 - Dobson - Multiple Sclerosis A ReviewPatySA2No ratings yet
- The Lancet Commissions: Executive SummaryDocument34 pagesThe Lancet Commissions: Executive SummaryKen CheungNo ratings yet
- PN0222 CF3 MSPrognosticationDocument5 pagesPN0222 CF3 MSPrognosticationArthur VasconcelosNo ratings yet
- Review: Multiple Sclerosis: Mechanisms and ImmunotherapyDocument27 pagesReview: Multiple Sclerosis: Mechanisms and ImmunotherapyAhmed KumarNo ratings yet
- Jamda: Original StudyDocument6 pagesJamda: Original StudyBenjamin RomeroNo ratings yet
- Multiple Sclerosis: Historic Perspective and Realization of Genetic Risk ContributionDocument8 pagesMultiple Sclerosis: Historic Perspective and Realization of Genetic Risk ContributionIuliana TomaNo ratings yet
- Chap 4 Multiple SclerosisDocument4 pagesChap 4 Multiple SclerosisSabina MoolyeNo ratings yet
- 10 1056@NEJMra1904794 PDFDocument17 pages10 1056@NEJMra1904794 PDFMартин ДончевNo ratings yet
- Progressive Multiple Sclerosis From Pathophysiology To Therapeutic StrategiesDocument18 pagesProgressive Multiple Sclerosis From Pathophysiology To Therapeutic StrategiesAnonymous QLadTClydkNo ratings yet
- Metabolic Syndrome, Mild Cognitive Impairment, and Dementia: A Meta-Analysis of Longitudinal StudiesDocument13 pagesMetabolic Syndrome, Mild Cognitive Impairment, and Dementia: A Meta-Analysis of Longitudinal StudiesMiguelySusy Ramos-RojasNo ratings yet
- A03 - Guideline 2016 Myelodysplastic Syndromes (MDS) - Jurnal Hong 2017Document5 pagesA03 - Guideline 2016 Myelodysplastic Syndromes (MDS) - Jurnal Hong 2017Muhammad BilalNo ratings yet
- Carta 2018Document9 pagesCarta 2018loloasbNo ratings yet
- GiovaniDocument9 pagesGiovaniRafaelNo ratings yet
- Neuroimmunology: Multiple Sclerosis, Autoimmune Neurology and Related DiseasesFrom EverandNeuroimmunology: Multiple Sclerosis, Autoimmune Neurology and Related DiseasesAmanda L. PiquetNo ratings yet
- Idh1, Idh2 Idh2 1p19q Co-Deletion, IDH1, IDH2, BRAF, EGFR AmplificationDocument12 pagesIdh1, Idh2 Idh2 1p19q Co-Deletion, IDH1, IDH2, BRAF, EGFR AmplificationNirbhay Singh Rathore100% (1)
- Immunization and Its Importance: A Literature ReviewDocument5 pagesImmunization and Its Importance: A Literature ReviewIJRASETPublicationsNo ratings yet
- SYEDA-FARIHA-AHSAN SECTION 02 BTE101 Mini-Report ASSIGNMENT-1Document8 pagesSYEDA-FARIHA-AHSAN SECTION 02 BTE101 Mini-Report ASSIGNMENT-1Sadia Tasmin LunaNo ratings yet
- Tissues and MembranesDocument2 pagesTissues and MembranesRav Evan VigillaNo ratings yet
- By: Alex B. Olivar JR., RN CHN Study Bullets Drug of Choice Disease Drug of ChoiceDocument5 pagesBy: Alex B. Olivar JR., RN CHN Study Bullets Drug of Choice Disease Drug of ChoiceAlexNo ratings yet
- Neural Control and Coordination - Shobhit NirwanDocument14 pagesNeural Control and Coordination - Shobhit NirwanSWASTIKA MALONo ratings yet
- Pathology Clinic Nasopharyngeal CarcinomaDocument2 pagesPathology Clinic Nasopharyngeal CarcinomaTukang Gali KuburNo ratings yet
- MicroPara Prelims 2nd Sem FinalDocument29 pagesMicroPara Prelims 2nd Sem FinalIvan MaximusNo ratings yet
- Biochemistry of Ageing AssignmentDocument9 pagesBiochemistry of Ageing Assignmentkalejaiye johnNo ratings yet
- Yersinia Pestis: Yersinia Pestis Yersinia Pestis (Formerly Pasteurella Pestis) Is A Gram-NegativeDocument14 pagesYersinia Pestis: Yersinia Pestis Yersinia Pestis (Formerly Pasteurella Pestis) Is A Gram-NegativeJames FranklinNo ratings yet
- Emerging Diseases of AvianDocument13 pagesEmerging Diseases of AvianAndres GilNo ratings yet
- National Guidelines For: HIV-1 Viral Load Laboratory TestingDocument86 pagesNational Guidelines For: HIV-1 Viral Load Laboratory TestingVINOD GUPTANo ratings yet
- Compilation of QuizzesDocument10 pagesCompilation of QuizzesElesis samaNo ratings yet
- SOL Review Answer SheetDocument15 pagesSOL Review Answer Sheetbrandonaniah7No ratings yet
- National Institute of Biomedical Imaging and Bioengineering: What Are Drug Delivery Systems?Document2 pagesNational Institute of Biomedical Imaging and Bioengineering: What Are Drug Delivery Systems?Irina RinnaNo ratings yet
- Application of siRNA TherapyDocument18 pagesApplication of siRNA TherapyAkash VIshwkarmaNo ratings yet
- Fen Otrimoxazole AlloDocument2 pagesFen Otrimoxazole AlloKristine AguilarNo ratings yet
- Genetic EngineeringDocument3 pagesGenetic EngineeringseshatcallingNo ratings yet
- Malabsorption Syndrome in ChickensDocument5 pagesMalabsorption Syndrome in ChickensŠhâh NawazNo ratings yet
- Wound Healing: Healing by First Intention (Primary Union)Document31 pagesWound Healing: Healing by First Intention (Primary Union)Muhammad Masoom AkhtarNo ratings yet
- Potential Targets For Antifungal Drug Discovery - Creative Biolabs - 1619624328334Document6 pagesPotential Targets For Antifungal Drug Discovery - Creative Biolabs - 1619624328334DicksonNo ratings yet
- Bioterrorism and Threat AssessmentDocument22 pagesBioterrorism and Threat Assessmentfares HACIB100% (1)
- Final Micro Module 1Document73 pagesFinal Micro Module 1Ahmed KerAtyNo ratings yet
- Microsoft Office PowerPoint Presentation NouDocument8 pagesMicrosoft Office PowerPoint Presentation NouStavarache LarisaNo ratings yet
- DirectPlex IFUDocument1 pageDirectPlex IFUNawed PerwezNo ratings yet
- Guidelines For Using HIV Testing Technologies in SurveillanceDocument43 pagesGuidelines For Using HIV Testing Technologies in SurveillancesomeoneyoucareNo ratings yet
- Cell Organelle Review WorksheetDocument4 pagesCell Organelle Review WorksheetMae SilogNo ratings yet
- The Bacterial Cell - Structures and FunctionsDocument27 pagesThe Bacterial Cell - Structures and FunctionsFRANCIS PAOLO CUADRANo ratings yet
- Complete Blood Count: DR: Mona Wagdy Ayad Assist Prof of Clinical PathologyDocument28 pagesComplete Blood Count: DR: Mona Wagdy Ayad Assist Prof of Clinical Pathologymarwanelsaeed1981No ratings yet